
Abstract
Introduction:
The American Joint Committee Cancer (AJCC) TNM system predicts survival in patients with differentiated thyroid cancer (DTC). In the eighth edition of the AJCC TNM, microscopic extrathyroidal extension (microETE) was removed and tumor size >4 cm was maintained in the definition of T3 disease to reduce unnecessarily aggressive therapy for adults at low risk of death from DTC. In pediatric patients where DTC survival rates are high, the AJCC TNM is used to identify patients at increased risk of persistent, postsurgical disease, to identify patients who benefit from radioactive iodine therapy. The aim of this study was to assess the correlation of microETE with cervical lymph node (LN) metastasis in pediatric patients and to determine if tumor size or microETE is more informative in predicting regional LN disease.
Methods:
Patients with DTC <19 years of age at the time of thyroidectomy with AJCC T3 tumors (seventh edition) and the presence of LNs on the surgical specimen were included in this retrospective chart review. Pathological findings were confirmed by pathologist review.
Results:
Forty-five patients with AJCC T3 designation were included, 34 with microETE and 11 without microETE. Of those with microETE, 32 (94.1%) demonstrated regional LN metastasis compared with 5/11 patients (45.5%) without microETE (p = 0.001). In addition, microETE was associated with lateral neck LN metastasis (p = 0.004), bilateral disease (p = 0.001), and tumor multifocality (p = 0.003). Patients with microETE had smaller tumors (median = 2.5 cm, interquartile range [IQR]: 1.6–4.5) compared with patients without microETE (median = 5 cm, IQR: 4.2–5.4; p = 0.02). No increased association was found between microETE and vascular invasion, distant metastasis, or persistent/recurrent disease.
Conclusions:
In pediatric patients with DTC, microETE is a strong predictor of LN metastasis when compared with tumor size. For patients who do not undergo prophylactic central neck LN dissection, the presence of microETE predicts an increased risk of postsurgical disease and should be included in future revisions of the American Thyroid Association pediatric risk stratification categories.
Introduction
Differentiated thyroid cancer (DTC) is the most common form of endocrine neoplasm in children (1). Similar to adults, the incidence of DTC has increased significantly over the last two decades, with the most significant increase seen in adolescent girls, where papillary thyroid cancer (PTC) is now the second-most common malignancy between the ages of 15 and 19 years (2 –4). The majority of pediatric PTC is sporadic and occurs in patients with no identifiable risk factors. At the time of presentation, PTC is frequently associated with regional lymph node (LN) metastasis and this risk of LN involvement increases with tumor size, multifocal disease, and extrathyroidal extension (5).
In the United States, several scoring systems are designed to predict the risk of disease-specific mortality in adults with thyroid cancer (6 –9). The overall survival rate in pediatric patients diagnosed with DTC is more than 98%; thus, disease-specific mortality is not a useful metric to stratify treatment intensity or to assess therapeutic efficacy. Rather, the goal of optimizing care in pediatric DTC is to reduce morbidity, both surgical and medical complications, and side effects, without increasing the risk of persistent or recurrent disease.
The inaugural American Thyroid Association (ATA) pediatric guidelines offer two recommendations toward this goal: (i) referral to a high-volume thyroid surgeon, defined as a surgeon performing >30 cervical procedures/year, and (ii) recommending against the reflexive administration of postsurgical radioactive iodine (RAI) for patients at low risk of persistent, postsurgical disease. However, the ATA pediatric guidelines provide few recommendations for stratifying the surgical approach, suggesting that all patients with PTC should undergo total thyroidectomy with “consideration” for prophylactic central neck LN dissection even in the absence of extrathyroidal invasion or regional LN metastasis (10).
In the postoperative period, the American Joint Committee on Cancer (AJCC) Tumor, Nodal metastases, distal Metastases (TNM) anatomic classification system is similarly used in pediatrics as in adults, to describe the anatomic pathological features of the tumor and metastatic disease. In the seventh edition of the AJCC TNM, tumor (T) classification is divided into six categories based on tumor size and degree of invasion into adjacent tissues, referred to as extrathyroidal extension (ETE). Tumors are designated T3 if the tumor size is >4 cm or if microscopic ETE (microETE) is found on anatomic pathology, defined as tumor growth outside of the thyroid gland into the sternothyroid muscle or perithyroidal soft tissues not visible by gross examination (11). In contrast, the designation of extensive or macroscopic ETE (macroETE) is used for tumors where invasion into perithyroidal tissue is grossly visible during surgical dissection, including with invasion into subcutaneous soft tissues, the larynx, trachea, esophagus, or recurrent laryngeal nerve (12).
In the adult literature, there is ongoing debate regarding whether microETE correlates with disease-specific morbidity and mortality. Those in support of removing microETE from the AJCC TNM staging system refer to data showing no effect of this on recurrence risk or long-term outcomes (13,14). Those who support continued inclusion of microETE refer to data reporting a correlation between this and an increased risk of LN metastasis (15,16), extranodal extension (17), higher recurrence (15), and compromised survival (15,16). Ultimately, in the eighth edition of the AJCC TNM, microETE was removed as a criterion for T3 designation, leaving size as the only anatomic feature used to stratify T1 to T3a disease (9).
In pediatrics, the AJCC TNM system is used to identify patients who are at increased risk of persistent, postoperative disease, who would benefit from RAI adjuvant therapy (10). The present pediatric version of the ATA guidelines does not use the presence or absence of microETE to stratify the risk of persistent postsurgical disease; yet, recent data suggest a correlation between microETE and an increased risk of regional LN metastasis (18,19). This observation is particularly salient when considered within the context of ongoing discussion whether prophylactic central neck dissection should be performed for all pediatric patients with a preoperative diagnosis of PTC (20).
Confirming whether microETE predicts invasive behavior is important to stratifying the risk of persistent, postsurgical disease. Consequently, the aim of this study was to assess the correlation of microETE with cervical LN metastasis in pediatric patients and to determine whether tumor size or microETE serves as a more informative predictor for regional LN disease. With the incorporation of ETE as a high risk criterion for malignancy in the American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS), as a secondary aim, we also reviewed the preoperative ultrasound (US) studies for each patient to assess the sensitivity and specificity of US to identify microETE subsequently confirmed by surgical pathology (21).
Methods
Patients diagnosed with DTC at the Children's Hospital of Philadelphia (CHOP) Thyroid Center between January 2009 and June 2017 with 1-year follow-up data through May 2018 were eligible for inclusion in this retrospective chart review if they met the following criteria: age <19 years at the time of thyroidectomy, thyroidectomy performed at CHOP, AJCC T3 tumors as defined by the seventh edition, and the presence of LNs on the surgical specimen or identified on the postsurgical RAI whole-body scan (Fig. 1). This study was approved by the Institutional Review Board at CHOP.
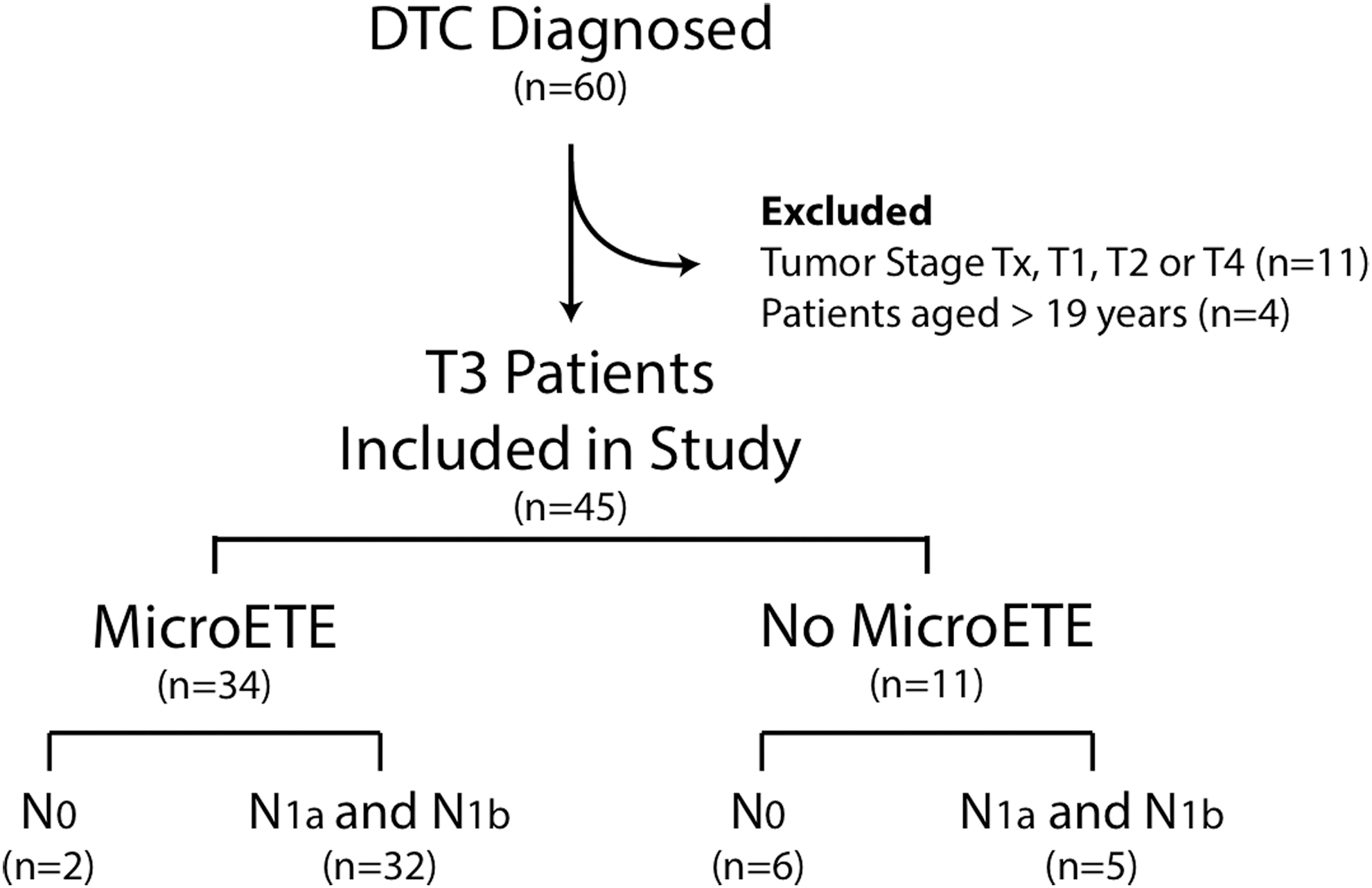
Summary of patients included for analysis.
Demographics, including age, sex, race/ethnicity, date of thyroidectomy, and final surgical pathology diagnosis, were extracted from each patient's medical record. Histopathological variables assessed and extracted from pathology reports included the following: extrathyroidal extension, tumor size, tumor laterality, tumor focality, vascular invasion, extranodal extension, regional LN metastasis, and/or distant metastasis. Two pathologists (N.D.N. and L.F.S.) separately performed a histopathology review to confirm the final diagnosis, extent of disease, and tumor characteristics. Tumor pathology was classified according to the 2017 World Health Organization-published recommendations and the AJCC seventh edition. MicroETE was defined by the presence of one or two microscopic foci measuring ≤5 mm each located outside of the thyroid capsule with extension into perithyroidal soft tissue or skeletal muscle tissue (22). Tumor size was determined based on the largest dimension of the thyroid carcinoma. Tumor focality was classified as either unifocal or multifocal. Tumor laterality was classified as unilateral (presence of carcinoma in one lobe) or bilateral (presence of carcinoma in both lobes). Vascular invasion was classified as present or absent in patients with PTC, and the number of blood vessels involved was recorded in patients with follicular thyroid carcinoma. Central neck LNs (levels VI) and lateral neck LNs (levels II, III, IV, and V) removed by the surgeon were assessed as evidence of regional LN metastasis. If regional LNs were not evaluated at the time of surgery, LN metastasis was assessed from postoperative RAI whole-body scans. Representative histopathological images of microETE and macroETE are shown in Figure 2.

Extrathyroidal extension in pediatric papillary thyroid carcinoma. (
Thyroid US scans were reviewed (A.J.B.) to determine the location and TI-RADS score (23,24). Extrathyroidal extension was defined by the presence of tumor clearly protruding into the perithyroidal tissue with loss of the perithyroidal echogenic line (25). US images were viewed in transverse and longitudinal orientation and CINE clips were also reviewed when available to confirm tumor protrusion through the perithyroidal echogenic line compared to capsular abutment with or without bulging into the anterior tissue planes. The reviewer was blinded to which nodules had histologic confirmation of microETE during review of the US images.
Clinical outcomes were obtained from patient medical records and confirmed by the patient's primary endocrinologist (A.J.B. and S.M.M.). Persistent disease was assessed by review of postoperative thyrotropin (TSH)-stimulated thyroglobulin (Tg) and diagnostic whole-body scan images, when available, or by TSH-suppressed Tg and neck US at one year postinitial treatment. At one year, biochemical remission was defined as undetectable Tg antibodies and titers. Anatomical remission was defined by lack of identifiable thyroid carcinoma and metastasis on US cross-sectional imaging or whole-body scan. Persistent disease was determined if criteria for remission were not met at the time of the chart review.
Statistical analysis was performed using IBM SPSS Statistics version 24 (IBM, Armonk, NY). Chi-square analysis was calculated for categorical variables. Normally distributed continuous variables were compared using Student's t-test or Mann–Whitney U test as indicated for nonparametric data. Statistical significance for analysis was determined to be p-value <0.05.
Results
Forty-five patients with T3 classification under the seventh edition of the AJCC TNM system were eligible for inclusion in this study (Fig. 1). The median (interquartile range [IQR]) patient age was 15.3 years (13.7–17.7). Patient demographics and diagnostic information on histopathological diagnoses for included patients are shown in Table 1.
Characteristics of Pediatric and Adolescent Patients with T3 Differentiated Thyroid Cancer (n = 45)
Other includes tcvPTC, cmvPTC, and sPTC.
cmvPTC, cribriform-morular variant PTC; dsvPTC, diffuse sclerosing variant PTC; FTC, follicular thyroid carcinoma; fvPTC, follicular variant PTC; microETE, microscopic extrathyroidal extension; PTC, papillary thyroid cancer; sPTC, solid-variant PTC; tcvPTC, tall-cell variant PTC.
The presence of microETE was associated with increased likelihood of central (p = 0.001) and lateral neck LN metastasis (p = 0.004), and bilateral (p = 0.001) and multifocal tumors (p = 0.003). Twenty-three of the 34 patients (69.7%) with microETE had bilateral disease (p = 0.001) and 24/34 (70.6%) had multifocal disease compared with 1/11 (9.1%) and 2/11 (18.2%) without microETE.
Tumor size >4 cm was not associated with an increased risk for microETE (Table 1) with smaller tumor size associated with microETE (median [IQR] 2.5 cm [1.6–4.5] vs. 5.0 cm [4.2–5.4], p = 0.002) (Table 2). However, there was considerable overlap in tumor size between these two groups (Fig. 3). MicroETE was not significantly correlated with vascular invasion, distant metastasis, or persistent disease assessed one year postinitial therapy (Table 2).
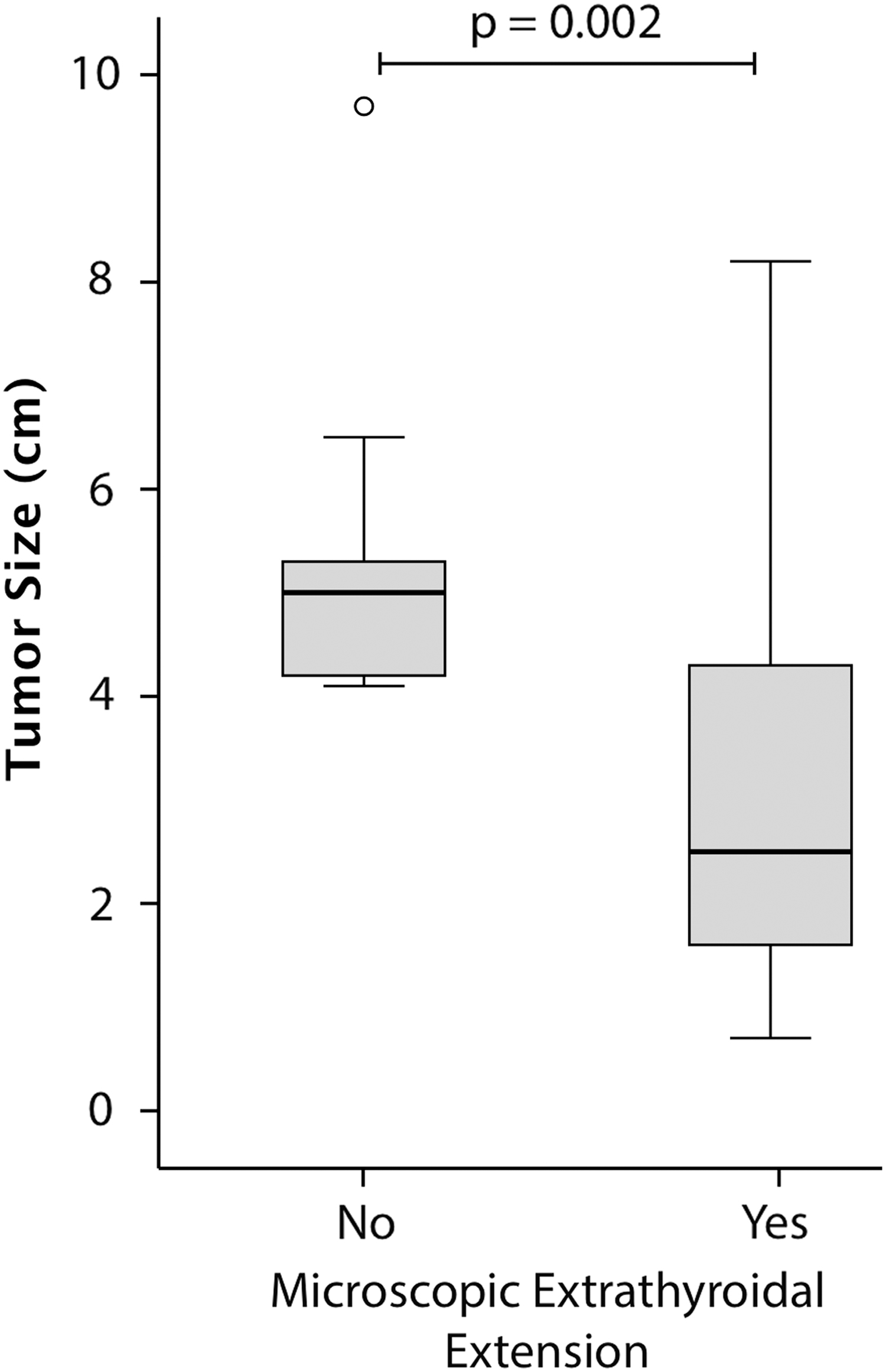
Tumor size in patients with and without microETE. Patients with microETE had smaller tumors compared with patients without microETE (median [IQR] = 2.50 [1.6–4.6] cm vs. 5.00 [4.2–5.4] cm).
Comparison of Histopathological Factors and Clinical Outcomes by Microscopic Extrathyroidal Extension
IQR, interquartile range; LN, lymph node.
Preoperative thyroid US data are shown in Table 3. Evidence of protrusion of tumoral tissue with loss of the perithyroidal echogenic line was identified in 76% (26/34) of cases with confirmation of microETE on final pathology, with 88% (23/26) of the microETE located at the anterior capsule (surface) of the thyroid. Consequently, preoperative US findings demonstrated a sensitivity and specificity for identifying microETE of 76.5% and 90.9%, respectively. There was no difference in TI-RADS score for lesions identified to have microETE on preoperative US compared with lesions without preoperative US evidence of ETE. However, lesions with ETE had a higher TI-RADS score compared with lesions without ETE, TR5 (seven points or more) compared with TR4 (four to six points), respectively. In addition, lesions with preoperative US evidence of ETE were more likely to display diffuse infiltration rather than a focal nodular appearance.
Clinical Characteristics of T3 Tumors According to Microscopic Extrathyroidal Extension Status on Preoperative Ultrasound
“Diffuse infiltration” refers to tumors that displayed lobar or complete infiltration of the thyroid without a distinct nodule. An “identifiable nodule” describes focal tumors with adjacent normal appearing thyroid. “Anterior location” of the nodule is based on transverse view.
TI-RADS, Thyroid Imaging Reporting and Data System; US, ultrasound.
Discussion
In this study, we found that microETE is associated with an increased risk of regional LN metastasis as well as an increased risk of bilateral and multifocal disease in pediatric patients with DTC. In contrast to previous reports, our data suggest that a larger tumor size is less predictive than microETE in predicting invasive behavior. Patients with microETE tended to have smaller tumors compared with patients without ETE. Preoperative US was informative in predicting microETE, especially for nodules with diffuse infiltration throughout the thyroid lobe extending to the anterior edge of the thyroid. The rate of persistent disease one year after initial treatment was similar in PTC patients with and without microETE, suggesting that the presence of microsETE was not associated with a difference in response to our standard approach to therapy assessed at the one-year postinitial therapy time point.
These data are important particularly in the context of ongoing efforts to refine the approach to surgical and medical therapy according to invasive potential as well as the risk of persistent or recurrent disease. In an effort to reduce the risk of recurrent disease, the 2015 ATA pediatric guidelines on the evaluation and management of thyroid nodules and thyroid cancer recommended that prophylactic central neck LN dissection should be considered for patients with PTC based on tumor focality and size, even in patients without preoperative evidence of ETE or locoregional (lateral neck) LN metastasis (recommendation #12b) (10). However, there is ongoing debate as to whether the benefits of pursuing prophylactic, central compartment LN dissection outweigh the risks of complications of surgery in low-risk patients (20,26,27).
Reliance on pathological diagnosis of microETE is of limited utility in planning surgery, as this cannot be used to accurately select patients who may be at greatest benefit from prophylactic central neck LN dissection. High-resolution sonography has been used to screen patients for central neck compartment LN metastasis. Unfortunately, because the thyroid is typically still in a eutopic location, the sensitivity is reduced, with a reported range between 9.5% and 30% (28 –30). In contrast, the sonographic identification of microETE appears to have greater reliability in identifying tumors that appear to be intrathyroidal, but actually have invasive behavior, with a reported sensitivity and specificity to detect histologic ETE between 63–85% and 69–98%, respectively (30 –33). Blinded review of the preoperative thyroid US from our cohort showed a sensitivity of 76.5% and a specificity of 90.0% for the identification of microETE ultimately confirmed on histology (Fig. 2 and Table 3).
Larger size was not associated with microETE, and, in fact, tumors with microETE had an overall smaller size compared with tumors without microETE (Table 2 and Fig. 3). While the difference in tumor size was significant for patients with and without microETE, the overlap in size between the comparative groups suggests that size may not be a reliable clinical feature to predict microETE or the risk of occult central neck LN metastasis. Future prospective studies are needed to determine the importance of tumor size compared with other features that may correlate with an increased rate of central neck LN metastasis.
This study validates several recent reports that show a correlation between ETE with central neck LN metastasis. Spinelli et al. reported results on 132 pediatric patients who underwent total thyroidectomy, including LN dissection in 87 (65.9%) (19). Tumor multifocality, vascular invasion, ETE, and the presence of LN metastasis in the lateral neck were all associated with an increased rate of central neck LN metastasis and an increased risk of persistent disease (lower rate of disease-free survival) (19). A similar association between ETE, tumor size >4 cm, and multifocal and nodal metastasis was reported by Kim et al. in a review of 1075 pediatric patients in the National Cancer Institute Surveillance, Epidemiology and End Result database (5). In a more recent review of 203 patients <20 years of age followed for a median of 5.5 years, Jeon et al. reported that on multivariate analysis, both micro- and macroETE independently predicted an increased risk of persistent and recurrent disease. Based on their data, they subsequently proposed a revision to the ATA pediatric risk-level stratification system to include the presence of ETE (microscopic or macroscopic) into the ATA “intermediate” risk category as an independent factor to predict persistent, postsurgical disease (18). This addition would parallel the ATA adult guidelines on postoperative risk stratification for the use of RAI (recommendation 51, table 14) (34) as well as recent publications showing a correlation between microETE and an increased risk of LN metastasis as well as reduced disease-free survival (15,16).
Taken together, our results, as well as the results from Spinelli et al. and Kim et al., support the recommendation by Jeon et al. that the presence of ETE should be included in the ATA pediatric risk stratification as a predictor of persistent postoperative disease. With the elimination of microETE from the eighth edition of the AJCC TNM, pediatric thyroidologists must ensure that ETE is reported in the synoptic portion of the anatomic pathology report with increased attention to ensure its consideration during postoperative decision-making. This latter point is particularly important for patients with PTC who do not undergo prophylactic central neck dissection or do not have LN in the anatomic specimen (Nx) (10,18). Prospective data across several pediatric thyroid centers are needed to explore if the presence of bilateral disease, multifocal disease, and ETE noted on preoperative US may be part of a multifactor system that could be used to stratify which patients would benefit from prophylactic, central neck LN dissection.
Our study is limited by its retrospective design, a small-sample population, and selection bias from a tertiary center. Despite these limitations, our study has several strengths. Our data support findings from several recent studies in both the adult and pediatric literature that preoperative thyroid US can not only identify nodules with ETE but also confirm the relationship between ETE and the risk of central neck LN metastasis. Our study is the first to demonstrate that tumor size is not a reliable single factor in predicting invasive behavior and that preoperative sonographic factors, including multifocality, bilateral disease, and ETE, may be stronger predictors for invasive behavior.
Conclusion
The presence of microETE may be identified on preoperative US, is associated with bilateral and multifocal disease, and predicts an increased risk for central neck LN metastasis. In addition, microETE appears to be more reliable than tumor size in predicting invasive behavior. The inclusion of microETE as an intermediate risk factor in the ATA risk levels for the postoperative assessment of persistent disease is particularly important for patients who do not undergo prophylactic central neck dissection or do not have LNs found in the surgical specimen after dissection (Nx). Prospective studies are necessary to validate the sensitivity and specificity of preoperative US in identifying microETE as well as determining the clinical utility of this method for stratifying patients for prophylactic central neck dissection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.