
Abstract

A
We report here an update, four years later, with the first description of secondary resistance to crizotinib and subsequent therapeutic efficacy of other ALK inhibitors in a patient with an ALK-rearranged ATC.
We previously reported the case of a 75-year-old woman with advanced ALK-rearranged ATC showing near complete response under treatment with crizotinib. This response lasted 36 months until the patient presented new thoracic tumor progression. A new biopsy was performed to identify genetic mechanisms involved in secondary progression. Histological assessment was consistent with the diagnosis of ATC. Immunohistochemistry showed strong and intense staining with an ALK antibody (Clone D5F3). Fluorescence in situ hybridization confirmed the presence of an ALK rearrangement without a copy number variation. Next generation sequencing (Ion AmpliSeq™ Comprehensive Cancer Panel) identified the previously described STRN-ALK fusion gene. No other genetic alteration and in particular no secondary ALK mutation was identified.
Considering the absence of alternative bypass pathway activation, the patient was offered to start off-label treatment with ceritinib, a second-generation ALK inhibitor shown to be able to overcome crizotinib resistance in ALK-rearranged nonsmall cell lung cancer. Tolerance was good. First tumor assessment after 4 weeks of treatment showed significant tumor regression (−28% according to RECIST). After 8 weeks of treatment, a new CT scan showed an almost complete response (Fig. 1) that is still ongoing 16 months after treatment onset. Then, brigatinib was started for a cerebral progression that led to a rapid partial response (−41% to RECIST 1.1). Eight months later, the patient died of her radiation-induced locally advanced squamous esophageal cancer (proved by a different morphological histology).
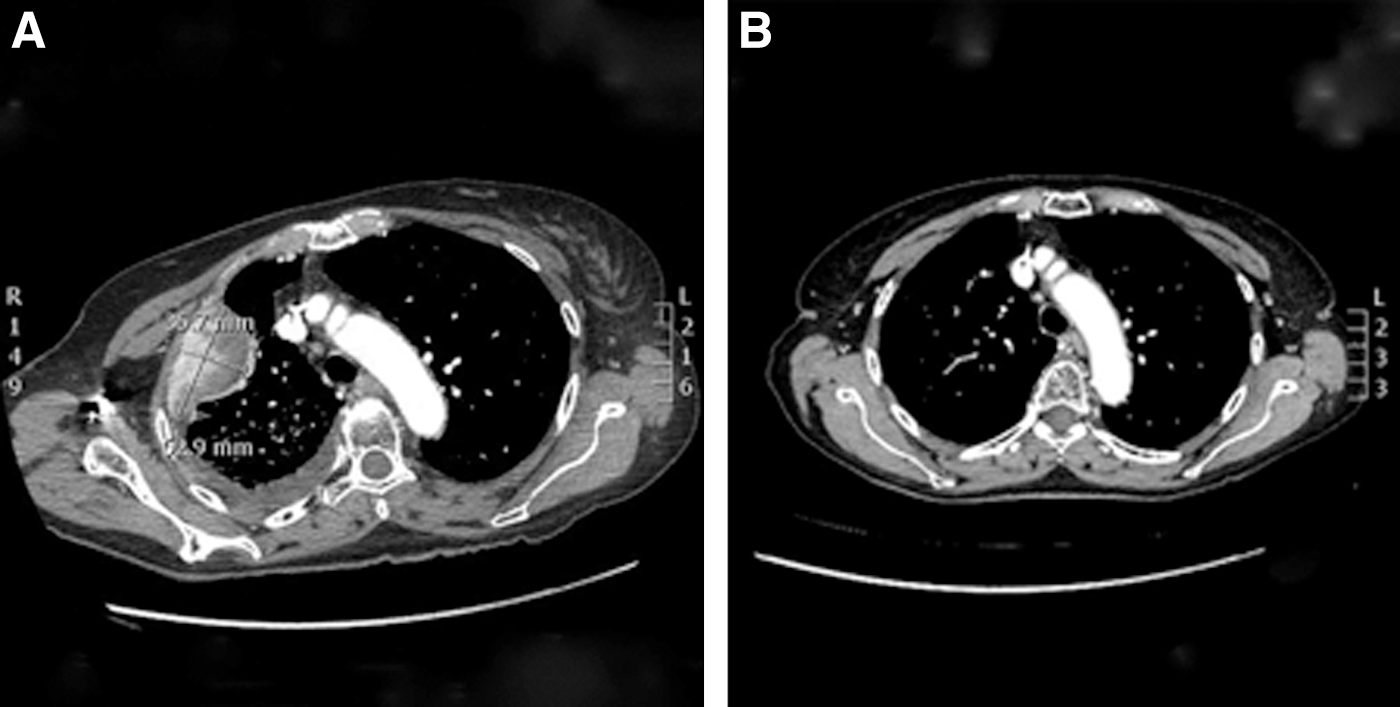
Computed tomography scans before (
In our case, no alteration, particularly in the 28 coding exons of the ALK gene (covered by the sequencing panel), can explain the resistance to crizotinib and the sensitivity to ceritinib and brigatinib sensitivity. The ALK inhibitor effect is probably sufficient to explain the decrease in tumor relapse. Indeed, in a phase 1 trial, 19 patients who were crizotinib resistant and were switched to ceritinib showed a tumor regression. Among them, only seven had an ALK-dependent resistance (5).
In conclusion, this case illustrates a response to ceritinib in a crizotinib-refractory ALK-rearranged ATC, and a subsequent response to brigatinib in a ceritinib-refractory ALK-rearranged ATC. Genomic and molecular testing of tumors has become increasingly useful for treatment through the identification of potential targets for novel therapies irrespective of histology. Identification of ALK fusions is of clinical importance and must be included in the work-up all patients with ATC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.