
Abstract
Background:
Studies differ regarding whether, compared with courses of conventional duration, longer-term antithyroid drug treatment increases frequency of remission in patients with Graves' hyperthyroidism. We prospectively conducted a randomized, parallel-group study comparing relapse rates in patients receiving longer-term versus conventional-length methimazole therapy. We also sought variables associated with relapse following the latter.
Methods:
We enrolled 302 consecutive patients with untreated first episodes of Graves' hyperthyroidism. After 18–24 months of methimazole, 258 patients (85.4%) were randomized to an additional 36–102-month courses (“long-term group”: n = 130; scheduled total time on methimazole: 60–120 months) or discontinuation of methimazole (“conventional group”: n = 128). Patients were followed 48 months postmethimazole cessation. We performed Cox proportional hazards modeling to identify factors associated with relapse after conventional courses.
Results:
Methimazole was given for 95 ± 22 months in long-term patients and 19 ± 3 months in the conventional group. Fourteen patients experienced cutaneous reactions and 2 liver enzyme elevations during the first 18 months of treatment; no further methimazole-related reactions were observed despite therapy for up to another 118 months. Hyperthyroidism recurred within 48 months postmethimazole withdrawal in 15% (18/119) of long-term patients versus 53% (65/123) of conventional group patients. In the conventional group, older age, higher triiodothyronine or thyrotropin receptor antibody concentrations, lower thyrotropin concentration, or possession of the rs1879877 CD28 polymorphism or the DQB1-05 HLA polymorphism were independently associated with relapse.
C
Introduction
Over the past 70 years, millions of patients with Graves' hyperthyroidism were effectively treated with thionamide antithyroid drugs (ATDs) (1). However, these treatments have an important drawback: high recurrence rates, estimated at 51% to 68% in one systematic review (2). Surprisingly given the drugs' longstanding widespread use, the optimal duration of ATD therapy to minimize relapse frequency remains unclear (2,3). Historically, a ∼30% to 40% remission rate was attained with 12–18-month courses of therapy and this duration has been considered the upper limit of the duration of treatment (2,4). However, a few studies (2,5 –7) and a recent meta-analysis (8) suggested that longer-term ATD treatment of hyperthyroidism may be associated with higher remission rates, with a low frequency of drug-related complications.
Resolving how long to give ATDs has been hampered by the generally small sample sizes and sometimes short follow-up of studies examining the question (8). We therefore conducted a trial with a relatively large sample size and longitudinal surveillance for several years to compare rates of remission of hyperthyroidism in patients with longer-term versus conventional ATD therapy. We also sought to identify those patients receiving conventional therapy who might be high-priority candidates for longer ATD treatments by determining variables associated with relapse in such individuals. In view of the importance of genotype and HLA subtypes in predicting relapse of hyperthyroidism, we have added these variables to clinical and demographic factors to address this important aspect (9).
Methods
Study design, endpoints, and oversight
We conducted a prospective, single-center, randomized, parallel-group trial from October 2001 to March 2017 in an iodine-sufficient area (10). The local Ethics Committee approved the protocol before initiating the investigation; all patients provided written informed consent.
Consecutive patients with untreated first episodes of Graves' hyperthyroidism were enrolled. After methimazole courses of conventional duration (18–24 months), patients were randomized 1:1 by using the Table of Random Digits to continue methimazole until the drug was given for altogether 60–120 months, or to discontinue the drug (“long-term” or “conventional” groups, respectively).
The primary endpoint was relapse of overt hyperthyroidism after methimazole discontinuation. Overt hyperthyroidism was defined as serum thyrotropin <0.4 mIU/L plus serum free thyroxine (fT4) >23 pmol/L, serum triiodothyronine >2.7 nmol/L, or both; these thresholds comprised relevant institutional limits of reference ranges for the respective analytes (11).
Key secondary endpoints were occurrence of subclinical hyperthyroidism or overt or subclinical hypothyroidism during or after methimazole treatment. Subclinical hyperthyroidism was defined as thyrotropin <0.4 mIU/L with normal fT4 and triiodothyronine levels. Overt hypothyroidism was classified as thyrotropin >5.09 mIU/L, the upper limit of normal for the general population in Tehran (11) plus fT4 < 9 pmol/L. Subclinical hypothyroidism was defined as thyrotropin >5.09 mIU/L with normal fT4 and triiodothyronine concentrations.
Safety was assessed based on treatment-emergent adverse events observed by caregivers or reported by patients spontaneously or after questioning; we rated these events as related or unrelated to methimazole.
Patients
Patients were eligible if they had not previously received ATDs, radioiodine, or thyroidectomy. Other key inclusion criteria were age ≥19 years; biochemical overt hyperthyroidism; and no history or evidence of cardiovascular disease, chronic heart failure, chronic kidney disease, or cirrhosis. Important exclusion criteria included pregnancy, breastfeeding, or altered mental function. Thyroid scintigraphy was performed in most patients to exclude the existence of Graves' disease, in addition to pre-existing nodular goiter.
Methimazole therapy
Methimazole was given once daily at 20–30 mg/day for the first month. Through a titration method, this dose was respectively tapered or increased at each subsequent study visit as the patient became euthyroid or remained hyperthyroid. Goals of therapy were to maintain normal fT4 (10–23 pmol/L) and thyrotropin (<5.09 mIU/L) levels. Patients in the long-term group began their additional course of methimazole at the ending dose of their initial course, with further titration as needed to meet biochemical targets.
The precise durations of the initial 18–24-month methimazole course (all patients) and the additional course for a total of 60–120 months (long-term patients) were determined based on patient preference, visit intervals, or elevated risk of hypothyroidism with continued therapy, reflected by methimazole dose titration repeatedly failing to prevent increasing thyrotropin levels.
Procedures
At entry, demographic variables were obtained, and goiter size was assessed by palpation according to the World Health Organization criteria (12). Orbitopathy was rated as absent (Werner's class 0–1) or present (Werner's class 2–6: inflammatory signs, proptosis, extra-ocular muscle, or corneal involvement) (13). Patients were scheduled to be seen at 1, 2, 3, 6, 9, 12, 18, and 24 months prerandomization and every 6 months thereafter until 48 months postmethimazole discontinuation.
Biochemistry
Nonfasting venous blood samples were taken at each visit to determine serum thyrotropin, fT4, triiodothyronine, and thyrotropin receptor antibody (TRAb) concentrations. Samples were assayed immediately after blood draws, since treatment decisions were influenced substantially by biochemistry findings. Assay runs were performed in duplicate, by staff blinded regarding the treatment protocols of the patients.
From 2001 to 2005, thyrotropin was measured by immunoradiometric assay using kits (Izotop, Budapest, Hungary), fT4 and triiodothyronine by radioiomunoassay (DiaMetra, Milan, Italy), and TRAb, by enzyme-linked immunoabsorbent assay (Bio Vendor Laboratory Medicine, Inc., Czech Republic). Subsequently, these analytes were measured by electrochemiluminescence immunoassay (Roche Diagnostics GmbH, Mannheim, Germany). For all tests, interassay and intraassay coefficients of variation were <6.1% and <9.1%, respectively. Measurements took place in the laboratory of our institution.
Genotyping
Genetic polymorphism analyses were performed on one sample per patient. Immediately after peripheral blood leukocyte collection, genomic DNA was extracted by using standard salting out/proteinase K methodology, and polymerase chain reaction (PCR)-based testing was performed. PCR products were stored at −20°C at the end of PCR runs. DNA purity was determined via the A260/A280 absorbance ratio by using a NanoDrop micro-volume spectrophotometer (Thermo Fisher Scientific, Waltham, MA).
Genetic factors, including single-nucleotide polymorphisms (SNPs), have been implicated in susceptibility to Graves' disease (3,14). We therefore tested for eight SNPs, CD40C/T (rs11569309), CD40C/T (rs745307), CD40A/G (rs3765457), CD28A/C (rs1879877), CTLA-4C/T (rs5742909), CD28G/T (rs3181113), CTLA-4A/G (rs231775), and PTPN22C/T (rs2476601), using tetra-primer amplification refractory mutations system PCR (15,16). Electrophoresis of PCR products was performed on silver nitrate-stained 8% polyacrylamide gels.
Given the suggested role for some HLA subtypes in susceptibility to Graves' disease (3), HLA typing (subtypes DRB and DQB) at the allele level was also carried out by using a DNA-based method employing sequence-specific primers. The Morgan™ HLA sequence-specific primer DRB/DQB Typing Kit (TBG Diagnostics Ltd., Greenslopes, QLD, Australia) and the PCR-based method specified per manufacturer's protocol were utilized. For HLA typing, final PCR products were run on 2% agarose gel electrophoresis; bands were documented by using the safeVIEW–MINI2 ultraviolet transilluminator (Cleaver Scientific Ltd., Rugby, Warwickshire, United Kingdom). Specific and internal control bands were interpreted per manufacturer's instructions.
Statistics
Sample size was calculated assuming that the relapse rate would decrease from a 50% “best-case scenario” documented with conventional methimazole treatment (2) to the 30% previously noted with longer-term therapy (8). Assuming a one-sided type 1 error of 0.05 and a power of 90% generated sample sizes of 111 in each treatment group.
Baseline variables were compared with Student t, Mann–Whitney, chi-square, or Fisher exact testing, as appropriate. Time-to-relapse of Graves' hyperthyroidism after methimazole cessation was documented by using Kaplan–Meier curves, and it was compared between groups by using log-rank testing. The number-needed-to-treat with our longer-term regimen to attain one incremental remission relative to results with conventional therapy was calculated by inverting the difference between the conventional and long-term groups in cumulative incidence of relapse at 48 months postmethimazole withdrawal.
We used Cox proportional hazards modeling to compute crude and adjusted hazard ratios (HRs) of relapse for long-term therapy versus conventional therapy. HRs appear with their 95% confidence intervals.
Cox proportional hazards modeling was also used to assess potential predictors of relapse in the conventional group. Clinical and demographic variables were included in a preliminary model based on expert opinion; significant predictors were selected by using a forward stepwise method with p < 0.2 as the entry criterion and p > 0.1 as the removal criterion. Likelihood ratio testing revealed that adding genetic factors significantly improved the model's predictive performance (data not shown); therefore, we also assessed all such factors with ≥10% prevalence in our sample by using the same entry and removal criteria. Allele frequencies were estimated by direct gene counting. For each polymorphism, Hardy–Weinberg equilibrium was evaluated by using chi-square testing. To adjust for multiple testing, we used permutation to obtain empirical p-values for each SNP.
The trends of methimazole dose and thyroid analyte values during longer-term therapy were compared between patients relapsing by the end of the 48 months' post-therapy follow-up and those remaining in remission, using marginal models (general estimation equation).
Except for model variable selections, p < 0.05 was considered significant. Statistical analysis was performed by using SPSS 20 (SPSS, Inc., Chicago, IL) and STATA 14 (Stata Corp., College Station, TX).
Results
Patient characteristics
The patient characteristics are summarized in Figure 1. Three hundred two patients with diffuse toxic goiter were enrolled, of whom 258 (85.4%) completed the prerandomization methimazole course. For the 258 patients, the mean duration of that course was 19 ± 3 months, and the median duration was 18 months.

Study enrollment and follow-up for recurrence of hyperthyroidism. MMI, methimazole.
Of the 44 patients (14.6%) not completing the initial course, 12 relapsed, 3 became hypothyroid, 6 chose ablative therapy due to insufficient control of hyperthyroidism, 12 changed to other treatments due to methimazole side effects, and 11 were lost to follow-up. Overall, 44 subjects were excluded from the study before randomization.
Among the 258 randomized patients, 128 were assigned to discontinue methimazole, and 130, to receive longer-term administration. Of the 130, 121 (93%) completed their additional course; mean and median total times on methimazole were 95 ± 22 and 96 months, respectively. During the extended treatment, none of the 121 experienced overt hyperthyroidism. However, 197 (7.7%) of their 2551 serum samples taken during the additional course had thyrotropin levels <0.4 mIU/L, which was managed by 2.5–5 mg increases in daily methimazole doses. In addition, 174 (6.1%) of the samples had thyrotropin levels >5.09 mIU/L, which was managed by reducing methimazole dosage.
Of the nine assigned patients (7%) not completing extended methimazole courses, four relapsed and underwent radioiodine therapy, one became hypothyroid, and four were lost to follow-up. All nine were excluded from the study.
Table 1 compares patient characteristics at enrollment and at randomization by treatment group. Included are randomized patients who received scheduled follow-up and were euthyroid or overtly hyperthyroid at final assessment (n = 119/130, 92% of long-term patients, n = 121/128, 95% of conventional therapy patients). The groups were similar in age and sex composition. At enrollment, they differed only in that eventual long-term patients had a significantly greater prevalence of larger (grade 2) goiters. After the prerandomization methimazole course, the groups differed biochemically only in that the conventionally treated patients had significantly lower mean thyrotropin concentrations.
Patient Characteristics by Study Arm at Study Entry and After Prerandomization Course of Methimazole
fT4, serum-free thyroxine; NS, not statistically significant; T3, serum triiodothyronine; TRAb, serum thyroid receptor antibodies; TSH, serum thyrotropin.
Biochemical outcome
By 48 months postmethimazole discontinuation, relapse of overt hyperthyroidism had been detected in 65 of 123 conventional patients (53%), versus 18 of 121 (15%) long-term patients (p < 0.001) (Fig. 2). There was no difference in remission rates between the first and second half of the study period in the conventional group. Transient subclinical hyperthyroidism was present in 12 of 123 (10%) of the conventional group and 10 of 121 (8%) of the long-term group; since affected patients were <65 years old and developed no overt hyperthyroidism during follow-up, they were left untreated.

Kaplan–Meier curve for relapse of hyperthyroidism in patients with Graves' disease after methimazole withdrawal. The conventional group received a total of 15 to 24 months, and the long-term group, a total of 60 to 120 months, of methimazole treatment.
By the end of the follow-up, 56 of 123 conventional-group patients (46%) were in remission and 2 (2%) were overtly hypothyroid, compared with 101 (83%) and 2 (2%), respectively, of 121 long-term patients. For longer-term methimazole, the number-needed-to-treat was 2.6 per remission. The HR of relapse into overt hyperthyroidism for the long-term group relative to the conventional group was 0.20 (0.12–0.34) before and 0.16 (0.08–0.30) after statistical adjustment for baseline characteristics. When one considers the additional treatment period plus the subsequent 48-month follow-up in patients randomized to extended methimazole therapy, relapse into overt hyperthyroidism was observed in 22 of 130 (17%) patients, and development of overt hypothyroidism was observed in 3 patients (2%).
Factors associated with relapse: conventionally treated patients
In univariate analyses, factors associated with relapse of overt hyperthyroidism in the conventional group were older age, higher serum TRAb, and higher methimazole dose on medication withdrawal. In multivariable analysis, higher triiodothyronine and lower thyrotropin concentrations at methimazole discontinuation joined these factors as significant predictors (Table 2). Among genetic variables examined, only the CD28 polymorphism rs1879877 and HLA polymorphism DQB1-05 were statistically associated with relapse.
Univariate and Multivariate Hazard Ratios (95% Confidence Intervals) for Selected Potential Predictive Factors for Relapse of Hyperthyroidism After Conventional-Length Methimazole Therapy
CI, confidence interval.
Trends in thyroid-related analytes and methimazole dose: long-term group
Throughout the first 4 years on methimazole, patients who relapsed during the 48-month post-treatment follow-up and those remaining in remission throughout that period did not differ in mean thyroid-related analyte concentrations (Fig. 3 and Supplementary Table S1). However, at the end of methimazole treatment, mean fT4, triiodothyronine, and TRAb concentrations were significantly higher, and thyrotropin levels were significantly lower in patients who ultimately relapsed. Average methimazole dosage did not differ at either time point.
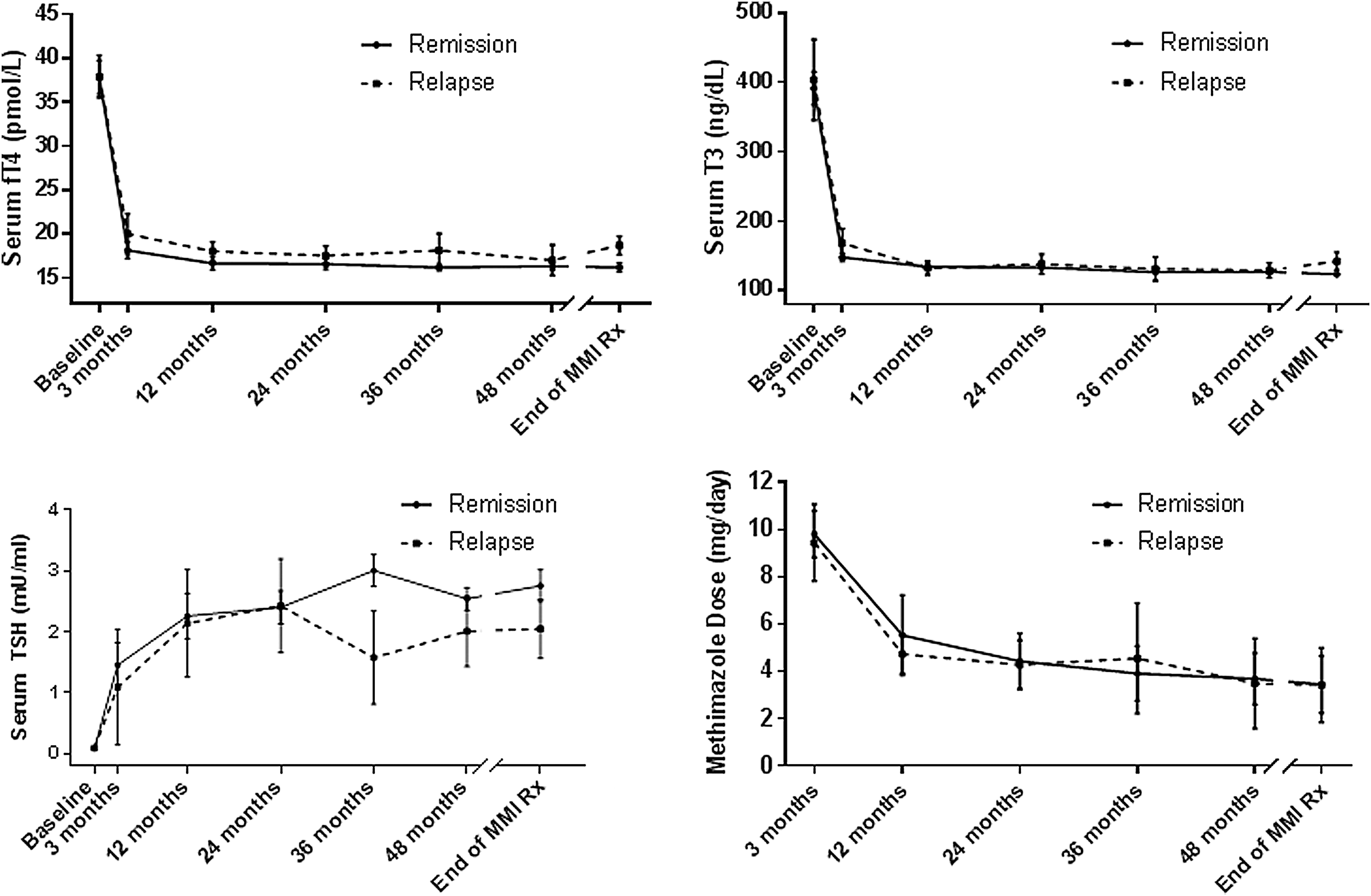
Serum fT4, triiodothyronine, and thyrotropin concentrations, and ending methimazole dose in long-term group patients, according to eventual remission or eventual relapse of hyperthyroidism.
Safety
During the prerandomization methimazole course, 16 of 302 patients (5.3%) experienced adverse effects deemed to be drug related, all within the first 2 months. Fourteen patients (4.6%) developed skin reactions, of whom 4 individuals were effectively treated with antihistamines and 10 shifted to propylthiouracil treatment. Two other patients (0.7%) had elevated liver enzymes and chose radioiodine therapy. No serious complications, for example, agranulocytosis, or unexpected drug-related adverse events were noted. No side effects were observed from month 3 through the end of up to 120 total months on methimazole. With respect to increased morbidity and mortality of subclinical hyperthyroidism, methimazole dose adjustment prevented long-term suppression of serum thyrotropin. The longest period of subclinical hyperthyroidism after withdrawal of methimazole was 12 months and occurred in 2 patients.
Discussion
This prospective, randomized trial lasting up to 10 years—the largest yet published addressing the optimal duration of ATD therapy—showed that 60–120 month courses of low-dose methimazole seemingly largely overcame the major limitation of conventional 18–24-month courses of ATD therapy of Graves' hyperthyroidism, that is, relapse in at least half of the patients (2,8). The two study groups were similar in many characteristics at randomization. However, they differed in goiter size, with a higher prevalence of larger goiters in long-term treated patients. Although we did not match for goiter size before randomization, large goiter size does not seem to be in favor of a higher remission rate in this group of patients. Our findings of a significantly higher remission rate with protracted versus conventional low-dose methimazole treatment (83% vs. 46%, p < 0.001), obtained with minimal drug-related toxicity, confirm earlier reports (7,8,17) of efficacy and safety of ATD courses exceeding 24 months. In particular, we extend the findings of Mazza et al. (7), who showed that longer-term methimazole treatment prevented relapse of Graves' hyperthyroidism in patients >35 years old, compared with courses of <15 months.
Our observations have potentially important public health implications regarding the most frequent first-line treatment (18 –20) of a common condition that imposes considerable morbidity and financial costs (3,21 –25). Specifically, our results suggest that a majority of patients with hyperthyroidism could benefit from long-term low-dose ATD therapy or, at a minimum, more patients with Graves' disease. Besides the low costs of these agents, which are widely available as generics, their apparently very low complication rate points to the feasibility of broadly applying very-long-term ATD courses, as has been proposed for children with Graves' disease (26) and patients with Graves' orbitopathy (5,6). Nonetheless, cost-effectiveness studies of extended low-dose ATD therapy are needed, especially in adults.
If long-term ATD therapy is to be used more often, but not given universally to patients with Graves' hyperthyroidism, our results suggest the following high-priority candidates: These patients would be older and have higher triiodothyronine and TRAb levels, as well as lower thyrotropin concentrations, when medication discontinuation is considered. Carriers of CD28 polymorphism rs1879877 or HLA subtype DQB1-05 may also be suitable candidates.
Our results regarding predictors of relapse after conventional methimazole therapy differ from earlier findings that male sex, severe hyperthyroidism pretreatment, large goiter, orbitopathy, and smoking are associated with relapse after ATD withdrawal (27). Our analysis also omitted such factors as family history, tendency for autoimmune thyroid disease, stressful life events, dermopathy, or long delays in beginning ATDs, which have been associated with decreased remission rates (27). A further study of predictors of relapse after conventional-length ATD therapy, for example, goiter grade, ophthalmological findings, and TRAb concentrations, is needed, particularly given the limited predictive performance of factors identified to date.
Although our study investigated the longest methimazole courses yet reported, and suggests that extended versus conventional-length ATD regimens may be superior, our long-term patients had a wide range of total treatment durations from 60 to 120 months. Further study is necessary to more precisely characterize optimal treatment length. It may well be desirable to individualize therapy duration. Our finding that thyroid-related analyses at the end of methimazole therapy are associated with outcome suggests that at least over the long term, these markers might be helpful to guide treatment decisions.
Limitations of our study should be noted. First, the trial involved an ethnically homogeneous sample from West Asia; generalizability to patients of other ethnicities is unclear. Second, since this study was not double-blinded, material biases, including selection and ascertainment biases, cannot be ruled out. Third, since serum TRAb levels were measured only before initiation and at withdrawal of methimazole in every patient, a graph of serial TRAb titers in the long-term group that could assist in determining whether an exact threshold of the long duration therapy occurs cannot be provided.
In conclusion, very-long-term, continuous, low-dose methimazole courses are safe, well tolerated, and a highly effective treatment for Graves' hyperthyroidism. Such therapy is accompanied by much higher remission rates compared with conventional-length methimazole courses and appears to cure a large majority of patients with diffuse toxic goiter.
Footnotes
Acknowledgments
Niloofar Shiva critically edited for English grammar and syntax; Robert J. Marlowe critically edited for English grammar and syntax, organization, and scientific content; and Tahereh Fakhimi prepared the article. The authors thank the patients and their families whose participation made this work possible. They acknowledge the Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Funded by the regular budget of the Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran; registered under identifier 5143 at the Iranian Registry of Clinical Trials,
Authors' Contributions
F.A., Conceptualized and conceived the trial; F.A., A.A., and M.T., designed the trial; F.A. acquired the data; Y.M., L.C., Carried out the statistical analyses; and F.A., A.A., and M.T. drafted the initial article. All authors interpreted the data, revised the article critically for important intellectual content, approved the final version, and agreed to be accountable for all aspects of the work.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1