
Abstract
Background:
The ultimate clinical goal of advanced cancer treatment is improvement of survival. Tyrosine kinase inhibitors (TKIs) were recently approved for radioiodine-refractory differentiated thyroid carcinoma (RR-DTC) that is resistant to conventional therapies since they have significant potential to improve survival in patients who previously had no more treatment strategies available. However, eligible patients are limited in clinical practice, making it difficult to accurately determine the efficacy of TKIs.
Patients and Methods:
We retrospectively analyzed the efficacy of lenvatinib at a single institution, enrolling 42 RR-DTC patients.
Results:
The best overall response was partial remission in 26 (62%) patients, stable disease in 10 (24%) patients, and progressive disease (PD) in 6 (14%) patients. The results indicated three-year overall survival (OS) and progression-free survival rates of 51.0% and 32.4%, respectively. Twenty-three (55%) patients had backgrounds that did not match the inclusion criteria of the Study of (E7080) Lenvatinib in Differentiated Cancer of the Thyroid (SELECT) trial. Furthermore, PD-experienced patients individually decided whether to continue lenvatinib, and 17 (41%) made the decision themselves; these patients had a three-year OS of 43.0% and postprogression survival (PPS) of 13.3 [95% confidence interval 6.1–not reached] months.
Conclusions:
Our real-world investigation revealed that patients have wide-ranging background characteristics, and the decision regarding continuation of therapy after PD is based on the patient's general condition. Our management protocol resulted in good PPS. Furthermore, our results indicated equivalent efficacy of lenvatinib as in the SELECT trial. In conclusion, lenvatinib proved effective for RR-DTC patients in a real-world setting.
Introduction
Lenvatinib is one of the tyrosine kinase inhibitors (TKIs) approved for radioiodine-refractory differentiated thyroid carcinoma (RR-DTC) patients. In the phase 3 Study of (E7080) Lenvatinib in Differentiated Cancer of the Thyroid (SELECT) approval trial, lenvatinib resulted in significant prolongation of progression-free survival (PFS) in RR-DTC patients (hazard ratio: 0.21 [99% confidence interval (CI) 0.14–0.31]; p < 0.001) (1). These results indicated that lenvatinib is a promising agent in the treatment strategy of RR-DTC. However, only a small number of RR-DTC patients can be considered candidates for TKI because RR-DTC does not always present with life-threatening progression (2 –4).
Although clinical trials are the best source of evidence for clinical use, we should recognize that the aims of clinical practice are different from those of clinical trials. In the real world, individual treatment is initiated to prolong survival and prevent decline in tumor-related quality of life (QOL) (5), while clinical trials aim to demonstrate the safety and efficacy of therapy. Hence, the primary endpoint in the SELECT trial was PFS and not overall survival (OS) (1).
In fact, few reports are available on the usefulness of lenvatinib in a real-world setting. In this study, we retrospectively investigated the efficacy of lenvatinib for RR-DTC patients using a single-institutional standardized strategy.
Patients and Methods
Patients
A total of 42 patients with RR-DTC treated with lenvatinib between May 2015 and February 2018 at Ito Hospital, Tokyo, Japan, were included in this retrospective cohort study. Patients with pathologically confirmed and proven RR-DTC were included as subjects. “Radioactive iodine (RAI) refractory” tumors were defined as targeted tumors that did not demonstrate RAI uptake on any RAI scan or had progressed despite demonstration of RAI avidity. Patients who were expected to experience survival improvement in conjunction with performance status (PS) improvement by lenvatinib were included, regardless of their Eastern Cooperative Oncology Group (ECOG) PS at baseline. Decision-making regarding treatment initiation was made at a hospital conference for each patient who had tumor-related symptoms, rapid tumor progression, or in whom the size of the tumor itself was life threatening. Lenvatinib was basically chosen as a first-line agent for RR-DTC patients based on the evidence of clinical trials (1,6) and major global guidelines (7). Lenvatinib was prescribed at a starting dose of 24 mg once daily.
Safety
Patients were followed up regularly after initiation of lenvatinib. Toxicity was monitored at least every two weeks for the first two months, and if the patient's condition was clinically stable, every month thereafter. Severity of adverse events (AEs) was graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) v4.0. Dose modification and interruption were made based on CTCAE grades. The frequency, severity, and time to AEs were evaluated.
Efficacy
In all patients, the target tumor lesions were determined in advance by a single radiologist following the response evaluation criteria in solid tumors (RECIST) guidelines (8). Clinical response was assessed by repeated axial computed tomography (CT) images of the target lesions. The frequency of CT assessment was every four weeks in the first six months and every three to six months thereafter, as a guide. In this retrospective investigation, disease progression was determined only as progressive disease (PD) according to the RECIST criteria, separate from judgment of the clinical usefulness of lenvatinib.
The primary endpoint was OS, and time to treatment failure (TTF) and PFS were evaluated as efficacy measures. OS was defined as the duration between the date of initiation of lenvatinib to death from any cause or to the date of the last follow-up. TTF was defined as the time to which the patients could not receive lenvatinib due to any reason, such as development of PD, AEs, or general condition failure. PFS was defined as the duration to disease progression or last follow-up. Other efficacy measures of tumor response, such as response rates, were also analyzed. Differences in clinical background characteristics of the study cohort from those of patients in the SELECT trial were also investigated.
Statistics
Statistical analyses were performed using JMP12 software (SAS Institute, Inc., Cary, NC). Continuous variables are presented as medians with interquartile ranges or mean with standard deviation. Survival curves were plotted using the Kaplan–Meier method, and the log-rank test was used to determine significance. Fisher's exact test was used to compare the prevalence or distribution of two variables. Differences in numerical values between two groups were compared by Welch's t-test. All p-values were two-sided, and p-values <0.05 were considered statistically significant.
This study protocol was reviewed and approved by the institutional review board of Ito hospital.
Results
Background characteristics
The baseline characteristics of the 42 patients with progressive RR-DTC are summarized in Table 1. Median age was 66 (range 33–83) years, and 30 (70%) patients were female. Twenty-seven (64%) and 15 (36%) patients had papillary and follicular thyroid cancer, respectively. All patients had unresectable metastasis, most frequently in the lungs (88%), lymph nodes (71%), and bone (48%). The median cumulative RAI dose was 6.2 (range 0.5–29.6) GBq, and all cases were confirmed as RAI-refractory. Two (5%) patients who could not receive RAI due to rapid tumor progression were not proved to be RAI-refractory. A total of 33 (79%) patients experienced tumor-related symptoms due to tumor progression. Before lenvatinib initiation, local treatment was performed as much as possible, including spinal decompression for bone metastasis in 14 patients, and pleural effusion drainage for malignant pleurisy in 4 patients. These strategies aimed to improve QOL by eliminating tumor-related symptoms. Accordingly, some of the patients could achieve relief from symptoms before lenvatinib therapy; 21 (50%) patients sustained tumor-related symptoms at the start of lenvatinib. Patients who were symptom-free before lenvatinib initiation were defined as “asymptomatic.” PS at baseline was 0 in 21 (50%) patients, while 9 (21%) patients had PS ≥2, of whom 4 and 2 patients had paralysis and pain due to bone metastasis, respectively. Four (10%) patients had previously received TKIs targeting vascular endothelial growth factor (VEGF) receptors, one each of whom received vandetanib and sorafenib as a part of clinical trials, and two received sorafenib in actual clinical practice. The median sum of tumor diameter according to the RECIST guidelines was 89 (range 11–205) mm. Tumor progression in ≤12 months was seen in 28 (67%) patients, and the median serum thyroglobulin (Tg) doubling time (9) was 0.73 (range 0.17–2.99) years. Serum Tg-Ab levels were negative in 32 (76%) patients at baseline.
Baseline Characteristics of the Patients
ECOG PS, Eastern Cooperative Oncology Group performance status; RAI, radioactive iodine; TAE, transcatheter arterial embolization; Tg, serum thyroglobulin; VEGF, vascular endothelial growth factor.
Safety
Lenvatinib was administered orally at a starting dose of 24 mg daily in all patients. First dose reduction and first dose interruption were experienced on day 15 (2–87) and day 34 (3–395), respectively. The mean daily dose was 11.6 (range 4–24) mg. The mean latest daily dose was 10 (range 4–24) mg at the cutoff date for the analysis (July 27, 2018). Dose interruptions, reductions, and withdrawals due to AEs were required in 36 (86%), 38 (91%), and 4 (10%) patients, respectively.
AEs were seen in all 42 patients (100%) (Table 2). The most frequent AE was hypertension (83%). Proteinuria (79%), appetite loss (74%), hand–foot skin reaction (69%), and diarrhea (64%) were also common AEs. These events were mainly of grade 1 or 2 severity, with grade 3 severity being most frequent for proteinuria and hypertension.
Summary of Adverse Events
HFS, hand–foot syndrome.
Lenvatinib was discontinued due to AEs in four patients, due to renal dysfunction in two and hepatic dysfunction and cholangitis in one patient each, respectively.
Efficacy
At the cutoff date for analysis, the median follow-up period was 15.4 (range 1.0–38.4) months, and the duration of treatment was 14.9 (range 0.4–38.4) months. Efficacy measures are summarized in Table 3. The best overall response was partial remission (PR) in 26 (62%) patients, stable disease (SD) in 10 (24%) patients, and PD in 6 (14%) patients. None of the patients achieved a complete response (CR). Overall response rate was 62%, and disease control rate (duration of CR, PR, and SD) was 86%. Tumor burden, defined as the sum of the largest diameters of target lesions, decreased in 41 (98%) patients. Of them, six patients shifted over to PD according to the RECIST criteria within four weeks from the time of nadir (8) because although their response was good at first, reprogression occurred soon thereafter, and hence, they were classified as PD. The median time to best morphological response in terms of the percentage changes from baseline to nadir was 3.5 (range 0.3–27.1) months. The decision to continue treatment was based on the development of disease progression to unacceptable general condition, and not necessarily considering the RECIST criteria, or until development of unacceptable toxicity.
Assessment of Efficacy
ORR was calculated as CR+PR.
DCR was calculated as CR+PR+SD.
Clinical benefit rate was calculated as CR+PR+sustained SD >23 weeks.
CR, complete response; DCR, disease control rate; ORR, overall response rate; PD, progressive disease; PR, partial response; SD, stable disease.
The median periods of OS, TTF, and PFS were not evaluable [95% CI 15.0–not reached (NR)], 29.2 months [95% CI 13.7–NR], and 13.8 months [95% CI 4.4–NR], respectively (Fig. 1). The OS rate of all 42 subjects as a whole was 51% at three years.
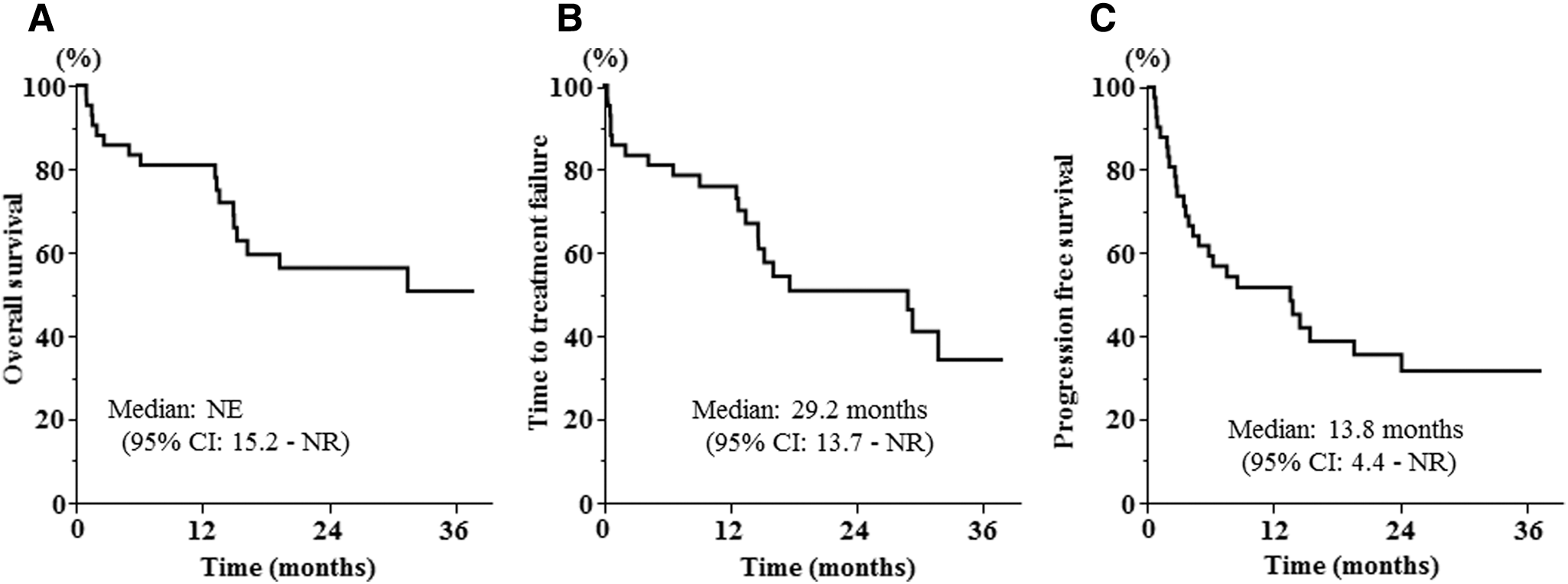
Kaplan–Meier estimate of measures of prognosis with lenvatinib therapy. (
Comparison of the baseline characteristics of 23 (55%) study subjects who met the inclusion criteria of the SELECT trial with those of the remaining 19 (45%) patients who did not meet the SELECT criteria, because of tumor progression in >12 months in 13 patients, ECOG PS of 3 in 4 patients, unproven RAI-refractory disease in 2 patients, blood oozing from tumors in 2 patients, presence of multiple cancers treated with cytotoxic agents not in remission in 1 patient, and among the 4 patients with brain metastasis, unstable lesions treated within a month in 1 patient, showed that background characteristics did not contribute to OS (Fig. 2A). Furthermore, neither rate of tumor progression nor other factors affected OS (Fig. 2B). At the end of the study period, the disease was well controlled in 18 (43%) patients, although 4 (10%) of them discontinued therapy due to AEs. The remaining 24 (57%) patients showed disease progression clinically. Of them, 21 (50%) patients had confirmed PD according to the RECIST criteria and 17 (41%) patients had died of their disease (DOD). The remaining three (7%) had DOD in the absence of tumor evaluation with images, but which was presumed to be due to tumor progression (Fig. 3).

Comparison of clinical outcomes between groups stratified according to background characteristics. (
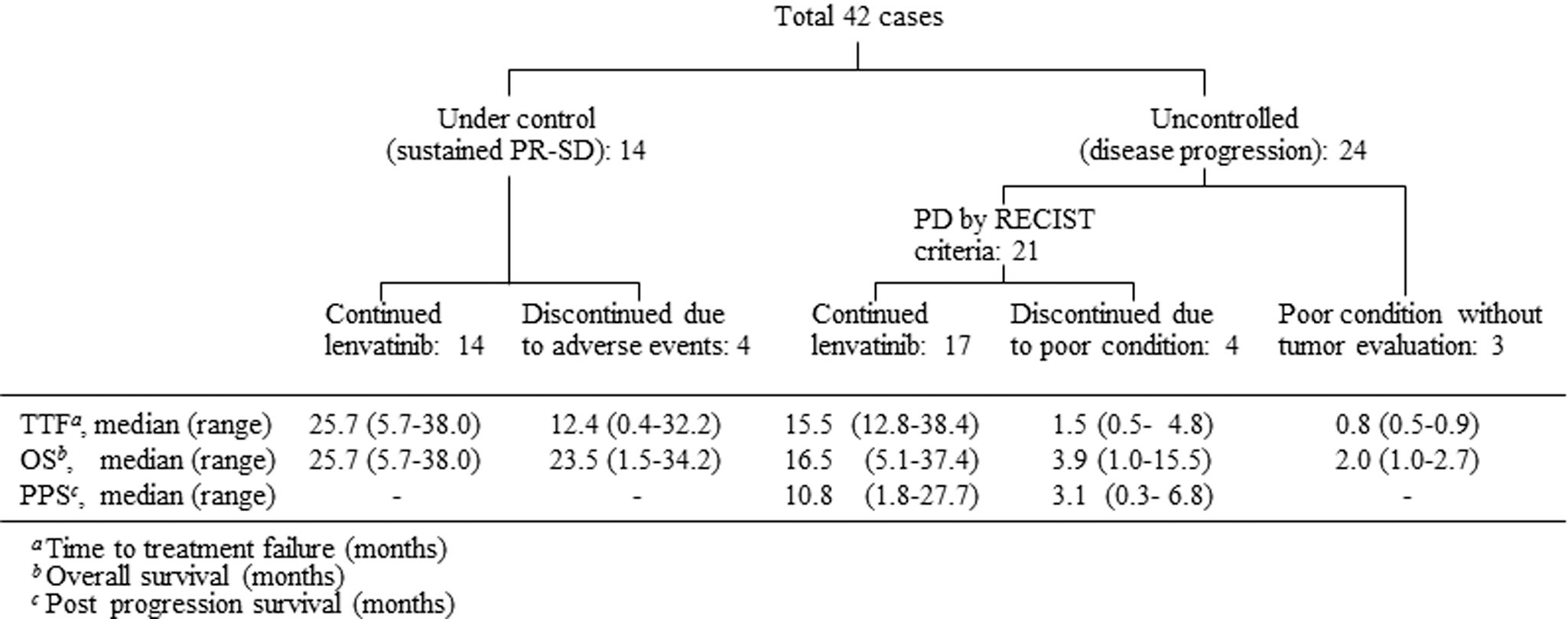
Disease control and PPS. Disease progression was seen in 24 patients; among 21 cases of PD according to the RECIST criteria, 17 continued lenvatinib and 4 discontinued therapy due to poor general condition. TTF, OS, and PPS of each group were investigated. PD, progressive disease; PPS, postprogression survival; PR, partial response; RECIST, response evaluation criteria in solid tumors; SD, stable disease.
Of the 24 patients with disease progression, only patients whose condition allowed them to tolerate therapy decided to continue therapy for long enough to expect a clinical benefit. PD according to the RECIST criteria was seen in 21 (88%) patients. At that time, 17 (41%) patients continued lenvatinib, including with synchronous or subsequent multidisciplinary treatment, and 4 (10%) patients discontinued therapy (Fig. 3). OS of the 17 patients who continued treatment was 32.0 [95% CI 15.2–NR] months (Fig. 4A). Furthermore, the postprogression survival (PPS) period was 13.3 [95% CI 6.1–NR] and 3.1 [95% CI 0.3–6.8] months, respectively, in patients who did and did not continue lenvatinib therapy after developing PD (Fig. 4B). All four patients who discontinued therapy had a PS of 3, their poor condition being due to tumor progression. They all instead moved on to best supportive care because prognostic improvement could not be expected with lenvatinib continuation.

Prognosis classified according to disease progression and treatment decision. (
Discussion
The ultimate clinical goal of advanced cancer treatment is improvement of survival. TKIs were recently approved for RR-DTC that is resistant to conventional therapies (10) since they have significant potential to improve survival in patients who previously had no more treatment strategies available (1,6,11).
Although clinical trials are the best source of evidence for clinical use of drugs and therapies, the aim of actual practice is different from that of trials. Analysis of the results of clinical practice is meaningful since it assesses individual clinical benefits.
However, demonstration of the efficacy of TKIs in real-world practice is not easy because patients who are appropriate candidates for TKI therapy are rare (11). The indications of TKIs in RR-DTC patients are limited; imminently threatening disease progression is expected to require intervention. In fact, little has been reported on the outcomes of patients treated with TKIs in the real world (12,13), and those reports were limited by the small number of subjects or the fact that they did not investigate OS.
In view of these difficulties, we evaluated the efficacy of lenvatinib in a real-world setting, with assessment of OS following treatment based on a uniform strategy at a single institution as the primary endpoint.
Our results show that the three-year OS of RR-DTC patients treated with lenvatinib is 51%, indicating equivalent efficacy as demonstrated in the SELECT trial (1), although we could not compare the effects with those of placebo administration for ethical reasons. The results of TTF and PFS were also similar to those in the SELECT trial.
We analyzed the data from the point of view of baseline background characteristics. About half the patients had background characteristics that were unmatched to the SELECT trial criteria (1). In our study, patients who were likely to benefit from TKIs were strictly selected, and there were no patients in whom TKIs were initiated too early according to widely used guidelines. The results suggest a distinctive feature of real-world practice, namely that decision-making is performed aiming at individual OS prolongation. In patients with these variable background characteristics, OS was not significantly different regardless of tumor growth rate before treatment initiation or existence of other factors that did not match trial criteria. These results seem to suggest the usefulness of lenvatinib for real-world DTC patients, regardless of the variations in patient background characteristics.
TKI initiation is appropriate in cases that have tumor-related symptoms even with slow tumor progression. Several global guidelines (7) and recommendations (5,14) have described that symptomatic patients are candidates for TKIs. Furthermore, the decision to start TKIs should be considered in cases with both small rapidly progressive tumors (over <6–12 months) and those with large slowly progressive tumors (over >12 months) if tumor-associated complications are a concern in the near future. Since lenvatinib has the potential to shrink tumors very quickly (1,15) due to suppression of VEGF signaling (16), as we have also already reported (17), it can cause immediate reduction in tumor-related symptoms. The results of the present study suggest that treatment efficacy can be obtained regardless of the speed of tumor progression at baseline.
In our study, management after disease progression was also investigated. RECIST criteria were adopted for diagnosis of PD in this retrospective investigation, which are the criteria commonly used in clinical trials. In this study, the decision regarding continuation of therapy was made depending on the patients' general condition.
We observed that patients sometimes experience transient tumor progression following interruption of therapy due to development of AEs (18,19). This phenomenon has been proven to involve VEGF signaling in vivo (13,20). Tumor blood vessels not only undergo rapid regression when VEGF signaling is inhibited but also regrow equally rapidly after interruption of therapy. The effect of VEGF inhibition on tumors is not permanent. Some cases demonstrating this phenomenon once again underwent tumor re-shrinkage following readministration of the VEGF inhibitor. The definition of PD according to the RECIST criteria includes ≥20% tumor progression from the best response as one of the criteria for evaluation of the response to therapy, meaning that the greater the amount of tumor shrinkage, the earlier that PD develops in cases with tumor regrowth. Since lenvatinib continuation after RECIST PD was not allowed in the SELECT trial, the utility of continuation can be proved only in actual clinical practice.
There are currently only two approved agents available for RR-DTC patients. Therefore, appropriate use of these two agents is very important. A recent investigation including other malignancies demonstrated that dose escalation can contribute to disease control if AEs are tolerable (4,21,22). Some of our patients were able to continue treatment by taking advantage of dose escalation or arranged interruption to avoid long interruption due to severe AEs, which indicates the significance of skillful dosing with a single drug.
PPS of patients who continued lenvatinib therapy after PD was substantially better than those of patients who discontinued therapy. Treatment continuation has the potential to prolong OS in cancer patients with PD and who are in sufficiently good condition to continue therapy. The significance of PPS has already been described in the strategy for other malignancies (23,24). However, we cannot definitively assert the utility of lenvatinib continuation after PD from our investigation because of its retrospective nature. Compared with the outcomes in the SELECT trial, the PFS period in our study was 13.8 months, which was 4.5 months less than in the SELECT trial. This difference could due to the diversity in patient background characteristics, including the presence of adverse conditions to treatment, as described. Nevertheless, an almost equivalent two-year OS was obtained in both studies, that is, 57% in our study and 58% in the SELECT trial. Equivalent OS regardless of inferior PFS indirectly suggests the utility of the continuation of therapy after PD. Seventeen patients with PD received treatment with lenvatinib, with continuation of therapy and subsequent multidisciplinary treatment, including conventional radiotherapy for new metastases and next line TKIs. A total of six patients who were unable to tolerate lenvatinib but were able to take other TKIs were treated with sorafenib as second-line therapy. However, its prognostic efficacy was uncertain because most patients could not be treated with sufficient amounts of the secondary drug to evaluate its efficacy because of their poor general condition. Thus, the appropriate timing to switch to second-line TKIs needs further evaluation.
Some patients in whom lenvatinib was effective could not continue treatment due to severe AEs. Several AEs, such as loss of weight or appetite, can lead to severe decline in the patients' QOL.
Based on these reports and experiences, not only morphological assessment but also the patients' general condition, age, and PS should be taken into consideration when planning lenvatinib continuation (25).
In the future, evidence-based suggestions regarding the timing of TKI initiation will be needed. Initiation without proper evaluation of whether the patient is an appropriate candidate for therapy should be avoided because TKIs can cause a variety of AEs (1,26), which can affect QOL (14,27). At the same time, if the disease has progressed too far, there is a greater possibility of appearance of tumor-related symptoms accompanying rapid regrowth after interruption of therapy due to AEs. Maintaining an appropriate balance between disease control and prevention of AEs is an important goal of TKI therapy, which includes initiating therapy at an optimal time (28 –30). Therefore, further consideration of initiation timing is very important.
A limitation of this study is the small cohort size.
We analyzed the efficacy of lenvatinib in real-world clinical practice, focusing on the differences versus clinical trials. Despite the fact that patients in the real world have a varied background, they were able to obtain favorable outcomes that were similar compared with the SELECT trial. We acknowledge that adoption of a multidisciplinary strategy that includes lenvatinib continuation after development of PD led to an overall good prognosis in this study. With our patient selection and disease control, a three-year OS of 51% was obtained. In conclusion, lenvatinib is effective in the treatment of RR-DTC patients in the real world.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.