
Abstract
Introduction:
Prior research has shown an association between breast and thyroid cancers, although their relationship is unclear. In China, asymptomatic women undergoing regular health checkups usually undergo breast and thyroid ultrasonography screening. The present cross-sectional ultrasound-based study estimated the prevalence of breast masses (BM) and thyroid nodules (TN) and their relationship among a population-based cohort of Chinese women.
Methods:
This study included 34,184 consecutive asymptomatic Chinese women who underwent both breast and thyroid ultrasound evaluation during one health care examination. Detected lesions were assigned into categories of different malignant risks according to the Breast and Thyroid Imaging Reporting and Data System (BI-/TI-RADS). Binomial logistic regression was used to determine the association between occurrence of BM and TN, and multinomial logistic regression was used to analyze the correlation of BM and TN in different BI-/TI-RADS categories. Associations between BM and TN, as well as anthropometric and biochemical markers, were also explored.
Results:
Of those enrolled, 6371 (18.6%) had BM, 12,153 (35.6%) had TN, and 2279 (6.7%) had both. After adjusting for age, body mass index (BMI), and height, females with TN had a higher risk of BM (odds ratio [OR] = 1.151, 95% confidence interval [CI 1.081–1.225], p < 0.0001) than those with normal thyroids, and females with BM had a higher risk of TN (OR = 1.165 [CI 1.096–1.238], p < 0.0001) than those without BM. Women with a TN >10 mm (OR = 1.249 [CI 1.104–1.413], p = 0.0004) and those with a TN ≤10 mm (OR = 1.134 [CI 1.062–1.211], p = 0.0002) were at higher risk of BM compared with those with normal thyroids. As RADS categories increased, so did the correlation between BM and TN. The increased risk of TN was associated with a higher BMI, height, systolic blood pressure, and a lower plasma albumin level. The increased risk of BM was associated with a lower BMI, plasma albumin levels, and higher height.
Conclusions:
A high prevalence of BM and TN was detected by ultrasonography screening in this cohort of Chinese women. These lesions occurred frequently and simultaneously, particularly in women with lesions in higher RADS categories.
Introduction
Both thyroid and breast diseases are more likely to occur in women (1,2), and their relationship has been widely explored. Prior research has shown an increased risk of developing either thyroid or breast cancer as a secondary malignancy after diagnosis of primary breast or thyroid cancer, respectively (3,4). However, some degree of ascertainment bias due to increased imaging surveillance of cancer survivors cannot be entirely excluded. Moreover, three prospective cohort studies have revealed that women with benign breast disease have an increased risk of subsequent thyroid cancer (5 –7), while another study revealed a negative result (8). Some studies have also found that women initially diagnosed with breast cancer have greater frequencies of thyroid disorders and nodules (9,10).
Among women without cancer, an association between breast and thyroid disorders has only been reported in a few studies with small sample sizes (11 –14). Furthermore, none have focused on the possible association between breast and thyroid lesions in screening studies of women from a general population without the possible influence and confounders associated with treatment or surveillance of either breast or thyroid carcinomas.
High-resolution ultrasound is an excellent modality for the evaluation of breast and thyroid lesions and is widely used in clinical practice in China wherein about 89% of breast cancer cases could be detected through ultrasonography (15). In the China Official Breast Cancer Screening Program, ultrasound was the primary diagnostic tool for 1.2 million women between 2009 and 2011, and only those with positive ultrasound findings were further investigated by mammography and biopsy (16). In health examination centers in China, asymptomatic women can usually choose to undergo breast and thyroid ultrasound evaluation at the same time. Therefore, the present cross-sectional ultrasound-based study evaluated the prevalence of breast masses (BM) and thyroid nodules (TN) and their association in an asymptomatic population of Chinese women.
Materials and Methods
Study design and participants
This cross-sectional study used data from the Quality Control Center of Health Examination in Chongqing (China), which is also the Health Management Center of the First Affiliated Hospital of Chongqing Medical University, on a general population of asymptomatic Chinese women. Consecutive female examinees who underwent comprehensive health examinations and synchronous breast and thyroid ultrasound scans from January 2015 to June 2017 were enrolled. Repeat examinations were recognized by their attached institution information and individual health examination ID, and only one examination data set was included.
Exclusion criteria were those younger than 18 years; history of treatment for breast or thyroid diseases; breast plastic surgery; pregnant or breast feeding; history of malignancy; history of hysterectomy or oophorectomy; history of radiation therapy for the head, neck, or chest region; and unavailable data (age, weight, height, and original descriptions and reports of thyroid and breast ultrasound). This study was approved by the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University and conducted in accordance with the principles of the Declaration of Helsinki. Requirement for informed consent was waived because all information was anonymous.
Procedures
Basic information, including sex and age, was checked before examination. Self-reported symptoms, disease histories, and postoperative imaging features or evidence from ultrasound or computed tomography (breast implants or resection of organs, etc.) were recorded. Blood pressure and anthropometric parameters (height, weight, and waist circumference) were measured by experienced medical staff following standard procedures. All blood samples were taken after at least 8 h of fasting and analyzed in the laboratory of the First Affiliated Hospital of Chongqing Medical University, which has been certified by the College of American Pathologists (CAP No.: 7215494).
Thyroid and breast ultrasound were performed using a 4.8–11 MHz linear probe (Aplio500; Toshiba Medical Systems), 5–14 MHz linear probe (Aplio500; Toshiba Medical Systems), or 3–12 MHz linear probe (HD11XE; Philips Medical Systems). All ultrasound examinations were performed and evaluated by experienced board-certified radiologists. For all subjects, ultrasound screening and the full diagnostic examination were completed simultaneously. All data collection was completed and registered in the electronic medical record system of the Quality Control Center of Health Examination in Chongqing. Data were extracted and processed by Microsoft Excel 2013 and SAS version 9.4.
Ultrasound assessment of breast and thyroid
For thyroid examination, subjects underwent ultrasound scanning in the supine position. Thyroid parenchyma (homogeneous or heterogeneous echo), gland size, and presence of TN were recorded in detail. A TN was defined as a defined lesion within the thyroid gland that is radiologically distinct from the surrounding parenchyma (17). Size, location, Doppler flow, and specific ultrasound features of the TN were described and documented. Ultrasound features of TN included comments on the composition (solid, cystic, mixed, or spongiform), echogenicity (hyper-, iso-, and hypoechogenicity), margins (well-circumscribed or irregular), calcifications (none, micro- or macrocalcifications), and taller-than-wide appearance (anteroposterior/transverse diameter ratio ≥1 or not). Herein, each TN was reviewed a second time and categorized according to Kwak's Thyroid Imaging Reporting and Data System (TI-RADS) standards (18).
For breast examination, all subjects underwent a whole breast ultrasound scan in the supine position. Descriptions of ultrasound findings were consistent with the Breast Imaging Reporting and Data System (BI-RADS) lexicon (2013) standards (19,20). A BM was defined as a three-dimensional lesion that occupies a space within the breast (19) and includes lesions such as breast cyst, mixed or solid masses, intraductal masses, and cystic duct dilation. Final assessment of malignancy risk for breast abnormities was given by board-certified ultrasound radiologists, and assessment was in conformity with the standard of the American College of Radiology BI-RADS (19,20).
Statistical analyses
Normality testing was performed for all continuous variables. Medians (interquartile range) and proportions were used to describe the data, and the Kruskal–Wallis testing was used to compare continuous variables by considering their nonnormal distribution. The chi-square test was used to compare categorical variables. Age-specific prevalence rates and 95% confidence intervals [CIs] of BM and TN were calculated.
Binary logistic regression was used to obtain odds ratios (OR) and CI for BM and TN. Basic multivariable models were adjusted for age, body mass index (BMI), and height, all of which are associated with BM and TN (21 –24). Metabolic and biochemical markers were not included in the binary logistic models directly, and additional screening models were used to select covariates, in which both statistic and medical significance were taken into account (Supplementary Appendix Tables SA1 and SA2) (25). In multivariable-adjusted models, age was categorized into groups according to their univariate logit transformation values, and other factors, including BMI, height, plasma albumin, and systolic blood pressure, were analyzed as continuous variables. A multicollinearity test was performed (by calculating the proportion of variations and variance inflation factors) for models, and no statistical collinearity was found.
Furthermore, multinomial logistic regression was used to explore the correlation between TN and BM with different RADS categories. The variables selected by additional screening model and put into binary logistic regression analysis were included in the generalized logit models for the multinomial logistic analysis. Data points were missing for blood pressure (182; 0.5%) and plasma albumin (876; 2.6%), and sample sizes were reduced for analysis when the two variables were included. A two-tailed p < 0.05 was considered significant. All statistical analyses were performed with SAS version 9.4 or SPSS 22.
Results
Of the 34,184 eligible adult females enrolled in this study, 6371 (18.6%) had BM, 12,153 (35.6%) had TN, and 2279 (6.7%) had both. Anthropometric and biochemical characteristics of participants are shown in Table 1. Age-specific prevalence of BM and TN is shown in Figure 1. BM prevalence increased slightly with age and was highest in women aged 45–49 years, with a peak prevalence of 27.4% [CI 26.1–28.7], then decreased and stabilized at a rate of 5.4–7.4% after 60 years of age (Fig. 1). With regard to TN, prevalence increased with age, except in women younger than 25 years, and rose to 77.4% [CI 73.0–81.9] for those aged 80 years and older (Fig. 1).
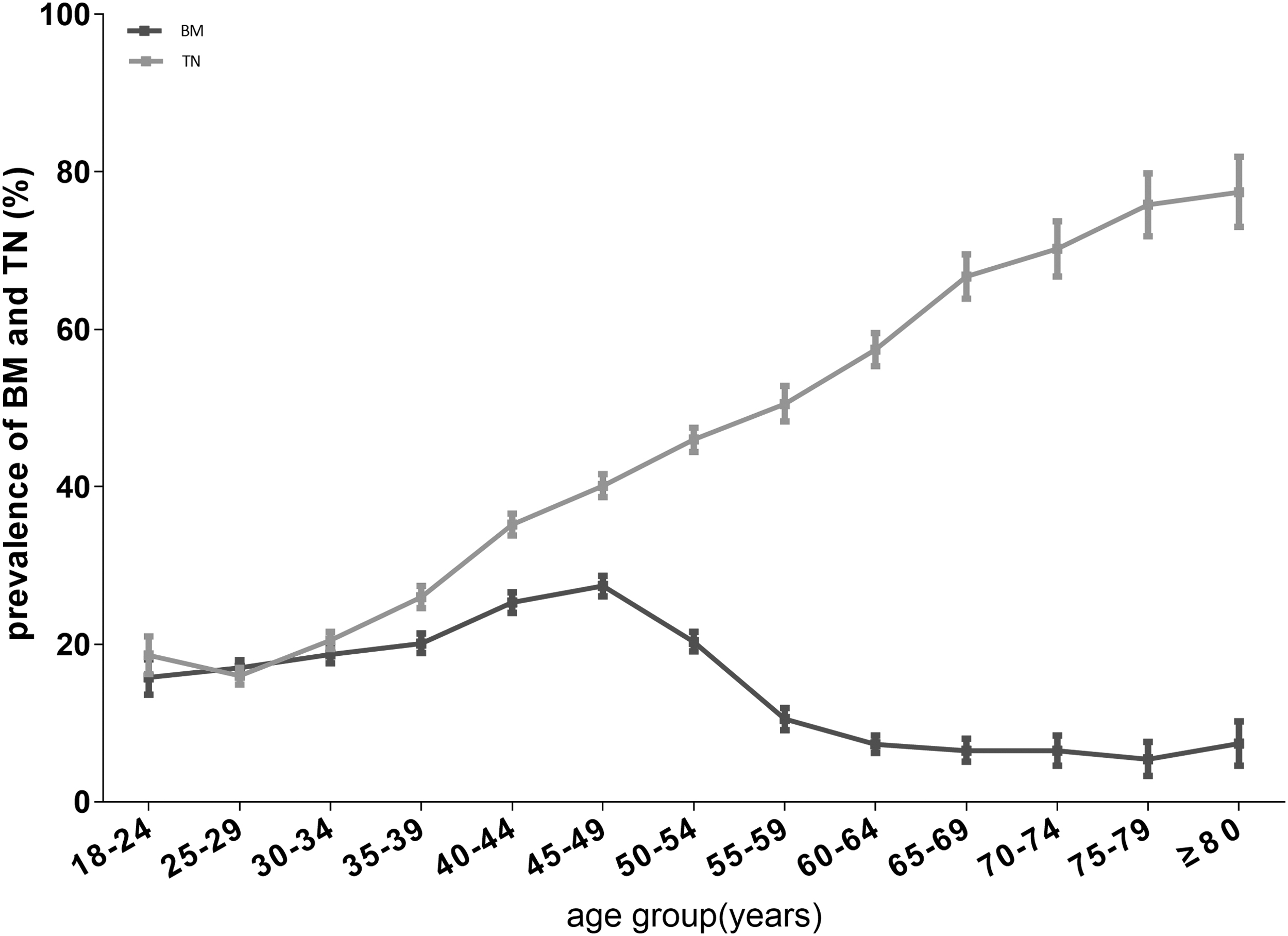
Age-specific prevalence and CI of BM and TN in Chinese women. BM, breast mass(es); TN, thyroid nodule(s); CI, 95% confidence interval.
Anthropometric and Biochemical Characteristics of Subjects with Different Breast Masses and Thyroid Nodules Status by Ultrasonography
p-Values were derived from the Kruskal–Wallis or χ 2 tests.
Cutoff values of these components are consistent with the metabolic syndrome criteria by Joint Statement.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BM, breast mass(es); BUN, blood urea nitrogen; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TN, thyroid nodule(s).
Among subjects with TN, 2087 (17.2%) had nodule(s) larger than 10 mm. All ultrasound BI-/TI-RADS categories for breast and thyroid are summarized in Table 2. The age-specific prevalence of BM and TN with different categories is summarized in Supplementary Appendix Figures SA1 and SA2. After adjusting for age, BMI, and height, women with TN had a 1.151-fold increased risk ([CI 1.081–1.225], p < 0.0001) of having synchronous BM compared with those with normal thyroid ultrasound scans (Table 3). Moreover, women with TN larger than 10 mm (OR = 1.249 [CI 1.104–1.413], p = 0.0004) and equal to 10 mm or less (OR = 1.134 [CI 1.062–1.211], p = 0.0002) were at higher risk of BM compared with those with normal thyroid structure. Similarly, participants with BM had 1.165 times higher risk ([CI 1.096–1.238], p < 0.001) of having synchronous TN compared with those without BM (Table 4). There was no significant interaction between age and BM or TN, indicating that their association is independent of age.
Ultrasound Breast and Thyroid Imaging Reporting and Data System Categories of Breast and Thyroid
BM were revealed in 18.6% (6371) of all subjects and assigned to BI-RADS categories 2–5.
TN were found in 35.6% (12,153) of all subjects and recategorized into TI-RADS 3–5.
Five cases with BI-RADS category 0 lesions were assigned to BI-RADS category 4A for their similar degree of abnormality hierarchy.
BI-RADS, Breast Imaging Reporting and Data System; TI-RADS, Thyroid Imaging Reporting and Data System.
Multivariable-Adjusted Odds Ratios for Breast Masses
Basic multivariable models 1 and 2 were adjusted for age (≤24, 25–29, 30–34, 35–37, 38–40, 41–43, 44–46, 47–49, 50–52, 53–55, 56–58, 59–61, 62–64, 65–69, 70–74, 75–79, and ≥80 years), BMI, and height.
The additional multivariable model was adjusted for age, BMI, height, thyroid status (normal, diffused heterogeneous echo, TNs), and plasma albumin level.
BMI, body mass index; CI, 95% confidence interval.
Multivariable-Adjusted Odds Ratios for Thyroid Nodules
The basic multivariable model was adjusted for age (≤24, 25–29, 30–34, 35–37, 38–40, 41–43, 44–46, 47–49, 50–52, 53–55, 56–58, 59–61, 62–64, 65–69, 70–74, 75–79, and ≥80 years), BMI, and height.
The additional multivariable model was adjusted for age, BMI, height, breast status (BMs or non-BMs), SBP, and plasma albumin.
Multinomial logistic regression analysis showed that the association between BM and TN increases with increasing RADS malignancy risk (Tables 5 and 6). The strongest adjusted correlation was noted in BI-RADS category ≥4A BM with TI-RADS category ≥4C TN (BI-RADS ≥4A: OR = 1.904 [CI 1.485–2.440], p < 0.0001; TI-RADS ≥4C: OR = 1.915 [CI 1.494–2.455], p < 0.0001).
Multivariable-Adjusted Odds Ratios [95% Confidence Interval] for Breast Lesions with Different Breast Imaging Reporting and Data System Categories
Model was adjusted for age (≤24, 25–29, 30–34, 35–37, 38–40, 41–43, 44–46, 47–49, 50–52, 53–55, 56–58, 59–61, 62–64, 65–69, 70–74, 75–79, and ≥80 years), BMI, height, and plasma albumin.
p < 0.05.
p < 0.001.
Multivariable-Adjusted Odds Ratios [95% Confidence Interval] for Thyroid Nodules with Different Thyroid Imaging Reporting and Data System Categories
Model was adjusted for age (≤24, 25–29, 30–34, 35–37, 38–40, 41–43, 44–46, 47–49, 50–52, 53–55, 56–58, 59–61, 62–64, 65–69, 70–74, 75–79, and ≥80 years), BMI, height, plasma albumin, and SBP.
p < 0.05.
p < 0.001.
In addition, because some studies have reported potential relationships between metabolic status and thyroid or breast neoplasms (22,26 –28), other risk factors for BM and TN were explored. A higher BMI was found to be associated with a decreased risk of BM and increased risk of TN, and taller women had an increased risk for both BM and TN (Figs. 2 and 3). There was no significant difference between the proportion of subjects with a maximal BM of 10 mm or less out of all subjects with BM in different BMI groups (Supplementary Appendix Table SA3). Moreover, additional multivariable-adjusted models also revealed inverse correlations between plasma albumin level (per 5 g/L increase) with prevalence of BM (OR = 0.874 [CI 0.827–0.924], p < 0.0001) and TN (OR = 0.924 [CI 0.881–0.969], p = 0.0011) (Tables 3 and 4). With an adjusted OR of 1.128 ([CI 1.060–1.200], p = 0.0001), elevated blood pressure levels (systolic ≥130 or diastolic ≥85) were also associated with a higher risk of TN.

Relationship between BMI and prevalence of BM and TN (adjusted for age, height, and TN/BM). BMI, body mass index.
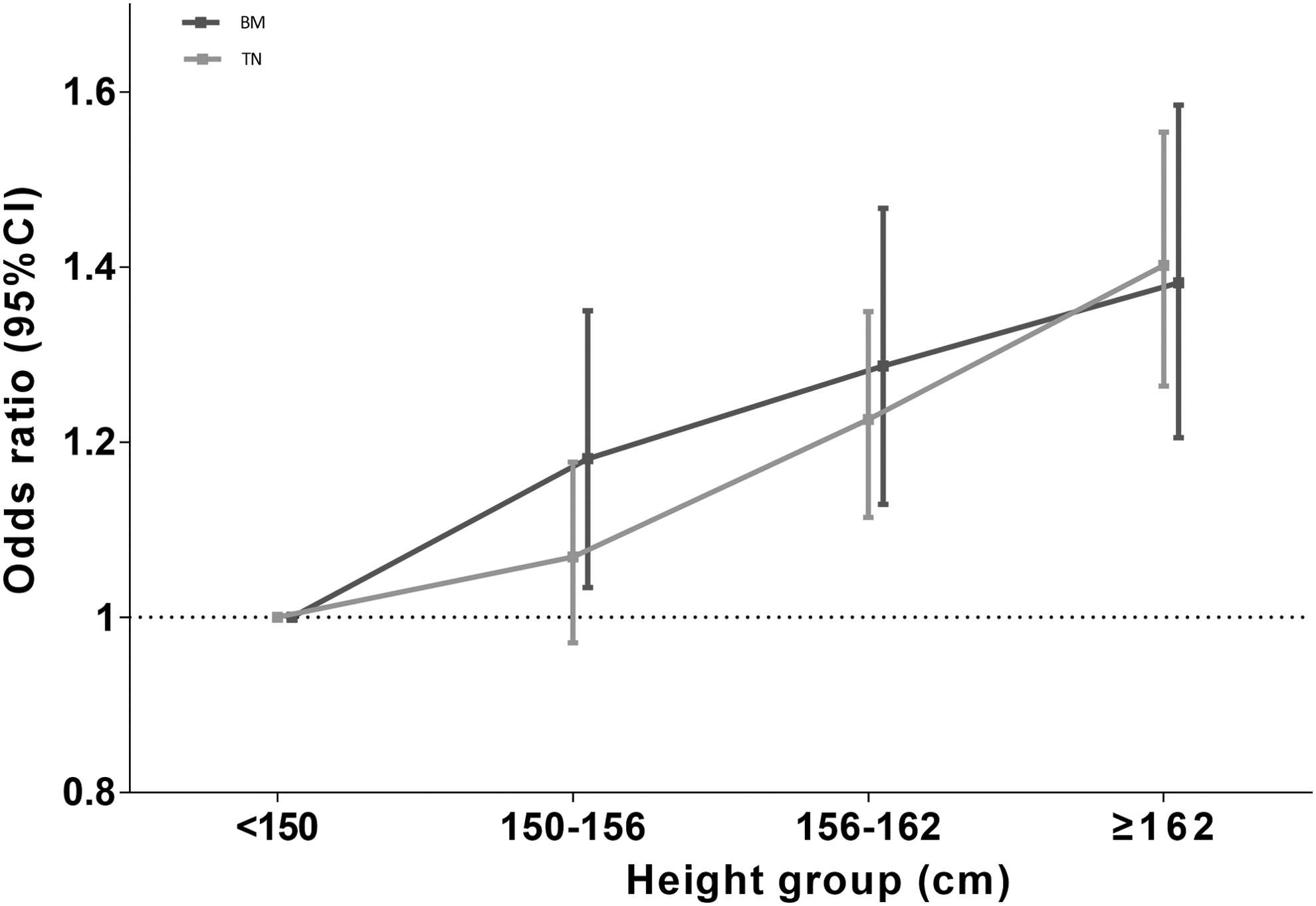
Relationship between height and prevalence of BM and TN (adjusted for age, BMI, and TN/BM).
Discussion
In the present study, the prevalence of BM and TN and their association in a population-based cohort of asymptomatic Chinese women who underwent simultaneous ultrasound screening for breast and thyroid lesions were determined. A high frequency of BM and TN was detected, as well as a tendency for these lesions to simultaneously occur. To the best of our knowledge, this is the first study focusing on the relationship between breast and thyroid lesions in a screening series. Because there was no influence through detection bias, which can be present in individuals who undergo surveillance examinations because of preexisting breast or thyroid disease (4,29), the results of the present study are believed to be reliable and better reflect the intrinsic relationship between breast and thyroid lesions.
Here, the peak age for BM prevalence was between 45 and 49 years old (Fig. 1), which coincides with the age peak of breast cancer in China reported previously (30). Moreover, 882 (2.6%) had BM with lesions in BI-RADS category ≥4A that need further diagnostic biopsy, accounting for 13.8% of the total subjects with BM, and 7424 (21.7%) had TN in TI-RADS category ≥4A, accounting for 61.1% of the total subjects with TN. Women with BM in BI-RADS category ≥4A also had about a twofold risk for occurrence of TN with a TI-RADS category ≥4C. A BM assigned to a BI-RADS category ≥4A has a malignancy risk of >2%, and tissue biopsy is recommended (19). A TN assigned to a TI-RADS category ≥4C has a malignancy risk of >44% (18), but this value may be an overestimate because the majority of TN herein were 1 cm or less in diameter.
The association between BM and TN found here suggests that there is relationship between breast and thyroid neoplasms (both benign and malignant), and this association is presumably caused by shared risk factors, such as hormonal risk factors and genetic susceptibility. (4). A previous case–control study showed that breast cancer patients with coexisting thyroid cancer have higher expression of estrogen and progesterone receptors compared with those with breast cancer alone (29). Additionally, estrogen receptors can be expressed in thyroid tissues, and expression in TN has been shown to be significantly higher than that in normal thyroid tissues (31). Estrogen has also been considered to play a role in stimulating growth and decreasing the differentiation of TN-derived stem and/or progenitor cells (32), which may lead to an increased co-occurrence rate of TN and BM.
In another malignant series, a large study in China of 13,978 breast cancer patients observed a much higher incidence (1.8%) of thyroid cancer (33), of which 30% had synchronous carcinomas (interval time for diagnosis of both cancers, <1 year), and it was associated with inferior recurrence-free survival of breast cancer. These findings emphasize the clinical significance of evaluating women presenting with breast or thyroid cancer for abnormal findings in the two organs.
The current study also revealed potential risk factors for BM and TN. Higher height was associated with an increased risk of BM, and a similar association between height and breast cancer has been reported (34 –36). In addition, women with a higher BMI had a lower risk of BM. Although it is well known that in postmenopausal women obesity is significantly associated with increased risk of breast cancer (37), the opposite association has been found in premenopausal women (38,39). Another study of premenopausal women aged 18–54 years revealed that an inverse association between obesity and breast cancer risk is stronger in early adulthood (40). It should be noted that the reduced premenopausal breast cancer risk with obesity has not been observed in all studies; some disparities in subtypes of breast cancer and ethnicities need to be further explored (37,41,42).
The current study did not find an interaction effect between BMI and age on BM. Although subanalysis of menopausal status was not conducted herein, 81% of subjects were younger than 55 years, the cutoff year of menopause in a previous study (40). To rule out the possibility of decreased sensitivity in detecting smaller BM among women with a higher BMI, the proportion of subjects with a maximal BM of 10 mm or less out of all subjects with BM in different BMI groups was calculated and no difference across BMI stratifications was found (Supplementary Appendix Table SA3). Therefore, the present results suggest that increased adiposity is more likely to be a protective factor for BM.
Underlying biological mechanisms may involve the relationship between obesity and hormone levels (43), such as increased estrogen in adolescence, decreased sex hormone binding globulin (23) and insulin-like growth factor 1 (44) in premenopausal women, and decreased thyroid function (45,46). Exploring such mechanisms might have preventive value for breast lesions. With regard to risk factors for TN, a positive correlation between age, BMI, height, and frequency of TN was found herein. This result was consistent with previous studies in Asian populations (21,22). TN and cancer share some common risk factors, including ionizing radiation, iodine deficiency, and anthropometric factors (47).
It is well established that breast cancer screening for women aged 40 years and older could decrease mortality and improve survival outcomes (30,48). Based on current guidelines for breast cancer screening (48), screening should be recommended for women with either benign or malignant TN. As for thyroid cancer screening, it remains unclear whether screening of the general population or specific subsets would decrease thyroid cancer mortality because it is typically low (49). A nationwide retrospective cohort study in Korea evaluated the long-term survival (average, 9.4 years) outcomes of thyroid cancer patients with different detection methods and found that patients with advanced thyroid cancer detected by ultrasound screening had lower all-cause and thyroid cancer-specific mortality compared with those detected based on clinical symptoms (50). This suggests that screening for thyroid cancer may be necessary in some patients, but this requires further study and cost–benefit analyses (51).
The current study does have some limitations. First, most of the study population was from an urban area in a single center. Therefore, the prevalence of TN and BM predominately reflected the status in urban populations of southwest China. Second, data from physical examinations did not provide the menopausal status of subjects. Thus, BM-TN correlations could not be exactly distinguished before and after menopause.
In summary, the results of the current study revealed a high prevalence of BM and TN as detected by ultrasonography screening in asymptomatic women. Simultaneous occurrence of these lesions was frequent, particularly in women with higher RADS category lesions. An increased prevalence of TN was associated with a higher BMI, height, systolic blood pressure, and lower plasma albumin level, while increased BM prevalence was associated with a lower BMI, plasma albumin level, and higher height. Understanding these correlations and potential underlying mechanisms will provide more clues for BM and TN screening and may also have preventive value.
Footnotes
Authors' Contributions
H.L., Z.W., J.-S.L., L.R., and L.-Q.K. designed and conducted the study. All authors collected data. H.L., Z.W., J.-S.L., H.-R.C., Z.X., and B.-S.Z. analyzed the data. H.L., Z.W., J.-S.L., H.-R.C., Z.X., B.-S.Z., L.R., and L.-Q.K. interpreted the data. H.L., Z.W., and J.-S.L. drafted the article. Content and language revisions were provided by H.L., S.T., Y.-L.S., K.-N.W., L.R., and L.-Q.K. All authors have provided final approval for the revised submitted article and agreed to be accountable for all aspects of the work.
Acknowledgments
We thank Dr. Li-ping Liu and Dr. Bo Tu (Department of Ultrasonography, The First Affiliated Hospital of Chongqing Medical University) for their help in data recognition and classification regarding breast and thyroid ultrasound reports.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported through provision of data by the Quality Control Center of Health Examination in Chongqing, Chongqing Medical University, China.
Supplementary Material
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
Supplementary Appendix Table SA3
Supplementary Appendix Figure SA1
Supplementary Appendix Figure SA2