
Abstract
Background:
Little is known about cancer-related worry in thyroid cancer survivors with favorable prognosis.
Methods:
A diverse cohort of patients diagnosed with differentiated thyroid cancer in 2014–2015 from the Surveillance, Epidemiology, and End Results (SEER) Program registries of Georgia and Los Angeles County were surveyed two to four years after diagnosis. Main outcomes were any versus no worry about harms from treatments, quality of life, family at risk for thyroid cancer, recurrence, and death. After excluding patients with recurrent, persistent, and distant disease, multivariable logistic regression was used to identify correlates of worry in 2215 disease-free survivors.
Results:
Overall, 41.0% reported worry about death, 43.5% worry about harms from treatments, 54.7% worry about impaired quality of life, 58.0% worry about family at risk, and 63.2% worry about recurrence. After controlling for disease severity, in multivariable analyses with separate models for each outcome, there was more worry in patients with lower education (e.g., worry about recurrence, high school diploma and below: odds ratio [OR] 1.78, 95% confidence interval [CI 1.36–2.33] compared with college degree and above). Older age and male sex were associated with less worry (e.g., worry about recurrence, age ≥65 years: OR 0.28 [CI 0.21–0.39] compared with age ≤44 years). Worry was associated with being Hispanic or Asian (e.g., worry about death, Hispanic: OR 1.41 [CI 1.09–1.83]; Asian: OR 1.57 [CI 1.13–2.17] compared with whites).
Conclusions:
Physicians should be aware that worry is a major issue for thyroid cancer survivors with favorable prognosis. Efforts should be undertaken to alleviate worry, especially among vulnerable groups, including female patients, younger patients, those with lower education, and racial/ethnic minorities.
Introduction
Cancer-related worry, which typically centers around uncertainty about the future following a cancer diagnosis, is prevalent among cancer survivors and has the potential to affect their quality of life (1,2). Additionally, cancer-related worry can have emotional and social consequences causing significant disruption in survivors' functional status (1,3). Prior studies on cancer-related worry have focused on survivors of common cancers, such as breast cancer and prostate cancer (4 –7). In these patients, it has been shown that worry varies by sociodemographic factors, such as patient age, and that it persists for several years into survivorship (4,7).
However, due to less research funding, poor media coverage, and the perception that thyroid cancer is a “good cancer” due to its high survival rate, worry in thyroid cancer survivors remains understudied (8 –10). Although the incidence of differentiated thyroid cancer has increased in recent years, mortality in low-risk patients with localized disease remains close to zero percent (11). Therefore, given the excellent long-term survival for the vast majority of thyroid cancer patients, it is sometimes assumed that cancer-related worry is not a problem for these patients.
We hypothesized that despite differentiated thyroid cancer being perceived as a “good cancer,” cancer-related worry is still a major issue for disease-free thyroid cancer survivors (10). To elucidate patterns of cancer-related worry in disease-free thyroid cancer survivors and to identify at-risk patients, we surveyed a diverse cohort of 2215 differentiated thyroid cancer survivors without persistent or recurrent disease, who were reported to the population-based Surveillance, Epidemiology, and End Results (SEER) Program registries of the state of Georgia and Los Angeles County.
Methods
Study population and data collection
The SEER Program was founded by the National Cancer Institute, and it collects and publishes data on cancer incidence and survival from 19 representative geographic locations throughout the United States. The SEER data currently cover ∼34.6% of the population, and the registries supported by this program were designed to facilitate cancer research activities in their covered populations (12). For this current survey study, our sample was identified from the Los Angeles County and Georgia SEER registries to include a large, diverse, contemporary population-based sample of patients with relatively recently diagnosed thyroid cancer.
We surveyed patients aged 18–79 years who were newly diagnosed with differentiated thyroid cancer between January 2014 and December 2015. Patients were identified using the following SEER ICD-O-3 morphology codes for thyroid cancer diagnosis: 8050, 8260, 8340, 8341, 8342, 8343, 8344, 8350, 8450 (papillary thyroid cancer); 8330, 8331, 8332, 8335, 8337 (follicular thyroid cancer); 8290 (Hurthle cell cancer). Other selection criteria included being a resident of Los Angeles County or the state of Georgia at the time of thyroid cancer diagnosis.
The modified Dillman method of survey administration was employed to enhance survey response (13). This method consisted of a $20 cash incentive included in the first mailing, multiple mailings, follow-up phone calls, tracing of nonrespondents, and an offer of a phone interview when appropriate. The survey was written at no more than eighth grade reading level. Since there is a large Hispanic population in Los Angeles, patients with surnames suggesting Hispanic ethnicity were mailed copies of the survey in both English and Spanish. Bilingual interviewers contacted those with Hispanic surnames. Patients completed the surveys two to four years following diagnosis. A double data entry method was used to ensure <1% error. Survey responses, which provided details on patient worry, were linked to clinical data reported by the respective SEER registries.
As shown in Figure 1, there were 4185 response-eligible patients. Per the American Association for Public Opinion Research (AAPOR) definition (14), the survey response rate was 63% (2632/4185) and the cooperation rate was 77% (2632/3435). Since worry was an expected finding in patients with persistent or recurrent disease, we excluded the 232 (8.8%) patients with report of persistent or recurrent thyroid cancer and the 178 (6.8%) patients who did not report disease status. Next, we excluded the seven patients identified through the SEER clinical data to have distant metastatic disease (0.3%) as worry would also be common in these patients. The final cohort included 2215 patients (84.2% of respondents) who self-reported as being disease-free, with expected disease-specific mortality near zero.
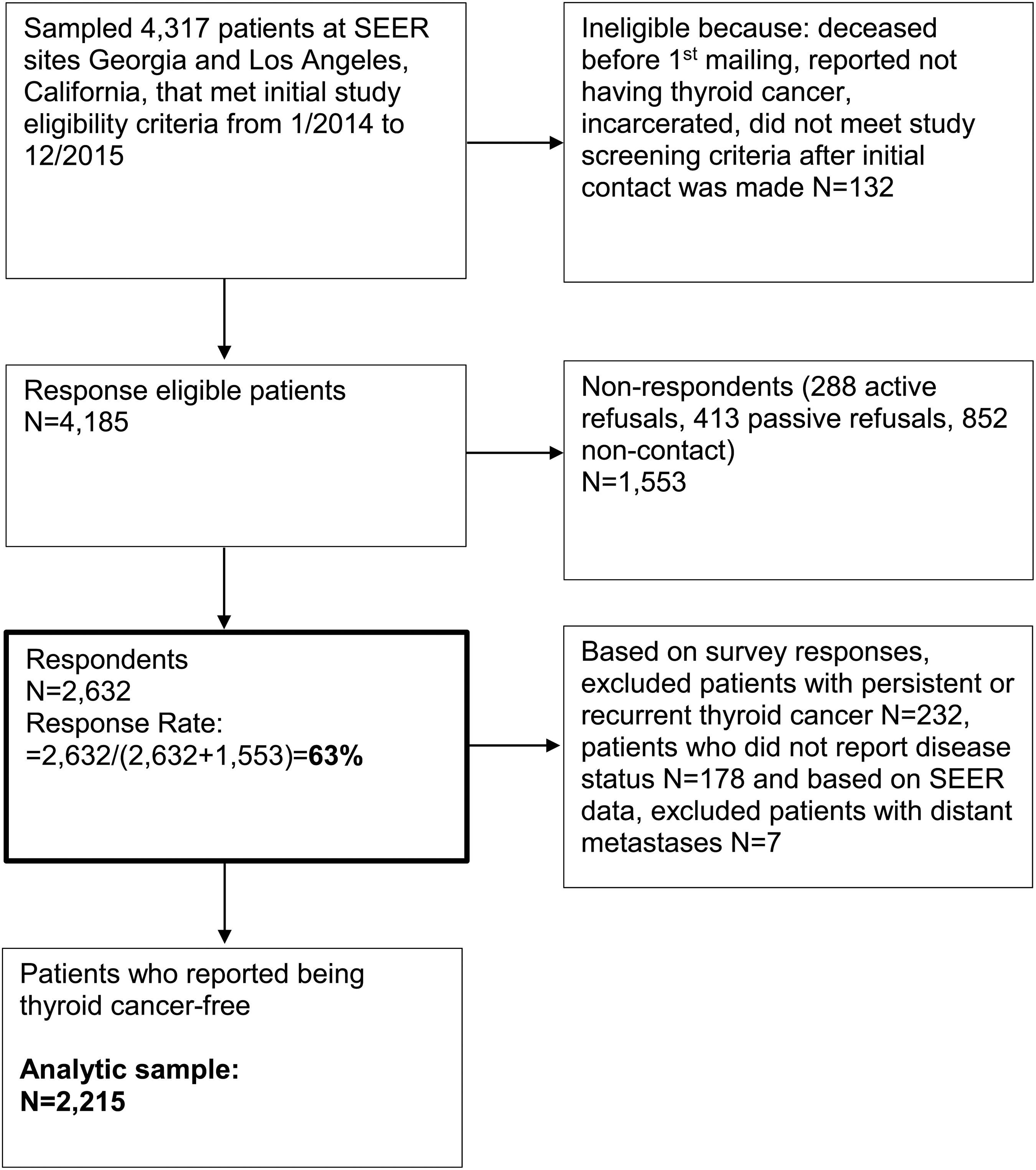
Flow diagram demonstrating sample selection.
The study was approved by the University of Michigan, the University of Southern California, the California Protection of Human Subjects Review Board (California State Institutional Review Board), the Georgia Department of Public Health and the Emory University Institutional Review Board, and received California Cancer Registry approval.
Measures
The survey instrument was developed based on systematic review, prior research in the target population, and input from a multidisciplinary clinical team. Extensive pilot testing was performed in a selected cohort of patients at the University of Michigan. Questions regarding worry were adapted from similar worry scales previously used in studies on breast cancer and cognitively pretested in selected thyroid cancer patients to best fit the population studied (4,15).
Patient report of specific worries
To determine thyroid cancer-related worries, patients were asked to rate how much each of the following factors worried them during the past month: harms from treatments, quality of life not being the same as before the thyroid cancer diagnosis, other family members being at risk for thyroid cancer, thyroid cancer coming back, and death from thyroid cancer. A 5-point Likert scale with the following options was used: not at all, a little, somewhat, quite a bit, and very much.
Patient report of impact of worry on life
Respondents were asked to rate how often their thyroid cancer made it difficult to carry out usual daily activities at home and work, made them feel distant from family and friends, and made them feel upset, both at diagnosis and during the past month. A 5-point Likert scale with the following options was used: never, a little, sometimes, quite a bit, and a lot.
Covariates
Information on patient sex, education (high school diploma and below, some college, college degree and above), race/ethnicity (Hispanic, black, Asian, white, Other), comorbidities, history of other cancers, and self-reported depression before thyroid cancer diagnosis was obtained from the surveys. Regarding race/ethnicity, patients were asked to check all options that best described their race/ethnicity. Similar to prior studies, patients who selected multiple options for race/ethnicity (N = 228) were assigned to one category according to the following priority order: Hispanic, black, Asian, white, and other (16,17). Each individual was analyzed as having one race/ethnicity.
Comorbidities were assessed by asking surveyed patients to mark if they had ever been told by a doctor that they had any of the following before their thyroid cancer diagnosis: heart disease such as coronary artery disease or heart failure, stroke, diabetes mellitus, gastroesophageal reflux disease (GERD), kidney disease, liver disease, chronic lung disease such as chronic bronchitis or emphysema, arthritis, and other cancer. Cancers included were breast, lung, kidney, lymphoma, uterine/endometrial, colon or rectal, bladder, leukemia, pancreatic, brain, prostate, cervical, melanoma, ovarian, head and neck, and other. Number of self-reported comorbidities was categorized as 0, 1, and ≥2.
Details on patient age at thyroid cancer diagnosis (categorized as ≤44, 45–54, 55–64, and ≥65 years) were obtained from the SEER registries. The age categories chosen were based on age cutoffs per the American Joint Committee on Cancer (AJCC) TNM 7th edition and 8th edition staging for differentiated thyroid cancer (45 and 55 years, respectively) and on a common age cutoff for older adults (65 years), and distributions were assessed. Information on the AJCC TNM 7th edition classification was also obtained from the SEER registries and linked to the survey data. Tumor characteristics collected included the AJCC 7 T classification (T1a, T1b, T2, T3, T4) and lymph node status (N0, N1) at diagnosis. These tumor characteristics were derived from combined clinical and pathological details available in the SEER registries (18).
Statistical analyses
We first generated descriptive statistics for our sample, and nonweighted frequencies were reported. All statistical analyses incorporated weights to account for differential nonresponse and reduce potential nonresponse bias. The weight computation included the use of design weights to account for differential probability of sample selection and nonresponse weights to account for disproportionate nonresponse rates across different patient subgroups.
For the purpose of analyses, patient worry was considered synonymous with any worry, as any worry would be clinically meaningful and actionable in these low-risk, disease-free thyroid cancer patients. Therefore, worry was dichotomized as follows: those who answered “not at all” were considered “not worried”; otherwise, they were considered “worried.”
We examined bivariate associations between covariates, including demographic and clinical variables, and our dichotomous outcomes of specific patient-reported worries using two-sided t-tests and chi-square tests as appropriate. Multivariable logistic regression with separate models for each type of worry (harms from treatments, quality of life not being the same as before the thyroid cancer diagnosis, family at risk for thyroid cancer, recurrence, and death) was used to identify correlates of worry in the 2215 patients who reported being disease-free.
We subsequently conducted sensitivity analyses, first using all five categories of the worry Likert scale (“not at all,” “a little,” “somewhat,” “quite a bit,” and “very much”) and then using a more stringent categorization of worry with the following three categories: “no worry” (those who answered “not at all”), “low worry” (those who answered “a little” or “somewhat”), and “high worry” (those who answered “quite a bit” or “very much”).
Missing data were <5% per survey item, and only cases with no missing data on all variables were used in each model. All statistical analyses were conducted using R version 3.5.1. We used the Wald 95% confidence interval [CI] to determine statistical significance.
Results
Sample characteristics
Table 1 shows the respondent characteristics. Of the 2215 patients who were disease-free after initial treatment, 1726 (78.2%) were female, 1302 (54.3%) were White, and 1035 (47.2%) had a college degree or higher. Most patients had the AJCC 7 classification T1a or T1b (60.0%) and no involved lymph nodes (79.7%) at diagnosis. Approximately one-fifth of respondents (17.4%) reported having been diagnosed with depression before thyroid cancer diagnosis.
Patient Demographics and Tumor Characteristics (N = 2215)
Unweighted number.
Weighted percentage (to compensate for differential probability of selection and survey nonresponse).
Derived from combined clinical and pathological tumor characteristics reported to SEER registries.
AJCC, American Joint Committee on Cancer; SEER, Surveillance, Epidemiology, and End Results.
Thyroid cancer-related specific worries
Figure 2 demonstrates that of the respondents, 41.0% reported worry about death, 43.5% worry about harms from treatments, 54.7% worry about impaired quality of life, 58.0% worry about family at risk, and 63.2% worry about recurrence two to four years following diagnosis.
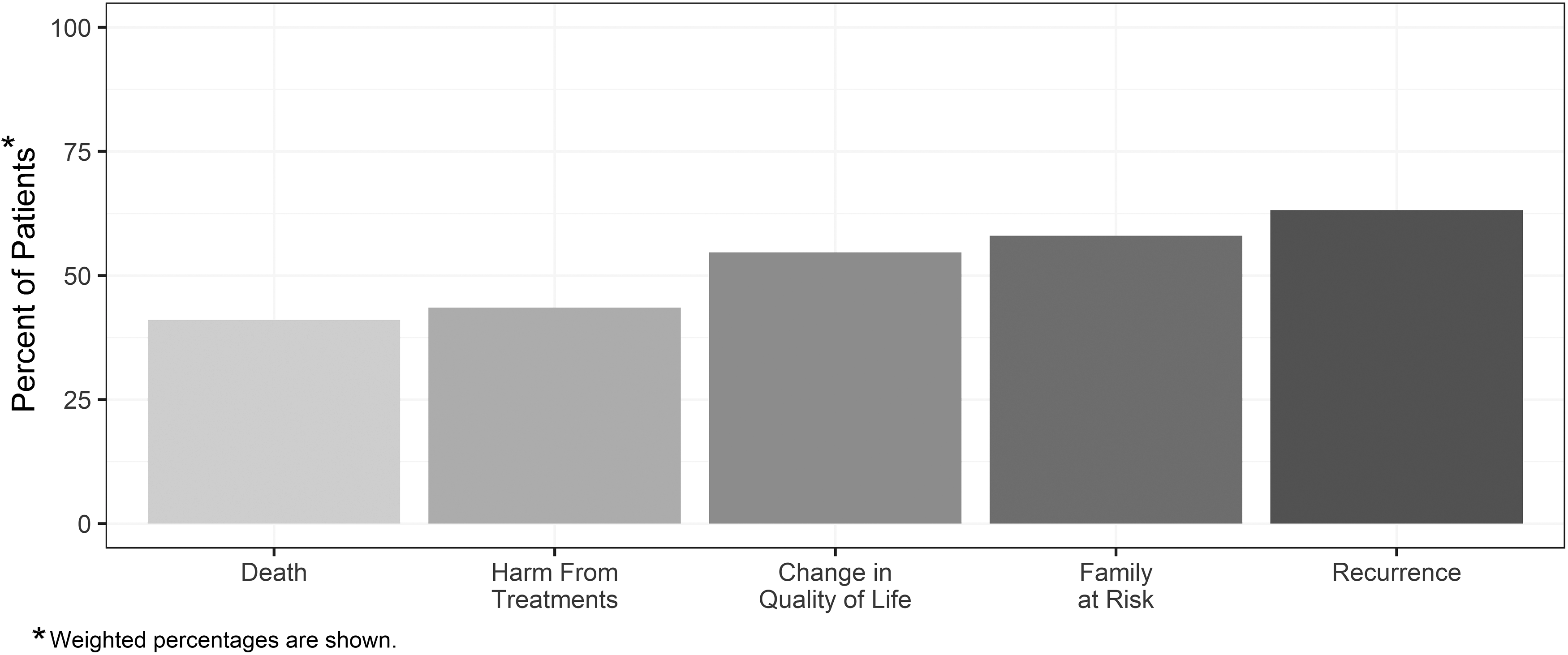
Patient report of specific worries two to four years after thyroid cancer diagnosis (weighted %).
The distributions for each specific worry outcome reported two to four years following diagnosis, excluding missing values, are detailed in weighted percentages as follows: worry about harms from treatments, 56.5% “not at all,” 18.2% “a little,” 13.4% “somewhat,” 5.4% “quite a bit,” 6.5% “very much”; worry about quality of life not being the same as before the thyroid cancer diagnosis, 45.3% “not at all,” 17.8% “a little,” 13.4% “somewhat,” 12.0% “quite a bit,” 11.5% “very much”; worry about family members at risk for thyroid cancer, 42.0% “not at all,” 19.0% “a little,” 17.2% “somewhat,” 10.2% “quite a bit,” 11.7% “very much”; worry about recurrence, 36.8% “not at all,” 23.9% “a little,” 16.8% “somewhat,” 9.1% “quite a bit,” 13.4% “very much,” and worry about death, 59.0% “not at all,” 17.9% “a little,” 9.9% “somewhat,” 3.8% “quite a bit,” 9.3% “very much.”
Figure 3 shows results from multivariable logistic models of patient worry about harms from treatments, quality of life, family at risk, recurrence, and death. After controlling for disease severity, male sex was associated with less worry about harms from treatments and family being at risk compared with female sex (odds ratio [OR] 0.79 [CI 0.62–0.99]; OR 0.64 [CI 0.51–0.80], respectively). Older age was associated with less worry about all outcomes (e.g., worry about recurrence, age ≥65years: OR 0.28 [CI 0.21–0.39] compared with age ≤44 years). Lower education was associated with more worry about all outcomes except worry about quality of life (e.g., worry about recurrence, high school diploma and below: OR 1.78 [CI 1.36–2.33] compared with college degree and above).

Multivariable analyses of patient characteristics associated with specific worries. Specific worries include harm from treatments, quality of life not being the same as before thyroid cancer diagnosis, family members at risk for thyroid cancer, recurrence, and death.
Asians and Hispanics were more worried than whites regarding harms from treatments (OR 1.60 [CI 1.15–2.23]; OR 1.81 [CI 1.39–2.36], respectively). Additionally, Hispanics were more worried about quality of life and family at risk (OR 1.46 [CI 1.12–1.90]; OR 1.51 [CI 1.14–1.99], respectively), and both Asians and Hispanics were more worried about death compared with whites (OR 1.57 [CI 1.13–2.17]; OR 1.41 [CI 1.09–1.83], respectively). Patients with a prior diagnosis of depression were more likely to be worried about impaired quality of life (OR 1.31 [CI 1.03–1.66]). Finally, patients with two or more comorbidities were more likely to be worried about harms from treatments and death (OR 1.47 [CI 1.09–1.98]; OR 1.39 [CI 1.02–1.89], respectively). For a complete set of results, see Table 2. Overall, the trends were the same for the different worry outcomes by degree of worry in the sensitivity analyses.
Multivariable Analyses of Patient Characteristics Associated with Specific Worries (N = 2215)
Bold values depict statistically significant results.
CI, 95% confidence interval; OR, odds ratio.
Patients who reported a history of other cancer(s) before their thyroid cancer diagnosis (N = 292) had significantly less thyroid cancer-related worry about quality of life (p = 0.001), worry about family at risk (p < 0.001), worry about recurrence (p < 0.001), and worry about death from thyroid cancer (p < 0.001) compared with those patients who did not have a history of other cancer(s) (data not shown).
Impact of worry on patients' lives
Figure 4 illustrates the impact of worry on patients' lives at thyroid cancer diagnosis and two to four years following diagnosis. At diagnosis, 63.1% of the respondents reported that worrying about their thyroid cancer made it difficult to carry out their daily activities, 44.8% that it made them feel distant from family and friends, and 88.2% that it made them feel upset.
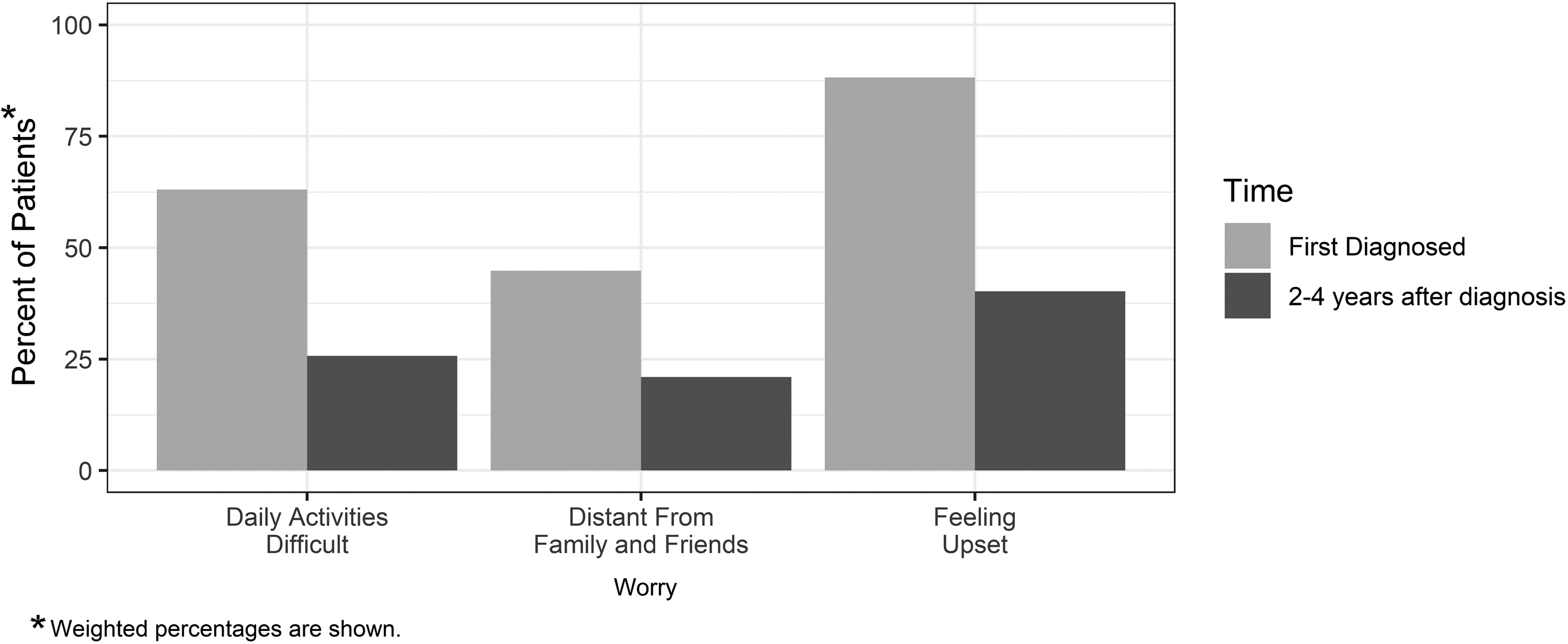
Impact of worry on patients' lives (weighted %).
The complete distributions, excluding missing values, are detailed in weighted percentages as follows: worry made it difficult to carry out daily activities, 36.9% “never,” 19.9% “a little,” 16.9% “sometimes,” 12.1% “quite a bit,” 14.1% “a lot”; worry made them feel distant, 55.2% “never,” 14.1% “a little,” 12.6% “sometimes,” 6.9% “quite a bit,” 11.1% “a lot”; worry made them feel upset, 11.8% “never,” 20.1% “a little,” 17.1% “sometimes,” 23.3% “quite a bit,” 27.7% “a lot.” Two to four years following diagnosis, only 25.8%, 21.0%, and 40.2% of patients reported these concerns, respectively, during the past month. The complete distributions, excluding missing values, are detailed in weighted percentages as follows: worry made it difficult to carry out daily activities, 74.2% “never,” 12.1% “a little,” 7.1% “sometimes,” 2.9% “quite a bit,” 3.6% “a lot”; worry made them feel distant, 79.0% “never,” 9.0% “a little,” 6.7% “sometimes,” 2.8% “quite a bit,” 2.5% “a lot”; worry made them feel upset, 59.8% “never,” 19.5% “a little,” 13.1% “sometimes,” 3.7% “quite a bit,” 3.8% “a lot.”
Discussion
Our study demonstrates that cancer-related worry is still common in disease-free thyroid cancer survivors, even two to four years following diagnosis and despite thyroid cancer being perceived as a “good cancer.” Common patient-reported worries include worry about harms from treatments, quality of life not being the same as before diagnosis, family members being at risk for thyroid cancer, recurrence, and death. Not surprisingly, diagnosis with more advanced disease and younger age are associated with thyroid cancer-related worry. Less expected was the finding that female sex, lower education, and being a racial/ethnic minority were also associated with more worry.
Our finding that Hispanics and Asians were more likely to worry about harms from treatments and death compared with whites indicates a need to focus on these populations with interventions to reduce unnecessary worry. Additionally, the fact that Hispanics were also more worried about other aspects of thyroid cancer such as quality of life and family being at risk points to them as being a particularly vulnerable group. These results provide new insight on the role of race/ethnicity on cancer-related worry in thyroid cancer survivors that has so far been lacking.
Studies in breast cancer survivors have shown that worry differs across racial/ethnic groups, with Latinas more likely to express concerns regarding death, and experience emotional distress and social disruption compared with whites and blacks (4,5,19). It is plausible that cultural differences and divergent social support systems also extend to thyroid cancer survivors and may impact perception of worry, likelihood, or willingness to report it and coping mechanisms (20). Additionally, language barriers and low acculturation may also play a role.
Consistent with studies of patients with other malignancies, we found that older age was associated with less report of any worry (1,4,19,21,22). It has been previously shown that younger age is associated with increased fear of recurrence and psychological distress, even several years following initial treatment, in both breast cancer and prostate cancer survivors (4,5,7,23,24). Possible explanations for this trend may include the fact that younger patients are more likely to have healthy peers, be of reproductive age or have young children, or trying to accomplish financial independence, thus making a cancer diagnosis more stressful.
Harms from treatments and impaired quality of life were reported worries. Worry about harms from treatments was prominent among females, younger patients, Hispanics and Asians, as well as those with lower education, advanced disease, and prior diagnosis of depression. We also found that disease-free low-risk thyroid cancer patients worry about impaired quality of life, a finding consistent with a prior smaller study (N = 153) of patients cured of differentiated thyroid cancer (25). With marked variation in all aspects of management (surgery, radioactive iodine, and thyroid hormone suppression therapy), especially for low-risk thyroid cancer patients, some patients may be at risk for overtreatment conferring unnecessary harms, which in turn may lead to worry and impact their long-term quality of life (26 –28).
More than half of surveyed patients reported worry about family members being at risk for thyroid cancer, with females, Hispanics, and those with lower education being most at risk for worry. Considering epidemiological data showing that only 5–10% of differentiated thyroid cancers have a familial occurrence, it is unclear where this worry stems from and may highlight the need for more patient education (29).
Worry about recurrence was the most common reported worry in this disease-free thyroid cancer cohort. Prior studies focusing on breast cancer and prostate cancer have shown that worry about recurrence is prevalent, even in low-risk cancer patients (5,7,24). For example, in a survey of a diverse cohort of women with ductal carcinoma in situ or invasive breast cancer, identified by the Detroit or Los Angeles SEER registries (N = 2290), 27.2% reported some, quite a bit, or a lot of worry about recurrence four years after diagnosis (5). Even though the worry scale we used for our study was adapted from this prior study, their cohort included high-risk patients with invasive breast cancers, and therefore, in this prior study, the scale was dichotomized differently (no worry: not at all/a little, and worry: some/quite a bit/a lot). However, recognizing that worry is also a common theme for other cancers, we adapted and utilized this scale in thyroid cancer patients with a favorable prognosis in whom many physicians assume no worry.
Studies on thyroid cancer-related worry are scarce. Consistent with our study, previous studies focusing specifically on thyroid cancer survivors have shown that fear of recurrence was common among young survivors and significantly impacted patients' health-related quality of life (30,31). In a population-based cohort study of Swedish patients with differentiated thyroid carcinoma surveyed by mail 14–17 years following their diagnosis (N = 353), 48% reported fear of recurrence. Moreover, this study interestingly showed that fear about recurrence had an equal influence on quality of life as having a recurrence (30).
Additionally, in a cross-sectional mailed survey study of Canadian thyroid cancer survivors (N = 941), worry about recurrence was prevalent (mean worry score 2.60 with standard deviation 0.98, on a scale from 1 [least worry] to 4 [most worry]), with younger age being one of the strongest predictors of cancer-related worry in multivariable analyses (31). In contrast to these prior studies, our study has a larger cohort, includes a diverse patient population with representation of Hispanic, Asian, and black patients, and includes details on tumor characteristics, such as the presence of lymph node metastases.
Surprisingly, worry about death was reported by 40% of disease-free thyroid cancer survivors cured of low-risk disease, despite the excellent survival of patients with differentiated thyroid cancer compared with patients with other malignancies. Several studies investigating worry about death in patients with other cancer types focused on patients with advanced cancers (32,33). To our knowledge, only one other study investigated worry about death in thyroid cancer patients, but this study lacked data on disease severity at time of diagnosis and included patients with persistent and recurrent disease. This prior study (N = 941) demonstrated heightened worry about death in thyroid cancer survivors (mean worry score 2.12 with standard deviation 0.99, on a scale from 1 [least worry] to 4 [most worry]), particularly those with younger age, suspected residual disease, and those ≤5 years since thyroid cancer diagnosis (31).
A major strength of our study is the combination of SEER registry data, which offer important details on thyroid cancer and its treatment, and a complementary patient survey, which provided granular details on patient worry. This study design allowed us to focus on worry in patients who are disease-free with near zero risk of disease-specific mortality. Collaboration with the Georgia and Los Angeles County SEER sites allowed for a diverse patient cohort with adequate representation of black, Asian, and Hispanic patients, and patients living in both rural and urban settings.
Additional strengths include the large population-based sample size, strong response rate among surveyed patients, few missing data, and our ability to control for patient report of a prior diagnosis of depression. The study also has some limitations. Although recall bias is a common risk with studies focused on patient-reported outcomes, most of the survey questions on the primary outcome for this study, thyroid cancer-related worry, focused on worry during the past month. Of note, associations observed in the study are not necessarily causal.
The results of this study have implications for both patients and physicians. Even though the mortality from well-differentiated thyroid cancer is low, worry is prevalent and varies by age, sex, level of education, race/ethnicity, and disease severity. This worry suggests a disconnect between actual thyroid cancer risks and patient perceptions of risk. Additionally, it is important to consider the potential impact of fear of recurrence and death on thyroid cancer survivors' long-term surveillance. Prior work has shown increased use of post-treatment imaging surveillance in thyroid cancer patients (34,35), and it is possible that patient worry may be driving this phenomenon.
Furthermore, patient worry does impact cancer care. Our prior work showed that physicians place importance on both physician and patient worry about death when deciding whether to treat a thyroid cancer patient with radioactive iodine, with this worry being more influential for physicians with low case volume (36). Since thyroid cancer mortality is low, this worry about death, in addition to worry about recurrence, may be an inappropriate driver for more intensive care, even in low-risk patients. Although the impact of worry on day-to-day life improves over time, it is still greater than expected in thyroid cancer survivors with a favorable prognosis. Thus, there is still a need to reduce worry across the care trajectory in at-risk patients through education and culturally sensitive targeted interventions.
Footnotes
Acknowledgments
This work is supported by R01 CA201198 from the National Cancer Institute (NCI) to Dr. Haymart. Dr. Haymart is also supported by R01 HS024512 from AHRQ and Dr. Papaleontiou by K08 AG049684 from the National Institute on Aging. The collection of cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885, Centers for Disease Control and Prevention's (CDC) National Program of Cancer Registries, under cooperative agreement 5NU58DP006344, and the NCI's SEER Program under contract HHSN261201800015I awarded to the University of Southern California. The collection of cancer incidence data in Georgia was supported by contract HHSN261201800003I, Task Order HHSN26100001 from the NCI, and cooperative agreement 5NU58DP003875-04 from the CDC. The ideas and opinions expressed herein are those of the authors and endorsement by the State of California and State of Georgia Departments of Public Health, the NCI, and the CDC or their Contractors and Subcontractors is not intended nor should be inferred.
Author Disclosure Statement
No competing financial interests exist.