
Abstract
Background:
Radioactive iodine (131I) is in widespread use for the treatment of hyperthyroidism. Data on long-term safety outcome are limited and conflicting. The objectives of this study were to evaluate the association of radioiodine treatment for hyperthyroidism with overall cancer and with specific cancer types.
Methods:
This is a historical cohort study, using the Clalit health care database. Participants were all adults with a new diagnosis of hyperthyroidism in 2002–2015, newly treated with 131I, or with thionamides (propylthiouracil/thiamazole), excluding patients with previous malignancies. Age, sex, smoking history, body mass index, Clalit district, socioeconomic status, history of diabetes mellitus and of hypertension, use of aspirin and of statins, and adherence to cancer screening procedures were used to calculate propensity score to receive radioiodine. Incidence rates and 95% confidence intervals (CIs) were calculated for overall cancer occurrence, and for each cancer type using Poisson distribution. Association between study variables and time to cancer event was evaluated using cause-specific hazard ratios (HR) and CIs, estimated by univariate and propensity score adjusted multivariate Cox proportional hazards models. For sensitivity analysis we stratified the cohort by calendar year at cohort entry and by length of follow-up.
Results:
A total of 16,637 patients formed the study cohort, with 123,166 person-years of follow-up. There was no association between radioiodine treatment and increased risk of overall cancer (HR = 0.99 [CI 0.83–1.19], p = 0.91; HR = 1.01 [CI 0.83–1.21], p = 0.95) in univariate and multivariate analyses, respectively. However, in a sensitivity analysis, we found an association with overall cancer risk in the first period of follow-up (up to 4.2 years) (HR = 2.11 [CI 1.59–2.80], p < 0.0001), and no association with increased risk in a longer follow-up period. An association was found between radioiodine exposure and an increased risk for non-Hodgkin's lymphoma (NHL) in univariate but a nonsignificant increased risk in multivariate analysis: HR = 2.89 [CI 1.12–7.46], p = 0.03; HR = 2.32 [CI 0.88–6.13], p = 0.09, respectively.
Conclusions:
No association was found between radioiodine treatment for hyperthyroidism and risk for incident cancer in long-term follow-up. In an analysis of specific cancer types, a statistically significant association was found with NHL only in univariate analysis.
Introduction
Radioactive iodine (131I) is in widespread use for the treatment of hyperthyroidism resulting from Graves' disease, toxic adenoma, and multinodular goiter, and for the treatment of thyroid cancer (1 –3). The radioiodine is incorporated into the thyroid gland after oral administration, and its beta emission damages the thyroid tissue and function (1). Other measures for decreasing thyroid hormone synthesis in hyperthyroidism are drug treatment with thionamides and, less frequently, (sub)total thyroidectomy (1).
The American Thyroid Association guidelines for the management of Graves' hyperthyroidism recommend a 131I dose sufficient to cause hypothyroidism, typically 10–15 mCi (370–555 MBq) (4). Slightly higher radioiodine doses are usually needed for the treatment of toxic adenomas and multinodular goiters, but the activities are usually lower than the ones used for remnant ablation or as an adjuvant therapy in thyroid cancer (100–200 mCi) (5).
Concern has been raised as to the possible carcinogenic effects of 131I, heightened by reports of increased incidence of cancers after exposure to the fallout from the Chernobyl nuclear accident, where the main contaminating isotope was 131I (6), and an increased risk of leukemia and a suggestion of a radiation dose–response risk for non-Hodgkin's lymphoma (NHL) in survivors of the Hiroshima and Nagasaki atomic bombings (7).
In thyroid cancer patients treated with radioiodine, an increasing cumulative activity of administered 131I is associated with an increased risk of solid cancers and leukemia (8). In Taiwan, the highest significant standardized incidence ratio (SIR) for secondary primary malignancy in thyroid cancer patients was found for leukemia, followed by NHL and solid cancers (9). In a retrospective analysis of thyroid cancer patients in Korea that aimed to investigate the association between radioiodine treatment and leukemia, a 131I activity exceeding 100 mCi was associated with the risk for developing leukemia, while lower radioiodine doses were not (10).
However, when studying thyroid cancer patients treated with radioiodine, the increased incidence of secondary primary malignancy could also be related to increased medical surveillance, contributing to an earlier detection of cancers with a long latency, and also to common etiological factors to the two malignancies, such as hereditary factors, as well as to misclassified metastases. In contrast, hyperthyroid patients with no history of malignancy can be evaluated for the effect of radioiodine treatment, with less the potential biases mentioned earlier. Moreover, hyperthyroid patients have alternative treatment options besides radioiodine, and it is of paramount importance to identify cancer risk associated with the treatment.
Data on long-term outcomes of patients treated with 131I for hyperthyroidism are limited and conflicting. Only few studies were published and most of the studies included reports on SIRs only, and did not include a control hyperthyroid group. An increased risk for specific cancer types, such as cancers of the stomach, kidney (11), and breast (12), has been observed. Other studies reported an increase in thyroid cancer occurrence only (13) and a decrease in overall cancer incidence (14).
We performed a cohort study within a population-based clinical database in Israel, with the aim to study possible associations with overall cancer risk, as well as the risk for specific cancer types after radioiodine treatment for hyperthyroidism.
Methods
Clalit Health Services is the largest health services provider in Israel providing medical care to more than half of the Israeli population. All clinical and administrative data of Clalit are centrally computerized to produce a patient electronic record that includes all diagnoses (coded using the International Statistical Classification of Diseases, 9th Revision [ICD-9]), lifestyle variables such as body mass index (BMI), and smoking, as well as full hospitalization records, radiology, laboratory, and pharmacy data. This database has been formerly described and is valid and reliable (15,16).
Using the Clalit database, we carried out a historical cohort study of all patients, ≥18 years, with a new diagnosis of hyperthyroidism (thyrotoxicosis, thyroid nodular goiter, or benign neoplasm of thyroid: ICD-codes: 226, 241, 242), between January 1, 2002 and June 30, 2015 who were treated with any thionamide drug (propylthiouracil or thiamazole) or with 131I. Date of entry to the cohort was the date of first prescription of a thionamide or radioiodine. If a patient was treated with thionamide and later with radioiodine, time of follow-up starting at beginning of thionamides and before receiving radioiodine was added to the follow-up time of thionamide treatment to prevent immortal time bias (17). Thus, for this patient, follow-up time for radioiodine was started at the date of administration of radioiodine.
To assure reliable data on past medical history, study patients were required to have at least 6 months of medical history in Clalit before entry into the cohort. We excluded all patients with any previous malignancy, myelodysplastic syndrome, myeloproliferative diseases, or a history of organ/blood marrow transplantation (ICD-9 codes: 140–172, 174–209, 199.2, 238.4, 238.71–238.77, 284, 285.0, 289.83, 996.8, V42) at cohort entry date.
Cancer diagnoses were retrieved from the Clalit database, and from the Israeli Ministry of Health National Cancer Registry. Data on mortality were gathered from Clalit. Follow-up was until a first diagnosis of cancer, or June 30, 2016, or death, or end of registration in Clalit, whichever came first. To account for latency time period, the time at risk of developing cancer was defined from 1 year after cohort entry, to the end of follow-up. End points were a new diagnosis of any cancer (ICD-9 codes: 140–172, 174–209, 199.2, 238.4, 238.71–238.77, 284, 285.0, 289.83) and specific cancer types, appearing at least 1 year after cohort entry date.
To account for possible confounders we retrieved data on demographic and clinical parameters at cohort entry date: age, sex, smoking history, BMI, Clalit district, socioeconomic status, history of diabetes mellitus, history of hypertension, and pharmacy administration of at least three prescriptions of aspirin and of statins at the year before cohort entry date. To account for possible detection bias, we retrieved data on adherence to cancer screening procedures recommended in Israel: mammography every 2 years for women ≥50 years in the past 6 years before inclusion in the study cohort; and annual fecal occult blood test (FOBT) for men and women ≥50 years in the past 5 years before inclusion in the study cohort. Missing data on smoking and BMI were treated as a separate “missing” category.
Incidence rates and 95% confidence intervals (CIs) were calculated for each cancer types and for overall cancers, using Poisson distribution. We calculated the inverse probability of treatment weighting using the propensity score to receive radioiodine, which included all demographic and clinical parameters (age, sex, smoking history, BMI, Clalit district, socioeconomic status, diabetes mellitus, hypertension, pharmacy administration of aspirin and of statins, and adherence to mammography and to FOBT) to estimate exposure effects adjusted for measured confounding.
Association between study variables and time to a first cancer event, and to mortality, was evaluated with the use of cause-specific hazard ratios (HRs) and CIs, estimated by the univariate and multivariate Cox proportional hazards models with adjusted standard errors to account for correlations induced by clustering the use of thionamides and then radioiodine in some patients (SAS PHREG procedure, sandwich formula).
For sensitivity analysis we stratified the cohort by calendar year at cohort entry to account for difference, if it existed, in radioiodine dose over the years. We also stratified the cohort by length of follow-up to ascertain for associations of cancer risk with time since radioiodine administration. Statistical Analysis Software, version 9.4 (SAS Institute, Cary, NC) was used. All analyses were two-tailed, p < 0.05 was considered significant. Patients and the public were not involved in the design, conduct, and reporting of the research.
Results
Study patients
Among all Clalit insurees between January 1, 2002 and June 30, 2015, 19,765 were newly diagnosed with hyperthyroidism and newly treated with radioiodine and/or with an oral thionamide. Of them, 353 were <18 years; 1141 patients were excluded because of a previous history of cancer/myeloproliferative/myelodysplastic disease; 24 patients were excluded because of a previous history of organ/tissue transplantation; and 1610 patients did not have a minimum of 1 year of follow-up from the date of cohort entry, and were also excluded from analysis. A total of 16,637 patients formed the study cohort for analysis of cancer occurrence, with 123,166 person-years (PYs) of follow-up.
The mean follow-up time was 7.27 (standard deviation [SD]: 3.81) years, range: 1–15 years. There were 2829 patients treated with radioiodine. Of them, 1808 were treated with thionamides followed by radioiodine. Their follow-up time for radioiodine was started at the date of administration of radioiodine to a total of 21,460 PYs of follow-up after radioiodine treatment. A total of 13,808 patients were treated with thionamides only, and 1808 patients were treated with thionamides before receiving radioiodine, to a total of 101,706 PYs of follow-up of after thionamide treatment.
Baseline characteristics of the study cohort, and the ICD-9 diagnosis of thyrotoxicosis, thyroid nodular goiter, or benign neoplasm of thyroid, which the patient received at cohort entry, are shown in Table 1. The mean age of the cohort was 51.9 (SD: 18.1, median: 51, range: 18–101); 74% were women. A total of 2695 patients (95.3%) treated with radioiodine were administered a single radioiodine treatment, 131 (4.6%) received two radioiodine treatments, 2 patients received three treatments of radioiodine, and 1 patient (0.006%) received four radioiodine treatments.
Baseline Characteristics of the Study Cohort
Categorical variables are presented as numbers and percentages and continuous variables as mean ± SD.
ICD-9, International Statistical Classification of Diseases, 9th Revision; SD, standard deviation.
Radioiodine treatment and cancer
A total of 825 patients were diagnosed with incident cancer during 123,166 PYs of follow-up, yielding an overall incident cancer rate of 6.70 [CI 6.26–7.17] per 1000 PYs of follow-up. In Cox regression analyses, no significant association was found between radioiodine and increased risk of overall cancer (HR = 0.99 [CI 0.83–1.19], p = 0.91; HR = 1.01 [CI 0.83–1.21], p = 0.95) in univariate, and in a multivariate analysis controlling for the propensity score to receive radioiodine, respectively.
All first incident cancer types and analyses of the association between radioiodine treatment and each cancer diagnosis are presented in Table 2; time to each cancer diagnosis is listed in Supplementary Table S1. We found a higher occurrence of NHL in the radioiodine-exposed patients, with 7 cases among 2829 radioiodine-exposed, and 11 cases per 13,808 nonradioiodine-exposed patients (HR = 2.89 [CI 1.12–7.46], p = 0.03; HR = 2.32 [CI 0.88–6.13], p = 0.09) in univariate and multivariate analyses, respectively. The absolute risk increase was 2.18 per 1000 PYs [CI −0.38 to 4.68] (Table 2; Fig. 1A, B).
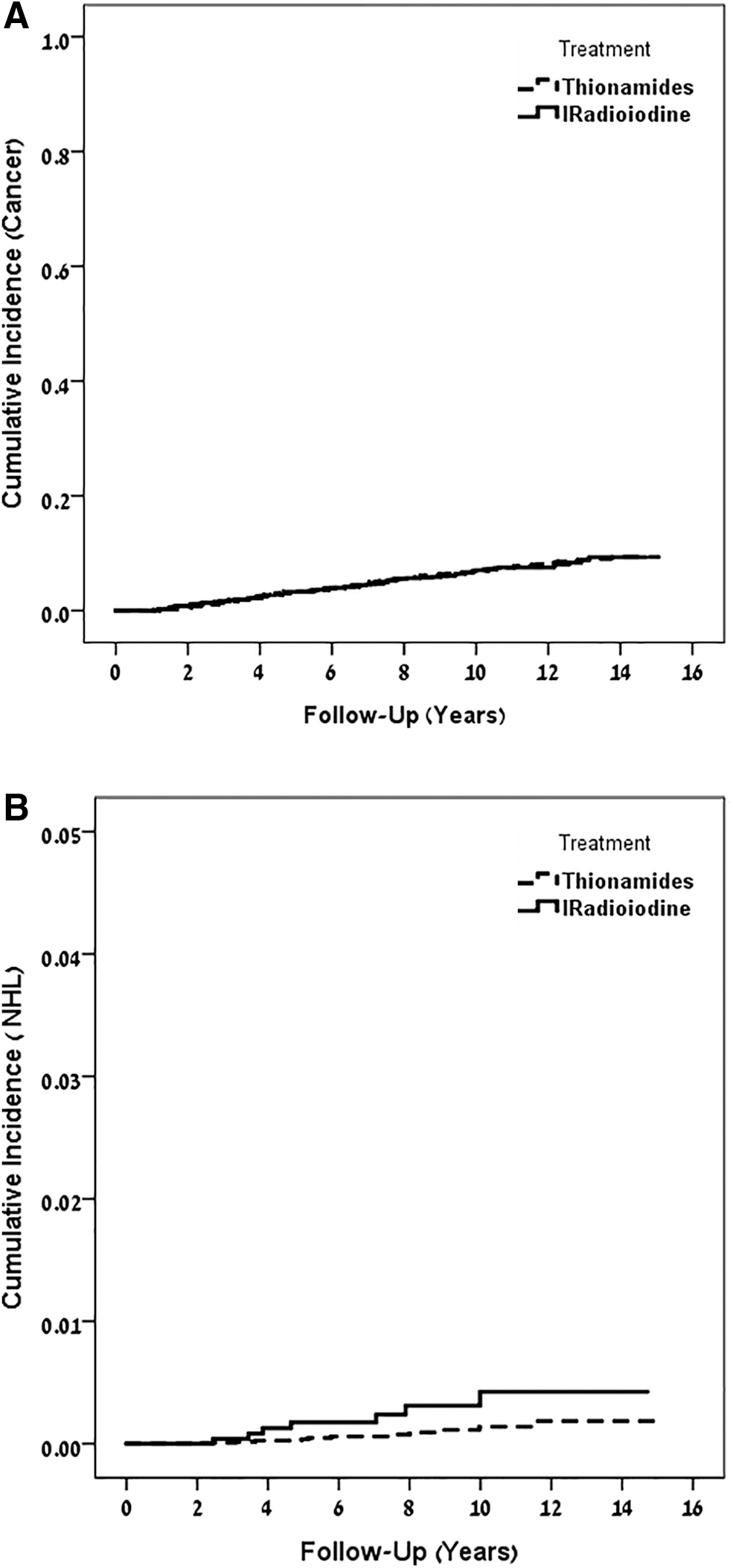
Kaplan–Meier curves showing cumulative cancer incidence in patients with hyperthyroidism that began treatment with thionamides or with radioiodine. (
Univariate and Multivariate Analyses of the Association Between Radioiodine Treatment for Hyperthyroidism and New Cancer Diagnoses
CI, confidence interval; CNS, central nervous system; CRC, colorectal cancer; HR, hazard ratio; NHL, non-Hodgkin's lymphoma; PYs, person-years.
Of the 7 NHL cases diagnosed in the radioiodine group, 2 suffered follicular NHL in the neck/chest, 8 and 4 years, respectively, after radioiodine exposure; 4 were diagnosed with large B cell lymphoma in the abdominal cavity/or diffuse NHL 3, 3, 5, and 7 years, respectively, after exposure; and 1 patient was diagnosed with Sezary syndrome 10 years after radioiodine treatment.
We have found a borderline association with a decreased risk of thyroid cancer in the radioiodine-treated patients (HR = 0.50 [CI 0.23–1.09], p = 0.08; HR = 0.45 [CI 0.21–0.99], p = 0.048) in univariate and multivariate analyses, respectively. Overall, treatment with thionamides was associated with a higher mortality rate than treatment with radioiodine, with a HR = 1.31 [CI 1.15–1.51], p < 0.001; HR = 1.21 [CI 1.05–1.39], p = 0.009, in the univariate and multivariate Cox proportional hazards models, respectively.
There was no difference in risk associated with radioiodine exposure in different calendar years, in a sensitivity analysis in which we stratified the cohort by year of cohort entry.
In a second sensitivity analysis we stratified the cohort to three tertiles by length of follow-up. Risk for any cancer, associated with radioiodine exposure, increased in the first period of follow-up (up to 4.2 years) (HR = 2.11 [CI 1.59–2.80], p < 0.0001), and no association with increased risk was evident in patients followed for 4.2–8.9 years (HR = 0.94 [CI 0.69–1.26], p = 0.67), and in follow-up of >8.9 years (HR = 0.94 [CI 0.58–1.53], p = 0.80) in multivariate analyses (Fig. 2 A–C).
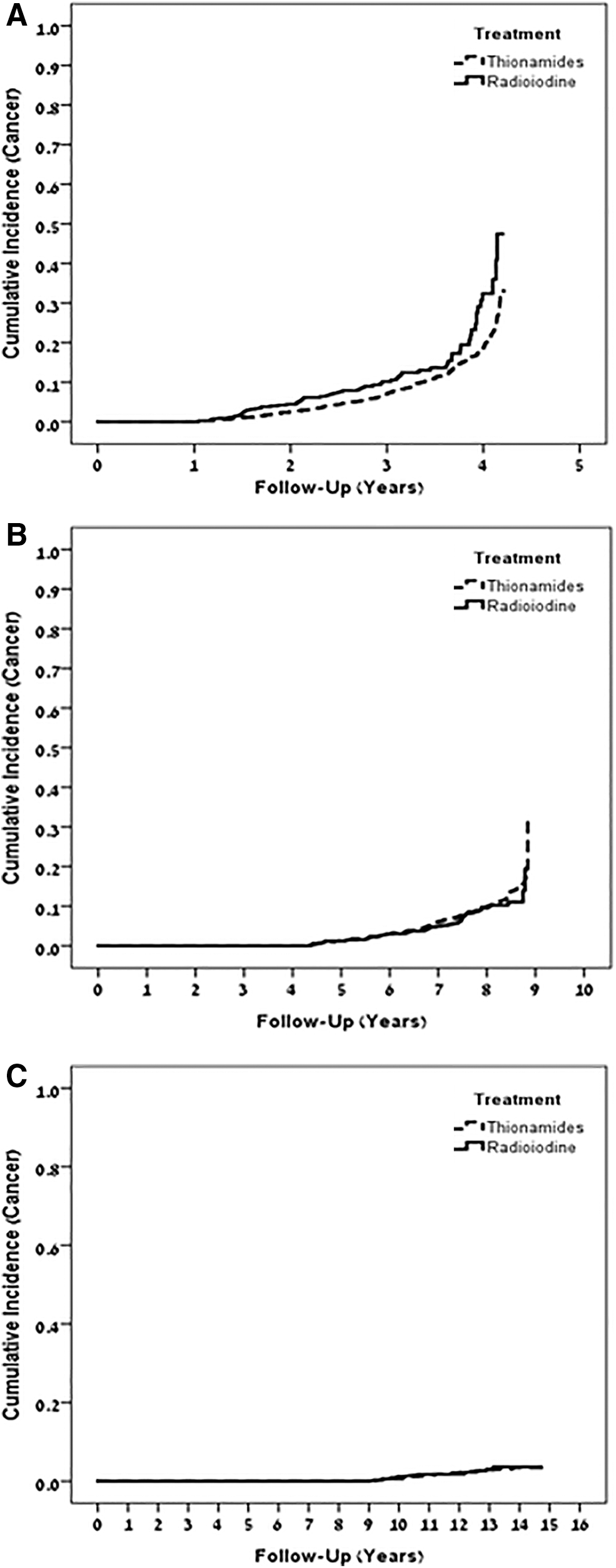
Kaplan–Meier curves showing cumulative cancer incidence in patients with hyperthyroidism that began treatment with thionamides or with radioiodine, by tertiles of length of follow-up: (
Specifically for NHL, when stratified by tertiles of length of follow-up, risk associated with radioiodine was 6.72 [CI 1.37–33.08], p = 0.02 in the first period of follow-up, and there was no statistically significant increased risk associated with radioiodine treatment in longer follow-up periods: HR = 2.58 [CI 0.59–11.32], p = 0.21; HR = 0.81 [CI 0.09–7.67], p = 0.86 for 4.2–8.9, and >8.9 years of follow-up, respectively, in multivariable analyses.
Discussion
In this cohort study with 123,166 PYs of follow-up, there was no association between radioiodine treatment for hyperthyroidism and an increased risk for incident cancer in long-term follow-up. Studying specific cancer types, there was an association between radioiodine exposure and an increased risk for NHL, in univariate but not in multivariable analysis, and a borderline association with a decreased risk of thyroid cancer.
Radioiodine can cause damage to the bone marrow, leading to chromosomal aberrations and, eventually, malignant transformation. Acute and late chromosomal damage were found in peripheral lymphocytes of patients who received various doses of 131I, either for thyrotoxicosis or for thyroid cancer, with a higher recovery ratio in the thyrotoxicosis patients (18). Leukemogenic effect of radiation have a latent period of at least 2 years (19), while tumorigenic effects reported in solid organs are longer than that (20).
In a cohort of 308,297 radiation-monitored workers, the greatest association was between cumulative dose of ionizing radiation and death caused by chronic myeloid leukemia, but there was also an association with mortality from NHL, and from other hematological malignancies (21).
Reports of the association between 131I for hyperthyroidism and cancer are inconsistent. In a retrospective cohort study (13) of women treated between 1946 and 1964 at the Mayo Clinic, a significantly increased risk of thyroid cancer (relative risk 9.1) was observed in 131I treated women, compared with surgically treated women, although this might have been related to the fact that the surgery group had less thyroid tissue at risk. None of the relative risks for the other sites were significantly different from unity. In the American Cooperative Thyrotoxicosis Therapy Follow-up Study (22) 131I therapy was not linked to overall cancer mortality or to mortality from any specific cancer, after excluding patients treated surgically, and with former malignancies.
Among 2793 patients in Finland, and age- and sex-matched controls from the population, the overall cancer incidence was higher among patients than in controls (rate ratio [RR] = 1.25 [CI 1.08–1.46]). The risk of cancers of the stomach (RR = 1.75 [CI 1.00–3.14]), kidney (RR = 2.32 [CI 1.06–5.01]), breast (RR = 1.53 [CI 1.07–2.19]), and unspecified site (RR = 2.22 [CI 1.00–4.90]) was increased (12). There was a 5-year latent period before the cancer incidence began to differ between groups, and the relative risk of cancer increased with higher 131I activities. Because the control group in this study comprised matched subjects from the general population, they could have been under less rigorous health checkups and thus detection bias might have influenced the results.
In 10,552 patients in Sweden, 1950–1975, the SIR for cancer was 1.06 [CI 1.01–1.11]. Significantly increased SIRs were observed for cancers of the lung and kidney. Among 10-year survivors, cancers of the stomach, kidney, and brain occurred significantly above expectation, and except for stomach cancer, there was no significant time-trend or dose–effect for any of the cancer sites or for all cancers combined (11). In a cohort study in England of 7417 patients with 72,073 years of follow-up, there were significant increases in incidence of cancers of the small bowel and thyroid, compared with the general population, but with a significant decrease in overall cancer incidence (14).
A recently published extended follow-up on 18,805 patients of the Cooperative Thyrotoxicosis Therapy Study, treated between 1946 and 1964, confirmed a dose–response relationship, by showing an association between 131I calculated activity absorbed by each organ and outcomes of mortality from solid cancers; a minority of the excess mortality risk, when compared with the general population, occurred in the first 20 years after treatment. There was no dose–response association with death from thyroid cancer, despite the high calculated activities received by the thyroid (23).
In this study, we observed an overall cancer incidence of 6.70 [CI 6.26–7.17] cases per 1000 PYs of follow-up, similar to rates reported in other western countries (24). We have observed a decreased risk of thyroid cancer associated with radioiodine, compared with the risk associated with thionamides. Because the thyrocytes are targeted and destroyed by the radioiodine, we speculate that this may result in a decrease in the incidence of well-differentiated thyroid cancer. Prior studies may not have been able to assess this because many patients were treated with smaller activities of 131I before the year 2000 and many of them had to be repeated due to failure (25). Hence, a significantly greater volume of surviving thyrocytes would have been expected in those older cohorts, which may have resulted in an increased risk of subsequent differentiated thyroid cancer in a subset of patients.
We tried to get an indirect measure of administered 131I activities in this study by counting the number of radioiodine treatments received. We have found that >95% of the radioiodine-exposed patients received only one radioiodine treatment, which suggests the use of radioiodine activities that are generally sufficient to cure hyperthyroidism and destroy the majority of the thyroid.
There was a tendency toward a decreased risk of urinary cancer with radioiodine. Because 131I is cleared renally, accumulation of radioiodine occurs in the urinary bladder. In a study by Hoffman et al. (13) there was a tendency toward an increased risk of bladder cancer, while Franklyn et al. (14) reported a significant decrease in the incidence of bladder cancer.
Our study has some limitations. The first limitation is the possibility of a differential bias. For example, physicians could have recommended radioiodine treatment to older patients more often than recommending thionamides. However, to reduce this bias, we included age, smoking, obesity, major chronic diseases, socioeconomic status, and screening adherence measures, as potential confounders in the multivariate analyses. Nevertheless, the higher mortality rates we have observed in the thionamide-treated patients might reflect unmeasured confounders such as ischemic heart disease or functional status associated with the choice of treatment by physicians and patients.
Second, detection bias might have occurred, because patients treated only with thionamides required closer endocrinology follow-up as the hyperthyroid state was not cured as in the radioiodine group. Moreover, closer follow-up could have detected earlier occult cancer cases. Thyroid cancer is a prime example for which intensified surveillance could have resulted in an increased incidence of early cancers with indolent behavior (overdiagnosis) (26). This overdiagnosis bias would tend to increase cancer detection in our control group and would thus affect the decreased risk observed in association with radioiodine.
The third limitation is our inability to include radioiodine activities in the analysis due to lack of radioiodine dosing data. However, by counting the number of radioiodine treatments received by each patient to achieve response we have an indirect estimate of the administered activities.
The fourth limitation relates to the incidence of specific cancers in Israel. Stomach cancer, for instance, has a wide geographic variation worldwide. While the highest age-standardized rate (found in Eastern Asia, Eastern Europe, and South America) can reach >60 years, in Europe the age-standardized rate is 13.7, and Israel, similar to North America, has one of the lowest rates, with an age-standardized ratio of 8.64 and 4.89 for Jewish males and females, respectively, and slightly lower rates for Arabs (27). Because of the small number of stomach cancer cases found in Israel, random error could have occurred in our study while evaluating a possible stomach cancer association with radioiodine.
Strengths of our study include the large population-based cohort used with a long-term follow-up, relying on a complete clinical database, and an active control group, as well as statistical adjustments implemented for minimizing confounding. By applying a new-user design, we required that both groups had been recently evaluated by a physician; therefore, the groups were likely to be more similar than comparing incident users versus nonusers, or versus ongoing users of another drug.
In conclusion, we show in this observational cohort study that treatment with radioiodine for hyperthyroidism is not associated with an increased risk for overall cancer. However, there might be an association with an increased risk for NHL. Prospective studies might be warranted for confirmation of the results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Table S1