
Abstract
Background:
Radioiodine (RAI) is a known risk factor for activation or de novo occurrence of Graves' orbitopathy (GO). Several studies demonstrated that GO can be prevented by glucocorticoids (GCs) in patients with pre-existing GO. We have previously shown that Graves' disease duration (GDd) <5 years is a risk factor for RAI-induced GO. We studied the effect of prophylaxis with either oral GCs (OGCs) or intravenous GCs (IVGCs) on GO activation in patients with GDd.
Methods:
In total, 99 hyperthyroid patients without GO or with pre-existing inactive GO with GDd <5 years were randomized to receive IVGCs (N = 49) or OGCs (N = 50) before RAI; 22 patients with GDd >5 did not receive steroids and were studied as controls. All patients underwent ophthalmological assessment before and 45, 90, 180 days and for a 5-year follow-up after RAI. Serum thyrotropin (TSH) receptor antibodies (TRAbs), thyroid hormones, and thyroid volume (TV) were also measured in response to RAI therapy and steroid prophylaxis.
Results:
No patient on prophylaxis developed GO after RAI. One woman of the control group, without steroid prophylaxis, and who had a marked elevation of her TSH, showed transient reactivation of GO, which spontaneously improved after restoring euthyroidism. On follow-up at 12 and 20 months after RAI, two patients developed overt optic neuropathy. A smaller TV was associated with a higher prevalence of RAI-induced hypothyroidism. Serum TRAbs increased significantly after RAI (p < 0.0001) but less in patients receiving steroids than in those without prophylaxis at 45 days (p < 0.01).
Conclusions:
The risk of RAI-induced GO can be prevented in all patients with GDd <5 years by steroids. Such treatment may not be necessary in patients with GDd >5 years. The blunting of TRAb elevation after RAI may be related to the prophylactic effect of steroids.
Introduction
Radioiodine (RAI) ablative treatment for Graves' hyperthyroidism (Graves' disease [GD]) has been associated with de novo occurrence or worsening of Graves' orbitopathy (GO) (1). The development or progression of GO after RAI is thought to be the consequence of radiation damage to the thyrocytes, resulting in release of thyroid antigens and activation of autoimmune reactions directed to the orbit (2). It is well accepted that patients with pre-existing GO who are active smokers, severely hyperthyroid before therapy, and with elevated serum levels of thyrotropin (TSH) receptor antibodies (TRAbs) are at increased risk for the progression of GO after RAI (3). In addition, GO may develop also if post-RAI hypothyroidism is not promptly corrected (4). In 1989, Bartalena et al. showed that systemic oral glucocorticoids (OGCs) prevent the exacerbation of GO that may occur after RAI in a proportion of patients with GD who have some degree of ocular involvement before treatment (5). Low-dose OGC prophylaxis has, therefore, been recommended in recent guidelines (EUGOGO; EUropean Group On Graves' Orbitopathy) for patients undergoing RAI who consider pre-existing GO among the risks of progression or de novo development of GO (6). A recent meta-analysis, which included 850 patients subjected to RAI, concluded that OGCs are very effective in preventing GO progression in patients with pre-existing GO, whereas randomized studies showing that steroid prophylaxis might be beneficial in patients without pre-existing signs of eye involvement are lacking (7).
Although the mechanism of RAI in triggering GO in patients without pre-existing disease is not clearly understood, de novo GO has been associated with cigarette smoking as a risk factor (1,8). As recently suggested (9), in patients without GO, the indication for steroid prophylaxis should be discussed with the patient before RAI treatment and based on specific risk factors. To date, there is unfortunately no consensus on either the criteria for selecting patients who may require steroid prophylaxis after RAI or the optimal steroid regimen, as reported in a survey among members of the European Thyroid Association (10). In 2009, a retrospective study on 113 patients subjected to RAI therapy assessed the prevalence of reactivation or de novo onset of GO, with or without steroid prophylaxis administered orally or intravenously (11). GO reactivated in 7.9% and newly occurred in 6.2% of patients, and was significantly more prevalent in patients with GD duration (GDd) <5 years. Moreover, intravenous glucocorticoids (IVGCs) were shown to be more effective than OGCs in preventing GO after RAI.
We have, therefore, designed the present prospective study in which patients with GDd of less than five years were randomized to receive either oral or intravenous steroid prophylaxis. As controls, we have studied patients with GDd of more than five years, who were not subjected to prophylaxis. The study objective was reactivation of GO or de novo occurrence of GO at six months after RAI. Patients were then observed for up to five years from RAI administration. In addition to GO activation, other study objectives were the outcomes of RAI therapy in controlling hyperthyroidism, the modifications of circulating TRAbs in response to steroid prophylaxis, and the impact of side effects, as recorded through a specific questionnaire administered to the patients during the course of steroid therapy.
Patients and Methods
Patients
One hundred twenty-one consecutive patients, 93 women and 28 men aged 23–70 years, mean age (±standard error [SE]) 47.1 ± 1.2 years, with GD and relapsing hyperthyroidism after standard treatment with antithyroid drugs, were seen between July 2009 and July 2012 and studied prospectively and observed until 2017. Ninety-nine patients with pre-existing inactive GO (clinical activity score [CAS] <4/10) and 22 with no evidence of GO were treated with RAI at the time when hyperthyroidism relapsed with elevated serum-free thyroid hormone concentrations not exceeding >50% of the normal range, to reduce the risk of post-RAI thyrotoxicosis (Table 1). Exclusion criteria were the presence of active moderate or severe GO (dysthyroid optic neuropathy, DON), contraindications to glucocorticoids administration, and pregnancy. Patients with GDd shorter than five years were randomized to receive prophylaxis with low-dose IVGCs (n = 50) (Group A) or OGCs (n = 49) (Group B). As controls, we studied 22 patients with GDd of more than 5 years treated with RAI without steroid prophylaxis (Group C; Table 1). All patients were studied prospectively at 45, 90, and 180 days after RAI treatment, by testing thyroid function and serum TRAb levels and by performing ophthalmological assessment, which included lid fissure and Hertel measurements, visual acuity, and eye motility determination. Soft tissue involvement was graded according to the Color Atlas (12). Activity of GO was classified by the CAS (13). Patients were subsequently observed in our clinic for up to five years after RAI administration. The study was registered (EUDRACT number 2009-010632-18) and approved by the ethics committee of our institution and informed consent was obtained from all the patients.
Clinical and Biochemical Characteristics of the Patients Undergoing Radioactive Iodine Therapy for Hyperthyroidism with Either Intravenous (A) or Oral (B) Steroid Prophylaxis and Disease Duration Less Than Five Years or Without Steroid Prophylaxis and Disease Duration More Than Five Years (C)
Risk factors for reactivation or de novo occurrence of GO after RAI according to the pre-existing presence of ocular involvement. All values are reported as mean ± SE.
A vs. C; B vs. C.
CAS, clinical activity score; GD, Graves' disease; GO, Graves' orbitopathy; RAI, radioiodine; SE, standard error; TRAbs, thyrotropin receptor antibodies.
RAI treatment and steroid prophylaxis
All patients underwent a 99Tc thyroid uptake 48 hours before administration of a therapeutic dose of RAI. 131I was administered at a fixed dose of 600 MBq, the maximum dose allowed for out-patients according to the national legislation. In all patients, thioamides were discontinued 5–10 days before RAI therapy.
Steroid prophylaxis was begun 48 hour after administering RAI. OGC prophylaxis consisted in the administration of a fixed starting dose of 35 mg/day of prednisone tapered off in 10 weeks with a cumulative dose of 1.540 g. IVGCs were administered with 2 doses of 500 mg/week for the first 2 weeks and 2 doses of 250 mg/week for the last 2 weeks, with a cumulative dose of 1.500 g of methylprednisolone. In all patients, a pump proton inhibitor was administered throughout the period of steroid prophylaxis to prevent gastric bleeding.
Biochemical analysis and clinical assessment
Serum-free thyroxine (fT4), free triiodothyronine (fT3), and TSH concentrations were measured using an electrochemiluminescent immunoassay (Roche Diagnostics) and reference ranges were 8–17 pg/mL, 2–5 pg/mL, and 0.26–5.2 mU/L, respectively. Hypothyroidism was defined as a TSH >3.5 mU/L. The value of 3.5 mU/L is the one we chose to begin levothyroxine (LT4) replacement after RAI, to prevent GO progression due to hypothyroidism. Serum TRAbs were measured as TSH binding inhibitory immunoglobulins, using a second generation TRAK human lumitest (Thermofisher, AG, Henningsdorf/Berlin, Germany) (reference value <1.5 U/L). In patients undergoing steroid prophylaxis, serum glucose, aminotransferases, and gamma-glutamyltransferase were measured before RAI and at the end of steroid administration and expressed as U/L. Serology for hepatitis B virus and hepatitis C virus was also tested at baseline. At baseline, all patients were investigated for smoking habits. Thyroid volume (TV) was measured in all patients by thyroid ultrasound at baseline and at 180 days after RAI by the same operator. All patients undergoing steroid prophylaxis were administered a questionnaire on the side effects of treatment, which recorded pain in the thyroid region of the neck, asthenia, insomnia, gastritis, hypertension, weight gain, and diffuse myalgias.
Study endpoints
The primary endpoint of the study was the reactivation or de novo occurrence of GO, assessed with a CAS ≥4/10, in patients with pre-existing or absent GO, respectively. The secondary endpoints were the outcome of hyperthyroidism after RAI and its relationship with steroid prophylaxis, the change in TV after RAI, and the relationship between the modality of steroid administration and eventual adverse effects. We also studied the changes of serum TRAbs after RAI and in relation to steroid prophylaxis.
Statistical analysis
All values are expressed as mean ± SE. Analysis by χ2 test or Mann–Whitney test was applied as appropriate and performed using SPSS 8.0 for Windows. Significance was defined as p < 0.05.
Results
Occurrence of GO after RAI
The clinical and immunological baseline characteristics of all patients are given in Table 1. There were no differences in age, prevalence of smokers, 99Tc uptake, and titers of serum TRAbs in the groups of patients of the study. Pre-existing inactive GO was present in 82 out of 99 (82.8%) patients undergoing steroid prophylaxis (Groups A–B) and 17 of 22 (77%) of those not receiving steroids (Group C; Table 1). The distribution of patients with or without pre-existing GO was not different in either group of steroid prophylaxis or the control group without prophylaxis (p = NS). Patients with pre-existing GO or without GO were not different in terms of the prevalence of smokers and the presence of serum TRAbs (Table 1). None of the patients receiving steroid prophylaxis had reactivation or a de novo occurrence of GO at six months after RAI administration (Table 3). In addition, the effect of oral or intravenous steroid administration was not different in preventing GO after RAI. One woman, not subjected to steroid prophylaxis (Group C), had transient GO reactivation 90 days after RAI, which occurred when the patient rapidly became markedly hypothyroid (TSH 70 mU/L). GO spontaneously improved after restoring euthyroidism.
Relationship Between Clinical Parameters and Radioiodine Outcome at Six Months
Values are reported as mean ± SD.
GDd, GD duration; SD, standard deviation; TV, thyroid volume.
During follow-up, two patients developed acute DON (Table 2). Both patients had pre-existing GO and received steroid prophylaxis (one OCGs and one IVGCs). DON developed at 12 months after RAI in a woman who remained hyperthyroid and eventually required a second cycle of RAI. The second patient developed DON at 20 months of follow-up in the contralateral eye to the one previously affected by GO. In both patients, there were subclinical signs of mild inflammation throughout the observation period (CAS 2–3), but not unequivocal evidence of optic nerve involvement.
Occurrence of Orbitopathy in Graves' Disease Patients With and Without Pre-Existing Graves' Orbitopathy Subjected to Radioiodine With and Without Steroid Prophylaxis at 6 and >12 Months of Follow-Up
A, intravenous; B, oral steroid prophylaxis; C, no steroid prophylaxis.
Analysis of parameters influencing the outcome of RAI in controlling hyperthyroidism
Only 14 patients had a slight elevation of serum fT3 concentrations (mean 5.8 ± 0.7 pg/mL). Overall, RAI was equally effective in inducing hypothyroidism whether the patients received steroid prophylaxis (81/99, 91%) or not (18/22, 81.8%; p = NS) (Table 3), and no difference was found in the time of occurrence of hypothyroidism (p = NS). LT4 therapy was promptly started when TSH was >3.5 mU/L. Ten patients had persistent hyperthyroidism 6 months after RAI, and among them, 8 required additional antithyroid treatment. GDd did not influence the occurrence of hypothyroidism after RAI in either group of patients (p = NS) or controls (p = NS). Mean basal TV was 18.9 ± 10.9 mL in cured patients compared with 32.7 ± 16.5 mL in subjects who were not cured (Table 3). A decreased TV was significantly associated with a higher prevalence of RAI-induced hypothyroidism in any group of patients (groups A and B, p = 0.0001, group C, p = 0.032), although the magnitude of TV reduction was not different among groups (p = NS).
Relationship between serum TRAb levels and RAI
As expected, higher basal serum TRAb levels were detected in patients with larger TV (p = 0.046; not shown), but they did not differ between patients receiving steroid prophylaxis or not, nor between cured and not cured patients (Table 3; p = NS). Moreover, basal serum TRAb levels in patients who became hypothyroid at 45 days did not differ from those of patients who remained hyperthyroid (not shown; p = NS).
The changes of serum TRAb levels after RAI were studied prospectively to seek a possible relationship with GO reactivation or with steroid prophylaxis. Basal serum TRAb levels were not different in the three groups of patients (Table 1; p = NS) and increased significantly after RAI administration (p < 0.0001; Fig. 1), as expected. The increase was observed in all groups of patients and was independent of the route of steroid administration. At 45 days after treatment, patients undergoing steroid prophylaxis had significantly lower serum TRAb levels (about 1/3) than those not receiving steroids (Fig. 1; p = 0.01), and a delayed TRAbs peak at 180 days.
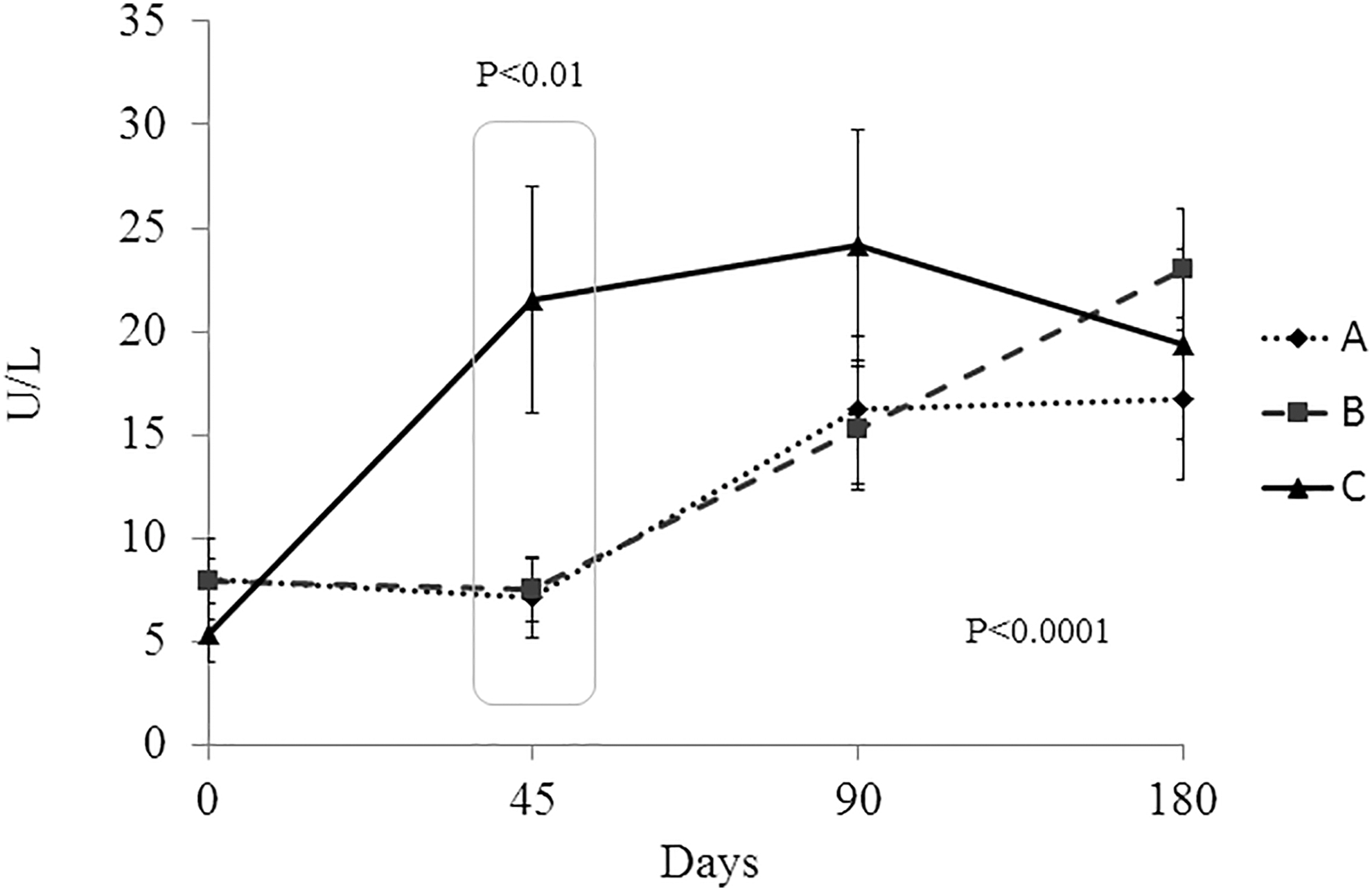
Changes of serum TRAb levels in response to RAI therapy in patients undergoing OGC prophylaxis (A), IVGCs (B), or no prophylaxis (C). A and B vs. C at 45 days p < 0.01 (ANOVA). ANOVA, analysis of variance; IVGCs, intravenous glucocorticoids; OGCs, oral glucocorticoids; RAI, radioiodine; TRAbs, thyrotropin receptor antibodies.
Side effects of RAI therapy
Sixty-one of 99 patients (61.6%) responded to a questionnaire on side effects of steroid prophylaxis. Twenty-four of 30 (80%) and 26 of 31 (84%) patients receiving OGCs and IVGCs, respectively, reported at least 1 symptom such as weight gain, mood disorders, and asthenia, with no differences between the route of steroid administration (p = NS). Interestingly, insomnia and gastric symptoms were more frequently reported by patients receiving OGCs than those receiving IVGCs (18 vs. 8, p = 0.035 and 14 vs. 3, p = 0.008, respectively).
Discussion
Systemic OGCs have been used to prevent the exacerbation of GO after RAI therapy for almost three decades (5), especially in patients with GD who have pre-existing GO. When planning for RAI ablation in patients with GD, the possibility of predicting which patients are at risk for the reactivation or de novo development of GO would limit the use of steroid prophylaxis to a specific set of patients. Until now, the choice has been to treat patients with pre-existing GO and with recognized risk factors for GO reactivation, such as smoking and elevated serum TRAbs before therapy (7,9). The question that remains unanswered is whether patients without GO undergoing RAI have such a negligible risk of developing GO to avoid prophylaxis or, alternatively, whether steroid prophylaxis should be cautiously undertaken in all patients (14). This approach could also be justified based on the data of Lai et al. who suggested that even very low doses of prednisone (0.1–0.2 mg/kg bw) tapered off in six weeks may be appropriate (15). This study was designed to confirm that GDd may be an additional risk factor for GO activation, consistently with previous retrospective findings by our group (11) who found a significantly greater proportion of GO reactivation in patients with recent onset hyperthyroidism (less than five years) than in those with disease of longer duration.
In this study, we administered a course of prophylactic steroid therapy in all patients with GDd <5 years and did not observe reactivation or de novo occurrence of GO. Control patients, who have a disease duration of more than five years, and not receiving prophylactic steroids, also did not activate or develop GO. Reasons for an increased risk of GO activation in patients with more recent disease are the presence of larger lymphocytic infiltrates in the thyroid (16,17) and in the orbital tissues (18 –20) giving an increased susceptibility for antigenic stimulation. In contrast, patients with long standing disease, stable euthyroidism, and burnt out orbitopathy are less likely to harbor lymphocytes in the target tissues. In a recent meta-analysis, Shiber et al. (7) reported that while steroid prophylaxis has been shown to be effective in preventing reactivation of GO in patients with pre-existing inactive GO, there are still inconclusive data on the effect of steroids in preventing de novo occurrence of GO. Factors that have been known to confer risk for GO activation are elevated serum TRAb levels (12,21,22), cigarette smoking (23), severe hypothyroidism after RAI (4), the degree of T3 levels at diagnosis (24), and pre-existing active GO (25). In the study of Tallstedt et al. (24), an increased risk of developing GO was observed in hyperthyroid patients with more significant serum pretreatment concentrations of total T3 and treatment with RAI. According to the interpretation of these authors, higher serum T3 concentrations may indicate more severe immunologic reactivity that predispose patients to GO. Since in this study patients with or without pre-existing GO did not differ for known risk factors for GO activation, prophylactic steroids were used in patients with disease duration <5 years, who were considered at increased risk of developing or activating GO than those with duration >5 years. The lack of GO activation observed in both patient groups suggests that we can confidently prevent GO with low-dose steroids even in patients without pre-existing GO and a short duration of disease. This prospective randomized study also shows that oral and intravenous steroid prophylaxis are equally effective in preventing the occurrence of GO after RAI therapy, whether patients had pre-existing or no GO. Randomization of patients to receive OGCs or IVGCs, with an equivalent total cumulative dose of steroids, did not significantly affect the study outcome, therefore, not confirming the better efficacy of IVGCs shown in a previous retrospective study (11).
We followed patients for 5 years after RAI because the study outcome at 6 months might have missed possible late reactivations of GO. The five-year long follow-up after RAI ablation did not show additional patients with activation or de novo occurrence of GO, with the exception of two patients who developed DON, possibly present subclinically at the time of RAI. This did not overtly manifest until 12 and 20 months after RAI, respectively, thereby making it more likely to be related to the natural course of the disease than RAI therapy itself. At the time of the diagnosis of DON, one patient was euthyroid on LT4 with undetectable serum TRAbs, the other patient had very low titers of serum TRAbs, became euthyroid and responded to high-doses steroids without requiring surgical orbital decompression. In our cohort of patients, we did not observe any influence of smoking on either GO activation or on the outcome of hyperthyroidism, as the number of smokers was not significantly different in the patient groups. When treating Graves' hyperthyroidism, a resulting prolonged or uncontrolled hypothyroid state is known to adversely affect GO (25), especially after RAI (26). Perros et al. (4) have reported that RAI is not associated with GO deterioration when post-RAI hypothyroidism is prevented by early administration of LT4. In this study, LT4 therapy was promptly initiated when the serum TSH was >3.5 mU/L, but 1 woman, who missed the 45-day follow-up visit, presented at 90 days after RAI with moderately active GO and a marked elevation of her TSH. GO spontaneously resolved after restoring euthyroidism one month later.
RAI was effective in controlling hyperthyroidism in ∼80% of patients. Neither GDd nor pretreatment serum TRAb levels showed a relationship with the response rate. Steroid prophylaxis for GO did not affect the outcome of hyperthyroidism after RAI. These results are similar to those of a previous study by Jensen et al. (27), in which steroid therapy was commenced before administering RAI. The efficacy rate was lower (60%), probably because the mean 131I activity administered was lower (376 MBq vs. 600 MBq) (28). TV has been found as the only parameter that influenced the efficacy of therapy, and smaller goiters have been associated with a higher rate of post-RAI hypothyroidism. This finding may be explained by the administration of a fixed dose of RAI that may have been insufficient for larger goiters, if compared with a calculated dose that takes into account the iodine uptake and the TV (28).
It has been shown that TRAbs may play a major role in the worsening of GO and that their titers increase about 4–5-fold at 3 months after RAI treatment (21). In this study, we could confirm that serum TRAb levels increase after RAI, but significantly less in patients subjected to steroid prophylaxis when compared with those not receiving steroids. In particular, steroids appear to blunt the increase of serum TRAbs at 45 days and to delay it at 180 days. In particular, in control patients, the increase of serum TRAb levels after RAI reached a peak at 45 days, whereas in those subjected to prophylaxis, the peak was at 180 days. This protective effect of steroids may play a role in the prevention of GO relapse after RAI therapy although there may be other mechanisms (reduced antigen release, reduced cytokine secretion) that may explain or contribute to this phenomenon (29). Lastly, patients treated with OGCs had a slightly higher incidence of side effects, such as insomnia and gastritis, despite the use of proton pump inhibitors throughout the course of steroid prophylaxis (30). This finding suggests that IVGCs may be preferable to avoid the more relevant untoward effects related to the prophylactic therapy with steroids, although the intravenous route of steroid administration requires in-hospital medical monitoring and loss of few days of work. A limitation of this study is that we did not study a group of patients with GDd <5 years without prophylaxis, based on previous retrospective work (11). We acknowledge that a proportion of patients who do not receive steroids may not develop GO after RAI.
In conclusion, RAI treatment is effective and safe for Graves' hyperthyroidism in patients with and without pre-existing inactive GO. GDd <5 years is confirmed to be a useful criterion to select patients for steroid prophylaxis after RAI with the aim to prevent activation or de novo occurrence of GO. Such prophylactic low-dose steroids do not seem to prevent progression of pre-existing GO to DON in a very small number of patients due to the natural disease course and unrelated to RAI therapy. Steroid prophylaxis, at a cumulative dose of 1.5 g, is effective independently of the route of administration. A better safety profile of IVGCs suggests that this modality of prophylaxis may improve patient compliance.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported, in part, by MIUR, Roma, and by funds of Fondazione Ca’ Granda, IRCCS, Milano, Italy, to M.S.