
Abstract
Background:
Some patients with metastatic differentiated thyroid cancer (DTC) lack iodine avidity and are therefore unsuitable for radioactive iodine (RAI) therapy. Limited experience suggests that single-agent selective mitogen-activated protein kinase (MAPK) pathway inhibitors can restore expression of the sodium–iodide symporter rendering RAI refractory (RAIR) DTC patients amenable to RAI therapy. The aim of this study was to assess the feasibility of mutation-guided MAPK-pathway blockade combined with thyroid hormone withdrawal (THW) for redifferentiation.
Methods:
This is a retrospective review of metastatic RAIR DTC and driver mutation in MAPK pathway, treated on a redifferentiation protocol. All patients had metastatic disease that had never been RAI-avid and/or imaging and biochemical progression despite treatment with RAI within the past 12 months. Patients with tumors harboring an NRAS mutation were treated with an MEK inhibitor (trametinib), and tumors with a BRAFV600E mutation with combined BRAF and MEK inhibition (dabrafenib and trametinib; or vemurafenib and cobimetinib) for four weeks. Thyrotropin stimulation was performed by THW for four weeks. Restoration of RAI uptake was determined by 124I positron emission tomography/computed tomography imaging. The response was assessed at least three months post-RAI.
Results:
From 2015 to 2017, six patients (age 45–70, four females) received redifferentiation therapy. Three patients had an NRAS mutation; two with follicular thyroid carcinoma (FTC) and one with a poorly differentiated thyroid carcinoma (PDTC); and three patients had a BRAFV600E mutation and papillary thyroid carcinoma (PTC). One NRAS and all BRAFV600E mutation cases demonstrated restoration of RAI uptake and proceeded to RAI therapy with a median follow-up of 16.6 months (range 13.5–42.3 months). The patient with an NRAS mutation and two of three patients with a BRAFV600E demonstrated partial imaging response beyond a three-month follow-up. Grade 3 adverse events (acneiform rash) were observed in two patients with NRAS mutations.
Conclusions:
Mutation-guided MAPK pathway inhibition with MEK inhibitor or a combination of BRAF inhibitor and MEK inhibitor under concurrent THW is a feasible and a promising strategy to redifferentiate RAIR DTC, thereby rendering them suitable for RAI therapy with satisfactory retention following treatment.
Introduction
Metastatic differentiated thyroid cancer (DTC) is associated with both morbidity and mortality (1). The ability of the metastatic tumor to retain iodine has made radioactive iodine (RAI) the mainstay of diagnosis and therapy of these patients (2). However, metastatic tumors in some patients do not concentrate RAI or become refractory to RAI therapy and are therefore classified as radioactive iodine-refractory (RAIR). The 10-year survival of the patients who achieved complete remission following RAI therapy is more than 90% and remains much better than the survival of the patients with initial RAI uptake, but with persisting abnormality following therapy or in those without initial RAI uptake, who have only a 10% survival rate (3). Two multitargeted tyrosine kinase inhibitors (mTKI), sorafenib and lenvatinib, have been approved by regulatory authorities for use in RAIR DTC (4,5). These novel agents have shown promising results with improvement in progression-free survival (PFS), but generally not in overall survival (OS) nor the quality of life (QOL). Furthermore, these agents are associated with numerous adverse events, require long-term treatment until progression, and are inevitably associated with the development of resistance in most cases (4,5). Therefore, there is an unmet need to develop effective well-tolerated treatment strategies for these patients.
The mitogen-activated protein kinase (MAPK) signaling pathway, which includes RAS, RAF, MEK, and ERK, regulates cell proliferation, differentiation, and apoptosis (6). Mutations in the RAF isoform BRAFV600E is often associated with a higher clinical stage, larger tumor size, extrathyroidal extension, lymph node metastases, the absence of iodine avidity, and treatment failure (7,8). While the BRAFV600E mutation is most common in papillary thyroid carcinoma (PTC) (9 –11), the incidence of NRAS mutation is higher in follicular thyroid carcinoma (FTC) (11). The Cancer Genome Atlas Research Network has reclassified PTC into BRAFV600E-like or RAS-like molecular subtypes (12). This classification may potentially be used to stratify the management of metastatic thyroid cancer (13). Mutations in these proteins activate the MAPK pathway and result in inhibition of thyroid-specific gene expression, including the sodium–iodide symporter and thyroid peroxidase, which are necessary for iodine uptake and organification, respectively (14,15). The presence of these mutations may also be associated with a reduced expression of the thyrotropin (TSH) receptor, limiting the impact of TSH-stimulated iodine uptake. Preclinical data indicate that inhibitors of either MEK or BRAF not only reduce their proliferative index but also partially restore thyroid-specific gene expression, rendering them susceptible to RAI therapy (16).
Pilot clinical studies, including a limited number of patients, assessed the efficacy of MAPK pathway inhibition with subsequent RAI therapy (redifferentiation protocol) in RAIR DTC (17,18). Although these studies showed encouraging results, there remain many unanswered questions regarding the optimal redifferentiation protocol. For instance, there is some concern about the use of recombinant human TSH (rhTSH) stimulation for the treatment of metastatic disease with studies indicating potential improvement in the therapeutic index of RAI therapy by using thyroid hormone withdrawal (THW) (19 –22). Other strategies include optimization of MAPK pathway inhibition by combination downstream signaling blockade.
In this study, we describe our initial experience of combined BRAF and MEK inhibition with concurrent THW in the redifferentiation protocol. Different aspects of this novel therapeutic strategy are discussed, including the duration and timing of the pathway inhibition in relation to RAI therapy and predictive markers of response beyond genotype.
Materials and Methods
Patients
Consecutive patients who underwent therapy with an RAI redifferentiation protocol at the Peter MacCallum Cancer Centre were reviewed retrospectively. Inclusion criteria were as follows: (i) histologically proven metastatic DTC; (ii) sufficient bone marrow (hemoglobin equal or above 90 g/L, neutrophil above 1.5 × 109/L, and platelet above 100 × 109/L) and renal function (creatinine clearance at least 40 mL/min); (iii) ECOG score 2 or below; and (iv) presence of a BRAFV600E or NRAS mutation. RAIR DTC was defined as follows: (i) minimal or no RAI avidity in some or all measurable sites of disease on appropriately performed RAI scans and/or (ii) imaging or biochemical progression despite RAI treatment within the past 12 months. For assessment of RAI avidity, either post-therapy 131I single-photon emission computed tomography (SPECT)/computed tomography (CT) or pretherapy 123I SPECT/CT or 124I positron emission tomography (PET)/CT was allowed. Conditions for appropriately conducted RAI scans included adequate TSH stimulation (>30 mU/L) and no exogenous iodine exposure in the preceding three months.
Each therapy was approved individually by the institutional tumor board under compassionate use criteria (Special Access Scheme—Category A). This study was approved by the Peter MacCallum Cancer Centre Ethics Committee (approval number 19/14R).
Mutation analysis
Amplicon-based next-generation sequencing was performed on DNA extracted from macro-dissected, formalin-fixed, paraffin-embedded tumor tissue followed by targeted sequencing on an Illumina MiSeq, 2 × 150 bp. Aligned reads and called variants were analyzed in PathOS (23). Variants were described according to the Human Genome Variation Society (HGVS) nomenclature version 2 (24).
Redifferentiation schedule
The redifferentiation protocol is detailed as below and summarized in Figure 1.
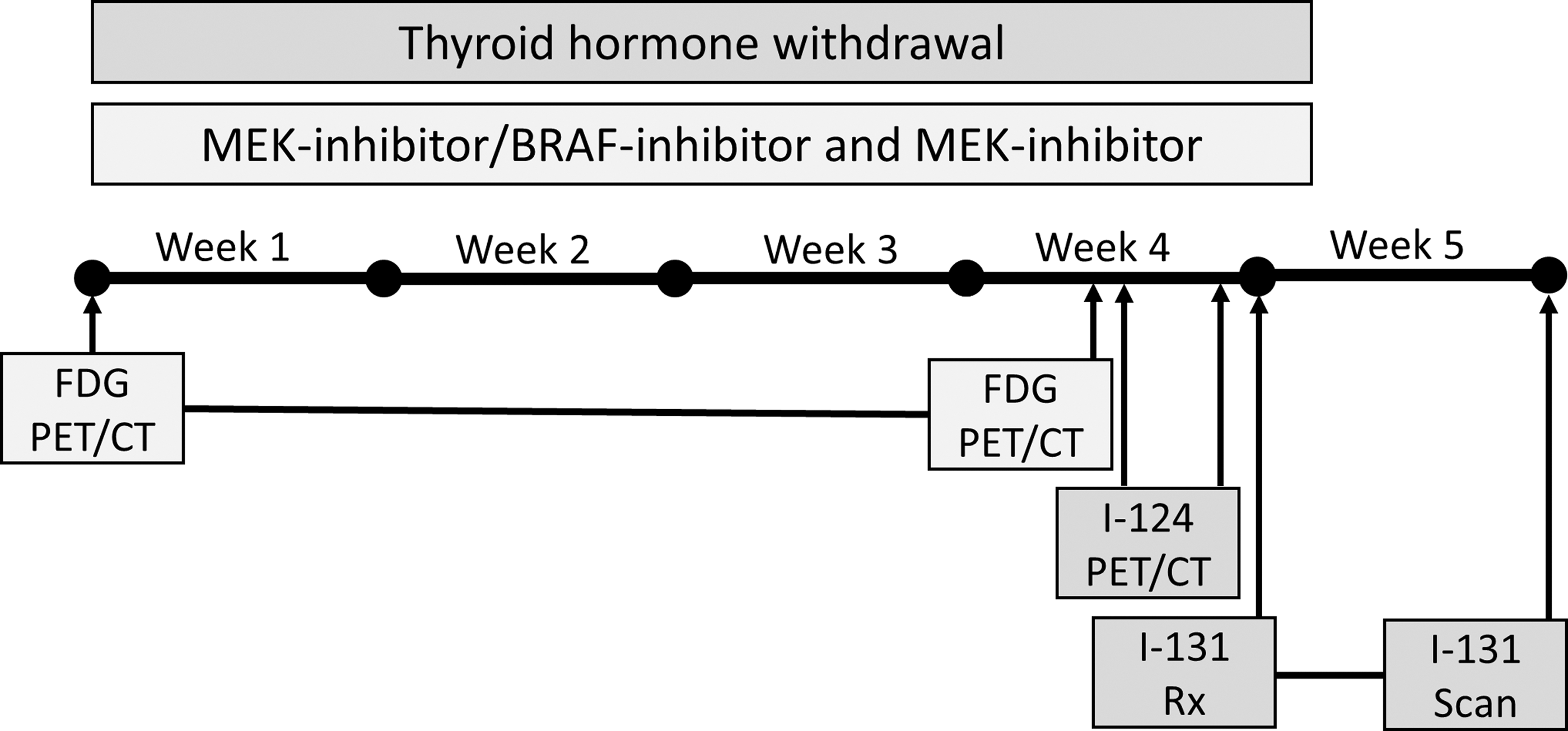
Schematic demonstration of redifferentiation protocol. CT, computed tomography; FDG, fluoro-2-deoxyglucose; PET, positron emission tomography.
Patient preparation and MAPK inhibition regimen
All included patients underwent four weeks of THW unless this was clinically contraindicated (n = 1). TSH stimulation was determined by blood sampling at approximately four weeks, and a TSH level >30 mU/L was considered satisfactory. If satisfactory TSH stimulation was not achieved with THW only (n = 1), and in the patient with THW contraindication, two injections of 0.9 mg rhTSH were administered intramuscularly 24 hours apart before RAI imaging and therapy.
The patients with NRAS mutations were treated with the MEK inhibitor trametinib (2 mg daily) for four weeks. The patients with a BRAFV600E mutation were treated with a combination therapy, including a BRAF inhibitor and an MEK inhibitor: dabrafenib (150 mg twice daily) and trametinib (2 mg daily), or vemurafenib (960 mg twice daily) and cobimetinib (60 mg daily) for four weeks. The choice of the agents used for the combination therapy was based on the access to these medications at the time of prescription. Treatment began four weeks from the expected date of RAI treatment, concurrent with THW. The patients were reviewed weekly and adverse events were recorded based on the Common Terminology Criteria for Adverse Events (CTCAE) version 4.
124I imaging protocol
Following confirmation of satisfactory TSH stimulation, two time point 124I PET/CT imagings were used to assess restoration of the iodine concentration at metastatic sites. For this, 1–2 MBq/kg body weight of 124I was injected intravenously (mean 120 MBq, range 80–210 MBq). Sequential CT and PET acquisition was then performed on an integrated PET/CT device (GE Discovery PET/CT 690 or GE Discovery 710; GE Healthcare, Milwaukee, WI). The CT portion of the study was acquired in the craniocaudal direction encompassing vertex to midthigh with the patient supine, with a slice thickness of 5 mm, an increment of 1.5 mm, 140 keV, 220 mAs, and 0.6 pitch. PET acquisition was subsequently acquired in the craniocaudal direction to minimize misregistration in the neck and chest as the primary regions of interest. Three-dimensional acquisition was performed with emission data corrected for random, scatter, and decay. Reconstruction was conducted with an ordered subset expectation maximization algorithm with two iterations/eight subsets. Gaussian filtering with 7 mm at full-width at half-maximum kernel was applied to mitigate image noise in delayed acquisitions.
Two time point pretreatment 124I PET/CT images were used to predict radiation dosimetry of subsequent 131I therapy by providing a measure of regional pharmacokinetics. By modeling the uptake and clearance time of 124I, an estimate of regional decays per GBq injected (rad per mCi) was calculated considering different physical half-life of 131I. Disintegrations were converted into an estimate of radiation-absorbed dose based on the OLINDA (v1.1) sphere model dose factors (25). To achieve a dependable estimate of pharmacokinetics, the first 124I images were captured at ∼24–48 hours and the second time point was delayed to 72–96 hours. Local tracer uptake in the tumor and bone marrow was calculated. To account for partial volume effect in case of small tumor size, an expanded contour, which captured all of the local activity as well as a true physical contour based on the CT margins (where visible), was utilized to reconcentrate the activity to an accurate tumor volume.
F-18-labeled fluoro-2-deoxyglucose imaging protocol
F-18-labeled fluoro-2-deoxyglucose (FDG) PET/CT scans were performed at baseline, before the commencement of MAPK inhibitor treatment and at approximately three to four weeks following MAPK inhibitor, just before 124I injection. FDG PET/CT was used to assess metabolic activity at the metastatic sites and monitor response to treatment.
Baseline and post-MAPK inhibitor treatment FDG PET/CT scans were performed on the abovementioned scanners. Patients fasted for at least six hours, had blood glucose measurements before administration of 3–4 MBq/kg of FDG, and acquisition of PET images was commenced approximately one hour later.
RAI treatment and follow-up
Restoration of RAI concentration following MAPK inhibitor was defined visually by new RAI avidity at metastatic sites. With increasing experience, an estimated radiation-absorbed dose derived from 124I two time point imagings was incorporated in the decision-making of suitability for RAI treatment. 124I-based dosimetry estimates were regarded as a proof-of-concept approach and the information was used as a general rather than strict guide for choosing the administered activity in conjunction with other aspects of the disease, including organs involved and the volume of metastases. All patients underwent a post-treatment whole-body planar and SPECT/CT of the metastatic region at approximately seven days after administration of RAI therapy.
The patients had follow-up at three months to assess imaging and biochemical response to treatment. Imaging response was assessed based on response evaluation criteria in solid tumors version 1.1 (RECIST v1.1) (26). Biochemical response was assessed by measuring thyroglobulin levels. Ongoing follow-up (median 16 months, range 5–40) until the date of article submission was recorded.
Results
From 2015 to 2017, six patients (age range 45–70, four females) underwent this redifferentiation protocol. Patient 1 was initially RAI avid at all metastatic sites but gradually lost RAI avidity after multiple RAI treatments. The other five patients were either minimally RAI avid or RAI negative in at least some metastatic sites at the time of diagnosis. Patients 1 and 2 had FTC with components of poorly differentiated on histopathology and a confirmed NRAS mutation. The BRAFV600E mutation was seen only in PTC. Table 1 shows the patient characteristics.
Patient Characteristics
CLND, cervical lymph node dissection; F, female; FTC, follicular thyroid carcinoma; M, male; MEK/PI3b-i, MEK/PI3b-inhibitor; PDTC, poorly differentiated thyroid carcinoma; Pt, patient; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; Rx, treatment; TNM, tumor, node, metastasis American Joint Commission on Cancer (AJCC) staging system; TT, total thyroidectomy.
Three patients (patients 1, 2, and 5) underwent RAI therapy within 12 months before redifferentiation therapy. Patients 1 and 2 demonstrated radiological and biochemical progression within 12 months of RAI therapy. Patient 5 proceeded to redifferentiation protocol following the absence of any uptake in lung metastases on the first post-RAI therapy scan, and progression could not be ascertained. All patients except patient 6 had already undergone at least one RAI treatment. The pretreatment 124I PET/CT of patient 6 showed only a small focus in the neck with no RAI avidity within known pulmonary metastases. Given the poor prognostic factors at baseline, including high FDG avidity of the tumor, and to maximize the clinical benefit from RAI therapy, the patient was considered for the redifferentiation protocol.
All patients with NRAS mutations received trametinib. One patient with a tumor harboring a BRAFV600E mutant received dabrafenib and trametinib and the other two were treated with vemurafenib and cobimetinib. All except one patient (who had underlying medical comorbidities) underwent THW for four weeks. One patient did not reach the predefined threshold of TSH stimulation (TSH only 25.9 mU/L) despite four weeks of THW. This was assumed to be related to the redifferentiation of the functional thyroid cancer cells following MAPK pathway inhibition. Therefore, two doses of rhTSH were administered and TSH increased to 149.9 mU/L. Table 2 details the redifferentiation protocol, and Table 3 summarizes the 124I dosimetry results and temporal changes in FDG uptake.
Summary of Redifferentiation Protocol and Patient Outcomes
Imaging response based on RECIST v 1.1 (response evaluation in solid tumors version 1.1).
rhTSH required as stimulated TSH following THW was 25.9mU/L. This increased to 149.9mU/L following rhTSH administration.
Due to raised thyroid antibodies.
AE, adverse event; BRAF-i, BRAF-inhibitor; CTCAE, Common Terminology Criteria for Adverse Events version 4; MAPK, mitogen-activated protein kinase; MAPK-i, MAPK-inhibitor; MEK-i, MEK-inhibitor; mTKI, multitargeted tyrosine kinase inhibitors; NA, not available; PR, partial response; rhTSH, recombinant human TSH; SD, stable disease; Tg, suppressed thyroglobulin; THW, thyroid hormone withdrawal; TSH, thyrotropin; UA, unassessable.
Summary of 124I and F-18-Labeled Fluoro-2-Deoxyglucose Positron Emission Tomography/Computed Tomography Parameters and Temporal Changes Following Four-Week Mitogen-Activated Protein Kinase Pathway Blockade
↑, increase; ↓, decrease; 18F-FDG, 18F-labeled fluoro-2-deoxyglucose; SUVmax, maximum standardized uptake value.
Overall, four patients achieved restoration of the iodine avidity and underwent RAI therapy. These patients demonstrated satisfactory RAI retention on post-treatment scans (range 1.2–5.3%). The median follow-up of these patients was 16.6 months (range 13.5–42.3 months) from the commencement of the protocol. Of these patients, three achieved a partial imaging response and one patient had stable disease according to RECIST v1.1 with no further treatment required until the last follow-up. Figure 2 depicts the RECIST v1.1 response assessment during follow-up, and Supplementary Table S1 provides the temporal changes in the measurements of the target lesions. Figures 3 and 4 depict patients (patients 1, 4, 5, and 6) with successful restoration of RAI avidity and satisfactory retention of RAI on post-treatment scans. Two patients (patients 2 and 3) who did not achieve of RAI avidity (Fig. 5) were treated with lenvatinib. Both patients remained responsive to lenvatinib at 17 months and 43 months of follow-up.

Response assessment by RECIST1.1 demonstrates the percentage change in the SOT following redifferentiation protocol. SOT, sum of target lesions. Color images are available online.

Pt 1 and 4, baseline iodine scans demonstrate inadequate iodine uptake at metastatic sites. Following four weeks of treatment with MAPK pathway inhibition (Pt 1, trametinib; Pt 4, trametinib and dabrafenib), 124I PET MIP images show restoration of iodine avidity at the metastatic sites (brackets). 131I post-treatment images show satisfactory retention of RAI in metastatic sites. High liver uptake on delayed 131I post-treatment scan for Pt 1 (arrow) is suggestive of significant hepatic metabolism of radioactive thyroid hormone, which may imply redifferentiation of thyroid cancer tissue. 124I PET images have uniform SUV threshold of 20. MAPK, mitogen-activated protein kinase; MIP, maximum intensity projection; Pt, patient; RAI, radioactive iodine; SUV, standardized uptake value. Color images are available online.

Pt 5 and 6, baseline 124I PET MIP images show low iodine uptake at metastatic sites in the thorax. Following four weeks of treatment with MAPK pathway inhibition (vemurafenib and cobimetinib), 124I PET MIP images demonstrate restoration of iodine avidity at the metastatic sites (brackets) and enhancement of uptake in the neck (arrows). 131I post-treatment images show satisfactory retention of RAI in metastatic sites (brackets) and neck (arrows). 124I PET images have uniform SUV threshold of 20. Color images are available online.
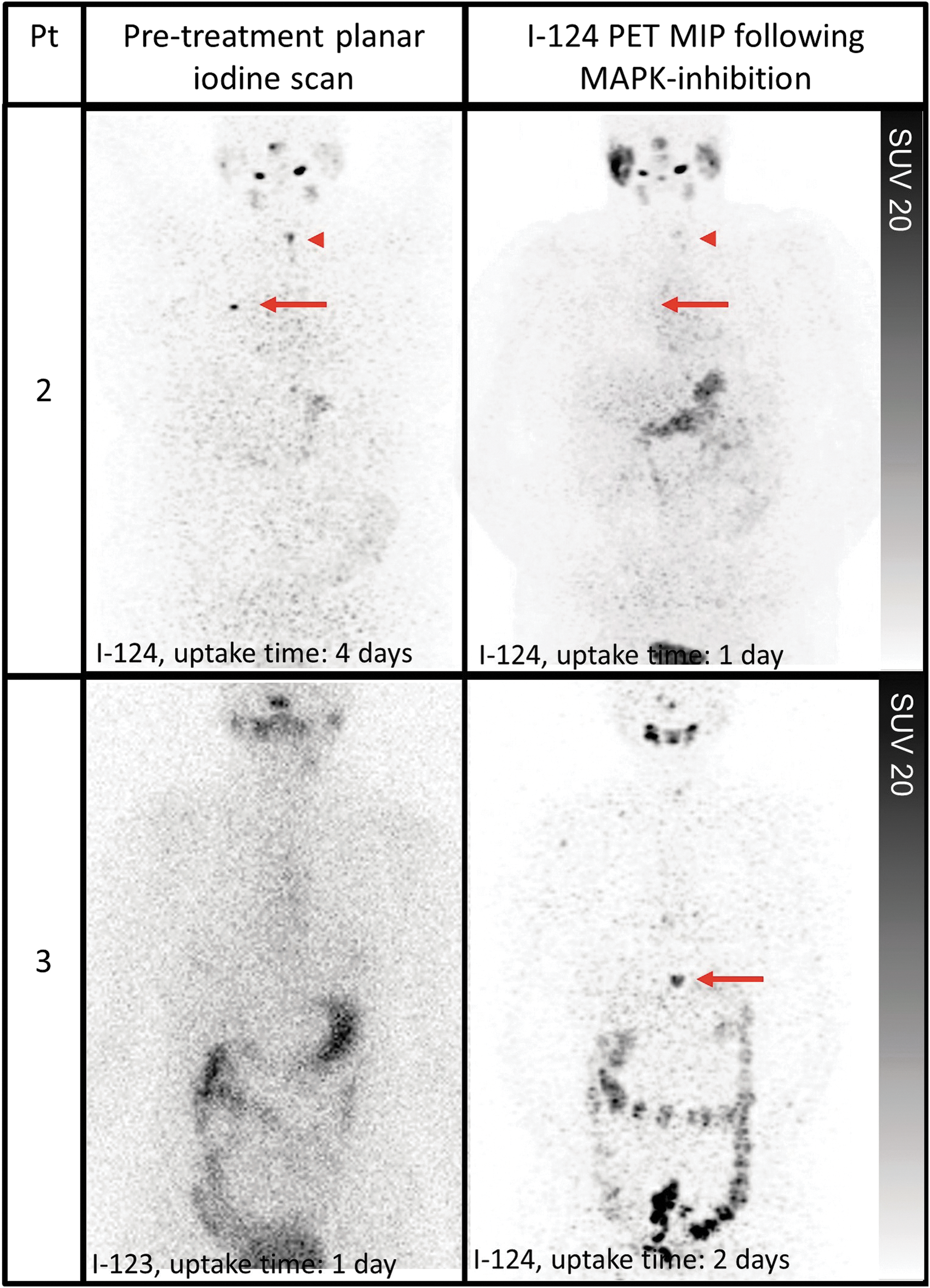
Pt 2 baseline iodine scan demonstrates low iodine uptake at metastatic sites in the chest (arrow) and neck (arrowhead). Following four weeks of treatment with MAPK pathway inhibition (trametinib), 124I PET MIP image demonstrates no significant enhancement of iodine avidity (arrow and arrowhead). Pt 3 baseline iodine scan shows no significant iodine avidity and following treatment with trametinib, suboptimal restoration of iodine avidity is noted (arrow). 124I PET images have uniform SUV threshold of 20. Color images are available online.
Discussion
Optimizing MAPK pathway inhibition
The MAPK signaling cascade is a critical pathway for human cancer cell survival, differentiation, dissemination, and resistance to drug therapy (27). The MAPK pathway is activated by upstream genomic events and/or activation of multiple signaling events where information converges at this nodal pathway point. This pathway is highly regulated in normal cells by phosphatases and bidirectional communication with other pathways, such as the AKT/mTOR pathway, which promotes anabolism (27). In cancer cells, this pathway is dysregulated, and its impact predominantly depends on the intensity of the signal and the context or tissue in which the signal is aberrantly activated (28). Understanding the differential nature of activation of the MAPK pathway in each tumor type is critical in developing single and combination regimens, as different tumors have unique mechanisms of primary and secondary signaling and subsequent sensitivity to drugs (28).
Phase I and II studies using different BRAF inhibitors (including dabrafenib and vemurafenib) have shown antitumor activity in patients with progressive BRAFV600E mutant PTC refractory to RAI therapy (29,30). In patients with BRAFV600E-mutated metastatic melanoma, combination therapy with a BRAF inhibitor and an MEK inhibitor significantly improved median OS and PFS compared with a BRAF inhibitor alone (31). A randomized phase II study comparing the BRAF inhibitor dabrafenib with and without the MEK inhibitor trametinib demonstrated similar responses but longer PFS with the combination (
Although clinical trials of MEK inhibitor monotherapy using selumetinib in NRAS mutant patients have not yet demonstrated robust response rates (32,33), highly favorable results have been reported in a redifferentiation protocol (17). In the study by Ho et al., all five patients with an NRAS mutation treated with selumetinib had successful redifferentiation and underwent RAI therapy, while only one of nine patients with a BRAFV600E mutation reaching the predefined threshold of iodine uptake restoration to undergo RAI therapy (17). Different levels of MEK inhibitor sensitivity were observed in tumor cell lines with BRAF or RAS mutations (34). Furthermore, in preclinical models, differences in the potency of MEK inhibitors have been observed. For instance, in ovarian and lung cancer cell line models, trametinib has shown more effective inhibition of cellular proliferation than other MEK inhibitors, including selumetinib (34,35). Given a potentially higher potency of trametinib and a lack of access to selumetinib in Australia, we elected to use trametinib in RAS mutant patients. Only one of three NRAS mutant patients achieved sufficient iodine avidity following single-agent MEK inhibitor therapy and was treated with RAI with satisfactory iodine retention. This patient maintained a durable response up to 30 months after therapy with the redifferentiation protocol (Fig. 2) despite previously progressing disease. The optimal single or combination small-molecule inhibitors of the MAPK pathway remain unknown and require further study. Table 4 summarizes the key features of the studies by Ho et al. (17) and Rothenberg et al. (18) compared with the current cohort.
Comparison of the Current Study Protocol and Patient Outcome to Previous Literature
Although in prior studies and in our cohort, at least four weeks of MAPK inhibitor therapy has been administered, the duration of redifferentiation therapies remains unclear. In thyroid cancer cell line models, withdrawal of BRAF oncogenic induction has resulted in an increase in apoptosis within 72 hours, which was no longer detectable by two weeks (16). It was also noted that apoptosis was restricted within two weeks due to the restoration of the follicular structure, thyroid-specific gene expression, and thyroid function. Although therapy with the small-molecule MAPK inhibitor used in the study showed a more attenuated recovery of expression of thyroid-specific genes compared with the withdrawal of oncogenic induction, it is conceivable that even a shorter duration treatment would potentially achieve optimal redifferentiation with optimal blockade of this pathway. Shorter duration of treatment with MAPK inhibitors may also minimize the toxicity associated with these medications, while maximizing the long-term therapeutic effect of RAI therapy.
Appropriate clinical setting and patient selection
Since 2014, two novel systemic treatments have attracted attention and gained regulatory approval in the treatment RAIR DTC, sorafenib and lenvatinib. These two mTKI were approved for use in the United States and the European Union for patients with metastatic RAIR DTC based on phase III randomized placebo-controlled clinical trials, demonstrating improvement in PFS (4,5). Despite promising results from these trials, the OS advantage remains to be determined without evidence of improvement in QOL. In fact, these agents are associated with numerous adverse events likely to negatively impact QOL, necessitating dosage reductions in nearly two-thirds of patients, treatment discontinuation in up to 20% of patients, and therapy-related death in 1.5–2% (4,5,36). Although the crossover trial designs effectively contaminated OS data, the absence of a proven effect of mTKI on OS in these trials may indicate that a delay in initiation of these treatments until observation of RECIST progression among initially placebo-treated patients did not adversely affect OS.
In the absence of definitive data on OS and QOL, an evidence-based recommendation with expert consensus suggests considerable restraint in the use of mTKI. Based on general expert consensus guidelines, consideration of treatment with mTKI should be reserved for structurally progressive, symptomatic, and/or imminently threatening DTC (in which disease progression is expected to require intervention and/or to produce morbidity or mortality in less than six months), that is, RAIR, and not amenable to satisfactory control using directed approaches such as surgery or radiotherapy (37,38).
Therefore, it is important to optimally apply all approaches to therapeutic RAI before embarking on these treatments. Patients with specific therapeutically targetable tumor alterations, such as BRAF or RAS mutations in the MAPK pathway, can also be considered for short-term therapies specifically targeting these alterations to restore iodine avidity. However, given the indolent nature of the metastatic disease in most patients, therapeutic interventions should not be considered for patients with stable, asymptomatic metastatic disease unless agents with a significant likelihood of leading to complete remission, prolongation of survival, or biologic impact such as redifferentiation are available. Compared with conventional chemotherapy or novel agents, the ability to induce iodine uptake in RAIR metastatic DTC has the potential advantage of requiring only a short course of targeted therapy to maximize the potential long-term therapeutic effect from RAI therapy.
In this cohort, we recruited patients with progressive metastatic disease despite treatment with RAI within the previous 12 months. We also treated patients with de novo non-RAI avid metastatic disease to modify the biology of the tumors and render them susceptible to RAI therapy. One patient (patient 6) had never been treated with RAI but had iodine avid residual disease in the neck and iodine-negative distant metastatic disease. While utilization of the redifferentiation protocol maintained the treatment efficacy in the neck, it also restored iodine avidity in the distant metastatic disease enabling all sites of disease to be effectively targeted by RAI therapy. Future trials, however, are needed to clarify the long-term efficacy of this treatment strategy.
Role of dosimetry
The dosimetry approach is not currently used in many institutions, although most available guidelines do mention its feasibility (39,40). The American Thyroid Association (ATA) guidelines classify dosimetry-guided RAI-administered activity to lung and bone metastases as a weak recommendation with low-quality evidence (38). The purpose of dosimetry in these contexts is to limit the whole-body retention to 2.1 GBq (80 mCi) at 48 hours and 2 Gy to the bone marrow. The usefulness of dosimetry should not be assessed only according to patient survival or therapeutic efficacy; the possible avoidance of futile RAI treatments and better characterization of RAIR disease should also be considered. This is especially of critical importance when the degree of restoration of iodine avidity is assessed following redifferentiation therapy with MAPK inhibition.
Ho et al. used 124I PET/CT lesional dosimetry to predict which patients were most likely to respond to RAI therapy (17). Based on 124I PET/CT dosimetry following redifferentiation therapy, if one or more lesions could be treated with a dose of 20 Gy or more with an 131I-administered activity of 8.1 GBq (300 mCi), the patient was eligible for RAI therapy. The eligible patients underwent a whole-body and blood standard 131I dosimetry protocol to determine maximum tolerable activity. Following redifferentiation therapy with selumetinib, 12 of 20 patients had increased iodine uptake, but only 8 patients reached the predefined threshold for treatment. Of those eight patients, six achieved imaging partial response. Rothenberg et al. used 131I for assessment of restoration of iodine avidity, and any new or increased uptake at the sites of disease were considered suitable for RAI therapy (18). In this study, 6 of 10 patients were treated with RAI with two patients achieving a partial response.
124I PET dosimetry is a promising technique for more precise quantitation of RAI uptake (41). The potential advantages of the 124I PET/CT over 131I whole-body scanning include inherent quantitation of PET imaging, greater sensitivity for the detection of small lesions even at several days postadministration, and the ability to predict radiation dosimetry. In this small sample size, we have described a dosimetry approach based on two time point 124I PET/CT, which may obviate the need for further pretreatment 131I dosimetry, hence simplifying this protocol. The question for the future is how to include dosimetry into the patient management framework. A larger sample size using prospective dosimetry is needed to validate this 124I dosimetry approach in metastatic DTC.
THW versus rhTSH
No randomized trial comparing THW- to rhTSH-mediated therapy for the treatment of distant metastatic disease has been reported. Importantly, however, rhTSH has not been approved for use in patients with metastatic disease and there is increasing evidence indicating an improvement of the therapeutic index of RAI therapy by THW. Studies have shown that 124I PET using rhTSH stimulation does not predict the uptake on 131I post-therapy scans at sites of metastatic disease following THW (20), but is highly accurate when THW is used for both scans (21). A small intrapatient 124I dosimetry comparison also demonstrated higher tumor-to-dose-limiting-organ (bone marrow)-absorbed dose ratio using THW than rhTSH-stimulated administrations (22). One small comparative study showed the median half-life and cumulative activity in tumor tissue was higher in THW than rhTSH-mediated RAI treatment (42).
In contrast to both prior studies using redifferentiation therapy in which rhTSH-mediated RAI therapy was used (17,18), our protocol mandated THW unless it was contraindicated due to medical comorbidities. To the best of our knowledge, this is the first study demonstrating the feasibility of THW in this treatment strategy. THW also pragmatically avoids the expense and logistical challenge of rhTSH stimulation necessary for both 124I PET dosimetry and subsequent 131I therapy.
Predictive markers of response beyond genotype
Baseline metabolic activity and metabolic response to treatment measured by FDG PET have prognostic implication in many cancers, including DTC (43,44). Consequently, the prognostic value of FDG PET as a real-time imaging biomarker in a patient-based rather than lesion-based scale should be used at diagnosis of metastatic DTC and may guide the intensity of therapy aggressiveness.
In BRAF mutant melanoma, metabolic changes early after BRAF and MEK inhibition can be a useful prognostic indicator of response to treatment (45) but are not necessarily predictive of structural imaging response (46).
In our small cohort of three patients with a BRAFV600E mutation, we have observed a significant metabolic response following four weeks of combination BRAF and MEK inhibition (Fig. 2 and Supplementary Fig. S1). This also translated into the successful restoration of iodine uptake in all three patients, which rendered them suitable to RAI therapy. Surprisingly, two patients with RAS mutations had an increase in metabolic activity following MEK inhibition (Table 4 and Supplementary Fig. S2). This occurred despite a structural response in one of these patients. We hypothesize this may relate to bidirectional communication and deviation from the MAPK pathway to the AKT/mTOR pathway with a resultant increased glycolytic metabolic activity. THW with increased TSH stimulation may also contribute to this phenomenon. However, our preliminary data indicate that future trials may need to incorporate FDG PET in the selection and response assessment of the patients undergoing a redifferentiation protocol.
Limitations
It should be noted that the overall small sample size, retrospective nature of the study, and the short follow-up in some patients preclude further statistical analysis and recommendations regarding the optimal redifferentiation protocol. The aim of this study, however, was to demonstrate the feasibility of utilizing different genotype-selected regimens of MAPK inhibitors, including combination therapy utilizing THW stimulation, and to provide further evidence of potential efficacy in selected patients. Importantly, given concerns regarding the use of rhTSH in metastatic disease, this is the first published series of thyroid redifferentiation therapy using THW TSH stimulation. There is variability in the protocol used among the patients. This is a novel and complex treatment strategy with several uncertainties in terms of optimal protocol. Our protocol did evolve over time with variable access to combination BRAF/MEK inhibitor therapies and increasing experience in treating these patients. We have also demonstrated the feasibility of incorporating 124I dosimetry in this protocol. Nonetheless, prospective multicenter trials are needed to further assess the efficacy and safety of this treatment strategy in a larger cohort of patients.
Conclusion
MAPK pathway inhibition, with an MEK inhibitor alone or in combination with a BRAF-inhibitor, is a feasible and promising strategy to redifferentiate RAI refractory DTC associated with RAS or BRAFV600E driver mutations, rendering them suitable for RAI therapy. Our series demonstrates a practical protocol using THW TSH stimulation with tolerable side effects, given the concerns using rhTSH in the setting of metastatic disease and satisfactory RAI retention following treatment. Future trials are required to optimize MAPK pathway inhibition, minimize toxicity, and determine the duration and timing of the treatment schedule in appropriately selected patients; due to the rarity of advanced thyroid cancer this will likely require multicenter recruitment.
Footnotes
Acknowledgments
We acknowledge the effort of our nuclear medicine technologists, particularly Mark Scalzo, the chief nuclear medicine technologist, who coordinated the complex preparation and imaging schedule of these patients.
Author Disclosure Statement
Prof. Rodney J. Hicks is supported by an Australian National Health and Medical Research Council Practitioner Fellowship. Other authors express no competing financial interests.
Funding Information
No external funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1