
Abstract
Background:
Routine preoperative vocal cord (VC) assessment with laryngoscopy in patients undergoing thyroidectomy allows clear documentation of baseline VC function, aids in surgical planning in patients with palsies, and facilitates interpretation of intraoperative neuromonitoring (IONM) findings. We aimed to determine the incidence of preoperative vocal cord palsy (VCP); to evaluate the associated risk factors for preoperative VCP; and to calculate the cost-savings potential of implementing a selective approach.
Methods:
Patients with a pre-thyroidectomy VC assessment by fiberoptic laryngoscopy were retrospectively recruited from the Monash University Endocrine Surgery Unit database from 2000 to 2018. Cases with preoperative VCP were reviewed for potential contributing factors and compared with a non-palsy cohort.
Results:
Of the 5987 patients who had preoperative laryngoscopy, VCP was documented in 41 (0.68%) patients. Four clinical parameters were found to be potential indicators of VCP, including: age (p < 0.001), nodule ≥3.5 cm recorded on ultrasound imaging (p = 0.01), presence of voice symptoms (p < 0.001), and previous neck surgery (p < 0.001). Malignant cytology (p = 0.5) and exposure to head and neck irradiation were not different between the groups. Utilizing these risk factors, 2354 (39%) patients had at least one feature that may raise suspicion for preoperative VCP. By performing preoperative laryngoscopy only on this subset of patients, the potential cost savings exceeds 400 Australian Dollars per patient.
Conclusions:
Using this large dataset, we have established that a VCP is rare in the absence of a large nodule, hoarseness, or previous neck surgery. Therefore, in the era of IONM, we support a selective approach to preoperative laryngoscopy by using the aforementioned criteria.
Introduction
When performed by experienced, high-volume surgeons, thyroidectomy is a safe and predictable procedure with a low risk of major complications (1). One of the most well-known complications of the operation is injury to the recurrent laryngeal nerve (RLN), resulting in a vocal cord palsy (VCP) (2,3). Although spontaneous recovery is expected in the majority of cases, this complication can be a source of distress or malpractice litigation. While much attention has been directed to postoperative voice changes due to VCP secondary to RLN injury, existing preoperative palsies have received less attention. The incidence of VCP in the preoperative thyroid patient has been reported to be between 1% and 6% (4). In this patient group, commonly cited palsy causes include malignancy with local invasion, previous neck surgery, and cases of idiopathic origin (5).
Routine preoperative vocal cord (VC) assessment with laryngoscopy in patients undergoing thyroid surgery allows clear documentation of baseline VC function, aids in surgical planning in patients with preoperative palsy, and facilitates the interpretation of intraoperative neuromonitoring (IONM) findings (4,6,7). This has been the practice at our institution: Before thyroid surgery, every patient undergoes laryngoscopy assessment at our pre-admission clinic, which typically occurs two weeks before surgery.
Despite its long-standing practice, international guidelines are not in agreement on the validity and necessity of routine preoperative laryngoscopy for thyroid surgery. The International Neural Monitoring Study and the 2013 American Academy of Otolaryngology—Head and Neck Surgery Guidelines highlight the importance of preoperative VC evaluation, and recommend routine assessment (6,8). Other guidelines endorse a more selective approach. The widely referenced 2015 American Thyroid Association Guidelines recommend preoperative VC assessment be undertaken only for patients with voice abnormalities, history of chest or cervical surgery, or known thyroid cancer with posterior extension or extensive central nodal metastases (9). This dichotomy is also echoed in recent U.S. data which suggest routine preoperative VC assessment is undertaken in 6.1% to 72% of cases of various institutions (10,11).
With the objective of assessing the feasibility of transitioning to a selective approach of pre-thyroidectomy VC assessment without compromising patient care, this study aimed to determine the rate of preoperative VCP at our institution; to determine the clinical indicators of preoperative VCP; and to calculate the potential cost savings of implementing a selective approach.
Materials and Methods
Patient eligibility
This retrospective case-control study recruited patients from the Monash University Endocrine Surgery Unit (MUESU) database during a 19-year period between January 2000 and August 2018. Patients who had a VC assessment by fiberoptic laryngoscopy before undergoing thyroid surgery were eligible. The “Office of Ethics and Research Governance” at Alfred Health granted approval for the use and storage of patient information in the MUESU database, as well as subsequent analysis of the data.
Case file review
The MUESU database was used to identify patients with a preoperative VCP. Medical records and the MUESU database were reviewed for a number of potential indicators for VCP including: patient demographics, preoperative cytology results, hoarseness and other voice symptoms, previous neck surgery, largest nodule dimension, and history of head and neck irradiation.
In this study, malignancy was considered a potential preoperative VCP risk factor only if it was confirmed on preoperative cytology. Cases with “suspicious for malignancy” cytology or incidental malignant diagnosis on histology of the operative specimen were not considered when identifying VCP indicators. In addition to the fiberoptic laryngoscopy assessment, patients are screened for subjective changes in voice quality, including hoarseness, altered pitch, vocal tremor, weakness, breathiness, or strained voice quality. Previous neck surgery included patients who had undergone previous thyroid, parathyroid, cervical spine, or esophageal (such as pharyngeal pouch) surgery. Largest nodule dimension was defined by the maximal dimension of nodules measured on preoperative ultrasonography. History of head and neck irradiation included patients who had external beam radiotherapy for benign or malignant conditions, childhood exposure to high levels of environmental radiation, and radioactive iodine ablation.
Statistical analysis
The incidence of potential VCP indicators was summarized by using frequency tables, which were used to identify the most common indicators. The VCP group was compared to patients without preoperative VCP using Stata SE v14, with a p-value of <0.05 set as significant. Continuous variables are reported as mean ± standard deviation, and categorical variables are reported as number and percentage.
Cost analysis
Cost-savings calculations were determined based on an estimated direct cost of 400 Australian Dollars (AUD) per laryngoscopy. This evaluation was based on the cost of a single-use laryngoscopy, and staff time involved in each procedure.
Results
Case identification
During the study period, all 5987 patients who underwent thyroidectomy were assessed with preoperative and postoperative laryngoscopy, and they were eligible for inclusion in analysis. Of these, 41 (0.68%) were found to have a VCP at the preoperative laryngoscopy. These 41 cases were labeled as the “VCP group,” and the remaining 5946 were called the “No palsy group” or “NP group.”
Baseline characteristics
The cohort had a female preponderance (80%), and ranged in age from 18 to 98 years, with a mean age of 54 ± 19 years. The mean size of thyroid nodules was 3.3 ± 2.0 cm (Table 1).
Baseline Characteristics of Thyroid Surgery Patients and Frequency of Potential Vocal Cord Palsy Risk Factors
Other category includes patients who underwent lymph node dissections, incisional biopsies, isthmusectomies, and nodulectomies.
NP, no palsy; SD, standard deviation; VCP, vocal cord palsy.
Surgery type
The majority of the cohort underwent total thyroidectomy (56%) or hemithyroidectomy (41%), while a minority of the cohort underwent a procedure categorized as “Other” (3%; Table 1). No statistical difference between the rates of total- or hemi-thyroidectomy in the VCP and NP groups was observed. Significantly more patients in the VCP group underwent an “Other” procedure (5/41 vs. 120/5946, p = 0.002; Table 1).
Clinical features
Four clinical parameters were found to be potential indicators of VCP as they were statistically different between the two groups. These include age, largest nodule dimension on ultrasound imaging, presence of voice symptoms, and previous neck surgery. On the other hand, rates of malignant cytology and exposure to head and neck irradiation were not different between the groups (Table 1).
Age
Patients in the VCP group were significantly older than patients in the NP group, ranging in age from 35 to 89 years, with a mean of 66 ± 15 years (p < 0.001; Table 1).
Voice changes
Subjective voice changes were reported by 5% of patients overall. Patients with VCP were more likely to complain of voice symptoms (17/41, 41%) compared to the NP group patients (290/5946, 5%; p < 0.001; Table 1). Conversely, 59% (24/41) of patients with VCP denied any voice changes.
Previous surgery
Significantly more patients in the VCP group had undergone previous neck surgery (32%, 12/41) compared with the NP group (10%, 585/5946; p < 0.001; Table 1). In each VCP case, the palsy identified on preoperative laryngoscopy corresponded to the side of previous neck surgery.
Malignancy
Preoperative diagnosis of malignancy by fine needle aspiration (FNA) cytology was made in 17% (7/41) of the VCP group. Of these 7, 3 patients (43%) also reported a subjective change in voice preoperatively. A similar proportion of patients (13%, 788/5946) in the NP group had a malignant cytology preoperatively (p = 0.5; Table 1).
Radiation exposure
No patient in the VCP group had a history of head and neck irradiation while 3% (196/5946) of the NP group did (Table 1).
Nodule size
In patients with a preoperative VCP, the largest nodule dimension ranged from 0.3 to 10.5 cm, with a mean of 4.4 ± 2.2 cm (Table 1). The largest nodule dimension of the NP group ranged from 0.3 to 12.0 cm, but the mean size was significantly smaller compared with the VCP group (mean 3.3 ± 2.0 cm; p = 0.01; Table 1).
From the analysis just cited, age, nodule size, voice change, and history of neck surgery were found to be significantly different between the VCP and NP groups. A total of 5102 (85%) patients did not have preoperative voice change or previous neck surgery. Their age ranged from 35 to 89, and the largest nodule dimension ranged from 3.5 to 10.0 cm. Therefore, to capture all patients with VCP preoperatively, a cut-off nodule size of ≥3.5 cm was used for the following analysis. Further, in the VCP group, 49% (20/41) of cases had a large nodule, defined as a nodule ≥3.5 cm. This was a significantly greater proportion compared with the NP group (N = 1607, 27%; p = 0.003).
Figure 1 visually depicts potential VCP indicators identified in the 41 palsy cases, including multiple indicators within the same patients. As demonstrated in Figure 1, patients with malignancy on cytology had a second risk factor of VCP identified preoperatively: nodule size ≥3.5 cm, hoarseness, or both. This suggests that malignant cytology is not an independent risk factor of VCP.

Venn diagram visually depicting potential VCP indicators and their case overlap. FNA, fine needle aspiration.
In summary, hoarseness, previous neck surgery, and nodule size ≥3.5 cm were found to be indicators of possible VCP (Fig. 1).
Selective laryngoscopy
The majority (N = 3633, 61%) of the 5987 patients who underwent preoperative laryngoscopy did not have any of the indicators for preoperative VCP cited earlier. None of these 3633 patients had a preoperative VCP (Table 2).
Frequency of One or More Vocal Cord Palsy Risk Factor
The remaining 2354 (39%) patients had one or more indicators of palsy. Hoarseness of the voice was reported by 307 (13%) patients, 598 (25%) patients had previous neck surgery, and 1627 (69%) patients had a nodule measuring ≥3.5 cm (Table 2; Fig. 2). In this group, 41 (1.7%) patients were diagnosed with VCP on preoperative laryngoscopy.
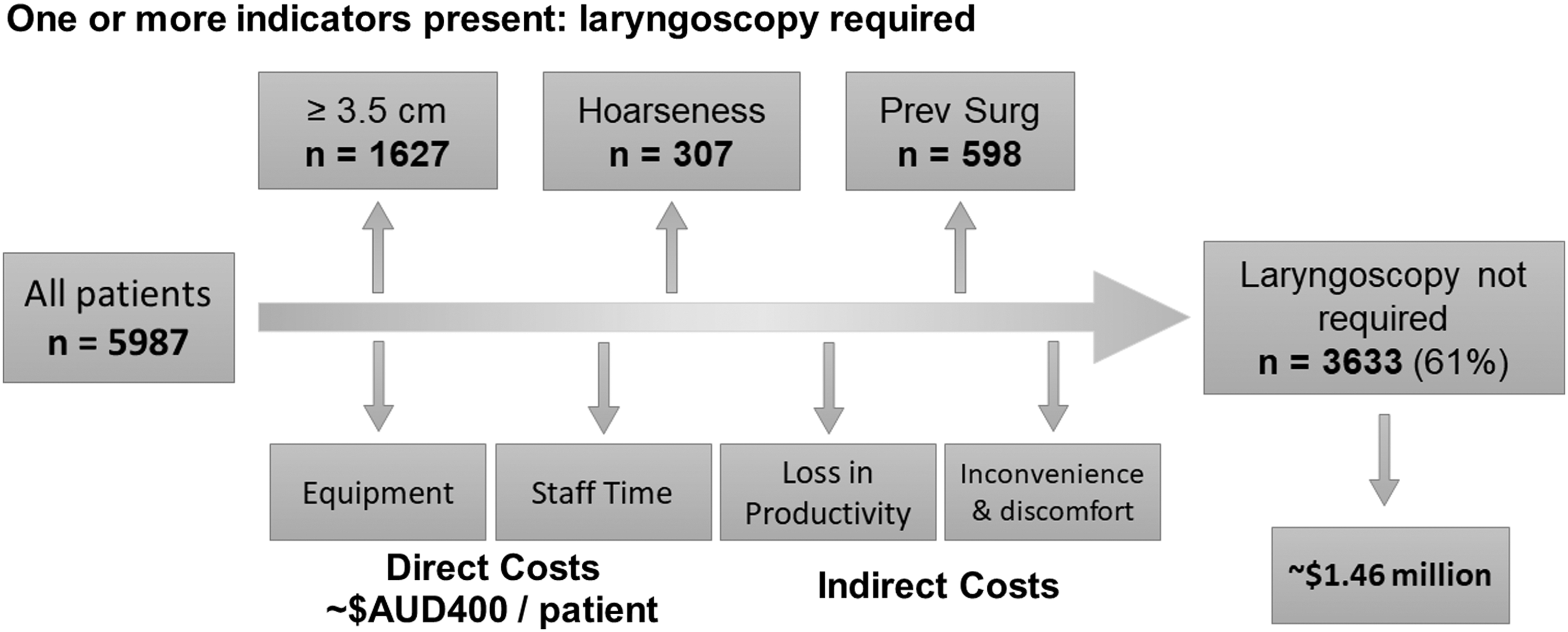
Proposed selective approach to pre-thyroidectomy laryngoscopy. This schematic diagram illustrates that, if selective pre-thyroidectomy laryngoscopy was performed only on the 1627 patients with large nodules, 307 patients with hoarseness, and 598 patients who had previous neck surgery, of the 5987 patients in our cohort, 3633 would not have required laryngoscopy without missing a preoperative vocal cord palsy. This could translate to more than a million dollars in cost savings. AUD, Australian Dollars.
Intraoperative neuromonitoring
Operative records of the palsy patients were analyzed. Of the 41 palsy patients with preoperative palsy, 39 (95%) had no vagal IONM signal on the ipsilateral side of their palsy. In the other two patients, the palsy side was not entered, and therefore no documentation of the IONM finding was available.
Cost savings
If a selective model of preoperative laryngoscopy was implemented, 3633 (61%) of this cohort would not have required preoperative laryngoscopy without missing a diagnosis of VCP. Using an estimated direct cost of 400 AUD per laryngoscopy, including equipment and staff expenses, more than 1.45 million AUD is the potential saving over the study period (Fig. 2).
Discussion
In this cohort of 5987 patients, preoperative VCP was identified in <1% of cases (N = 41, 0.68%). This study identified three independent indicators of preoperative VCP: subjective voice symptoms, previous neck surgery, and a large nodule (≥3.5 cm). These risk factors may be used to justify a selective approach to preoperative laryngoscopy without compromising patient care.
The prevalence of VCP in patients who underwent routine laryngoscopy before thyroidectomy has been reported in several retrospective case series (2,12,13). Both an Australian study (N = 160) (2) and, more recently a German study (N = 1333) (12) reported a preoperative VCP prevalence of 0.6%. A similar rate (0.68%) was found in this study with a larger cohort (N = 5987). Other studies suggest that preoperative palsy is more common, with one U.S. study suggesting that the preoperative palsy rate may be as high as 6.5% (N = 340) (13). These differences may reflect the patients in each cohort, including patient age and the proportion of patients undergoing revision procedures or with previous neck surgery (4,11,14). There is a lack of consensus on the necessity and practicality of preoperative laryngoscopy for all thyroid surgery patients (13,15).
Published literature cites the three most common indicators of preoperative VCP as malignancy, hoarse voice, and previous neck surgery (2,4,16 –18). This study confirms that a change in the quality of voice and previous neck surgery are clinically useful indicators of potential VCP. However, the preoperative cytological diagnosis of malignancy was not an independent indicator in this study. In addition to these commonly cited causes, our study found that large nodule size may also be used as an indicator of possible VCP.
It is well known that VCP may occur without the patient experiencing or reporting voice symptoms (19 –21). Indeed, only 41% (17/41) of patients with palsy in this study reported change in voice quality. If this measure was used in isolation, 59% (24/41) of patients with preoperative palsy may have been missed. Instead, these patients were captured by one or both of the other indicators—previous neck surgery and nodules ≥3.5 cm. Ipso facto, the absence of voice symptoms should not negate VC assessment, if one of these other features are present.
The RLN is vulnerable to injury during neck surgery, including thyroid surgery, with permanent nerve injury documented in up to 5% of cases (22,23). In our study, 32% (13/41) of the VCP group patients had undergone previous neck surgery. This rate is consistent with other studies (15,18).
A novel finding of this study is the relationship between large benign nodules and preoperative VCP. To our knowledge, this has not been previously reported. Nodules in the palsy group were significantly larger on average, compared with the NP group, and a significantly greater proportion of the palsy group nodules were >3.5 cm. The American Cancer Society's “Thyroid Cancer Stages” utilizes a 4-cm cut-off to differentiate between T2 and T3 tumors (24). If this convenient size was used to select patients for laryngoscopic assessment, instead of 3.5 cm, only one patient would have their VCP missed preoperatively. and not be considered for preoperative laryngoscopy.
While malignancy is often cited as a cause of RLN palsy, those studies typically use postoperative histology for determination of malignancy (11,25). Up to 25% of FNA samples yield an indeterminate cytology (9). Thus, a malignant diagnosis is not always known preoperatively. Accordingly, only a minority of our VCP cases (N = 7, 17%) had a malignant cytology preoperatively. In each of these cases, either a nodule ≥3.5 cm or voice symptoms was present, and would have ensured that the patient was thoroughly assessed if a selective laryngoscopy model was in place. If patients with a preoperative malignant diagnosis were included in our selective laryngoscopy model, an additional 788 patients (13%) of our cohort would undergo preoperative VC assessment. All of these 788 patients did not have another identifiable risk factor, and they did not have a palsy identified.
Our study found that patients with VCP (66 ± 15) were considerably older compared with the non-palsy group (54 ± 19; p < 0.001). This finding is consistent with other publications (11,14). Despite the significant difference in mean age of the groups, overlap in the ranges renders it unhelpful as a selection criterion.
In our institution, thyroidectomy patients undergo pre- and postoperative VC assessment by laryngoscopy. The resultant large dataset enables us to develop a set of clinically useful criteria to accurately select patients for preoperative laryngoscopy, as we transition from routine to selective preoperative laryngoscopy. Effective selection would confer benefits such as cost savings, more streamlined preoperative process, and less patient discomfort, without compromising care. From the findings of this study, if a selective model was introduced, 61% of our patient cohort (N = 3633) would not require VC assessment (Fig. 2). Our data suggest that none of these patients would have a VCP that would be missed, and, consequently, patient care would be unlikely to be compromised.
Implementing a selective approach to preoperative laryngoscopy poses challenges. Voice symptoms are typically subjective and patient reported, and may not be noticed by the patient, especially in the setting of insidious onset. To overcome this challenge, clinicians should consider applying objective methods of voice quality to assess a patient's preoperative voice. This practice is supported by guidelines from the American Academy of Otolaryngology, Head and Neck Surgery Foundation (8). Furthermore, although our model suggests that no patient with VCP would be overlooked, the risk of an undiagnosed VCP will never equal zero if a selective preoperative laryngoscopy approach was adopted. A study by Schlosser et al. reported a similar finding: 420 patients presented without voice symptoms, previous neck surgery, or malignancy, and only one patient (0.23%) had a preoperative VCP (15). In addition, while laryngoscopy is considered the gold standard assessment of VC function, it is a subjective assessment and is therefore open to inaccuracies. There is a possibility of missing a subtle incomplete palsy, especially if not all appropriate maneuvers are performed during laryngoscopy. We feel that the risk of missing a palsy is somewhat mitigated by the routine use of IONM. If the vagal stimulation is normal at the start of surgery, the surgeon can be reassured of the integrity of the ipsilateral VC function, as high negative predictive values of 98.5–99.6% have been reported (26 –28). However, in case the patient has not had a preoperative laryngoscopy and has none of the 3 aforementioned risk factors, and the vagal stimulation is absent before the thyroid lobe is mobilized, the surgeon needs to carefully troubleshoot the IONM setup before considering altering surgical strategy. This may include checking the position of the endotracheal tube with direct laryngoscopy, checking for a signal in the contralateral vagus nerve, and stimulating the vagus more proximally to exclude a non-RLN (on the right side), among many other steps (6).
This study provides several opportunities to consolidate our proposed selective preoperative laryngoscopy approach. This includes collecting data on voice symptoms with more objective evaluations such as the Voice Handicap Index Questionnaire. Furthermore, data on previous thoracic surgery have not been captured in this retrospective study, as recommended by the 2013 American Academy of Otolaryngology—Head and Neck Surgery Guidelines (9).
There is no consensus on the need to assess VC before thyroid surgery. Using our large dataset, and with a review of 19 years of data, we have established the feasibility of adopting a selective approach to pre-thyroidectomy laryngoscopy without compromising patient care in the era of IONM. We propose that the main indicators in a selective model include voice symptoms, a history of previous neck surgery, and nodules ≥3.5 cm. While it is important for clinicians to exercise their clinical judgment, this model may provide significant cost savings for the health care system without compromising patient care or clinical standards.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank Mr. Chhavi Bhatt for his work populating and maintaining the Monash University Endocrine Surgery Database. They would also like to thank the Department of Otolaryngology, Head and Neck Surgery for their collaboration, and for pre- and postoperative voice assessments; and their colleague Dr. Meei Yeung for her clinical care of the patients.
Author Disclosure Statement
No competing financial interests exist. James Lee is the recipient of the Royal Australasian College of Surgeons Foundation for Surgery Senior Lecturer Fellowship (2017–2018).
Funding Information
No funding was received for this article.