
Abstract
Background:
In the recent American Thyroid Association (ATA) guidelines for adult differentiated thyroid carcinoma (DTC) patients, risk stratification is clearly defined and lobectomy is acceptable for low-risk DTC. However, risk stratification for children with DTC in the ATA pediatric guidelines is rather unclear, and total thyroidectomy is recommended for all patients with any risk. The aim of this study was to attempt risk stratification based on our experience and to consider the appropriate extent of thyroidectomy, especially for low-risk DTC in the pediatric population.
Patients and Methods:
The subjects were 153 patients with DTC ≤18 years old, including 58 patients ≤15 years old and 136 female patients, who underwent initial curative surgery in our hospital between 1979 and 2014. Underlying pathology was papillary thyroid carcinoma in 130 patients and follicular thyroid carcinoma in 23. Risk factors related to disease-free survival (DFS) were analyzed and risk stratification was performed.
Results:
No patient died of the disease and 34 patients (22.2%) developed recurrences. At initial surgery, 30 patients (19.6%) had lymph node metastases diagnosed before initial surgery (cN1) and 9 (5.9%) had gross extrathyroidal extension (ETE). Significant factors related to DFS on multivariate analysis were cN1, ETE, and number of metastatic lymph nodes (NMLNs) ≥10, including microscopic MLNs. According to these factors, subjects were divided into three categories: low risk (no risk factors, n = 89); intermediate risk (1 risk factor, n = 37); and high risk (≥2 risk factors, n = 27). Ten-year DFS rates in the low-, intermediate-, and high-risk groups were 96%, 83%, and 48%, respectively. Only 12% of low-risk patients underwent total thyroidectomy. Because NMLNs become obvious only after surgery, another analysis after excluding “NMLNs” as a factor showed that cN and ETE were significant factors related to poor DFS. According to these two factors, risk stratification was attempted in the same manner. Ten-year DFS rates in the low- (no risk factor, n = 117), intermediate- (one risk factor, n = 29), and high-risk (two risk factors, n = 7) groups were 92%, 59%, and 43%, respectively. Only 12% of low-risk patients underwent total thyroidectomy.
Conclusions:
For low-risk pediatric patients, lobectomy may be sufficient as the initial surgical procedure.
Introduction
Differentiated thyroid cancer (DTC) is the most common pediatric endocrine malignancy, and its incidence is increasing (1 –3). Because of the low frequency of pediatric thyroid cancer, sufficient clinical data have not been available, and thyroid cancer care for pediatric patients is based predominantly on evidence from adult series. Pediatric DTC is different from adult DTC in several respects. The spectrum of genetic mutations in pediatric DTC is reported to differ from that in adult DTC (4). Unlike in the adult population, whether there are “high-risk” histologic subtypes that independently predict the extent of disease at presentation or disease-free survival (DFS) in the pediatric population with DTC is controversial. Although advanced local disease, and distant disease, is often observed in the pediatric and adolescent population at presentation, the patients respond well to surgery and radioiodine therapy, and the cumulative survival rate in this young age group is excellent (5,6). However, recurrence is frequently observed, and several risk factors for recurrence, for instance, multifocality, age, metastatic lymph nodes (MLN) at initial visit, and extent of thyroidectomy, have also been reported (7,8). In the most recent American Thyroid Association (ATA) guidelines for adult DTC patients (9), risk stratification is clearly defined, and lobectomy is an accepted option for low-risk DTC. On the contrary, the proposed risk stratification in the ATA guidelines for pediatric DTC patients (10) is less detailed, because it did not specify any cutoff points for cervical lymph node (LN) metastasis when classifying the risk, and they only defined cervical LN metastasis as minimal or extensive disease. In addition, total thyroidectomy is recommended for all pediatric patients at any risk. There is debate about whether a conservative approach for low-risk patients in the pediatric and adolescent populations is appropriate. In this study, pediatric DTC patients treated in our hospital were retrospectively studied, and risk stratification was attempted based on our experiences. An appropriate treatment strategy for low-risk DTC in the pediatric and adolescent population was also considered.
Patients and Methods
The medical records of 218 pediatric patients aged <19 years at the time of their initial visits and who were diagnosed with DTC from 1979 to 2014 at Ito Hospital were reviewed. Forty-seven patients underwent initial surgery at another hospital and were excluded. Because overall survival was reported to be excellent in pediatric and adolescent DTC, DFS was used as the primary endpoint. Excluding 18 patients who did not undergo initial curative surgery and/or had distant metastases at presentation, 153 patients were the subjects of this study. All the information used in this study, including the patients' characteristics, operative findings, postoperative treatment, and follow-up, was collected from the patients' medical records. Seven patients were referred to other hospitals, and the other 146 patients were followed in the outpatient department of our hospital. Follow-up information for seven patients was obtained through correspondence with other hospitals. The median follow-up period was 14.8 years (range: 13–455 months).
The patients were diagnosed and evaluated preoperatively by palpation, chest X-ray, neck ultrasonography (US), computed tomography (CT), and fine needle aspiration biopsy (FNABC). The thyroid primary tumor and cervical LNs were diagnosed and evaluated by palpation, US examination, and US-guided FNABC. Distant metastases were mainly diagnosed by CT, chest X-ray, or postoperative 131I (RAI) scintigraphy. Synchronous metastases (M1) were defined as distant metastases that were confirmed before initial surgery, or within six months after initial surgery. Metachronous metastases were defined as distant metastases that were detected more than six months after initial surgery. Clinically apparent nodal disease diagnosed by preoperative physical examination, US, FNABC, and intraoperative inspection was defined as clinical N1 (cN1), whereas no clinically apparent nodal disease was defined as clinical N0 (cN0) and microscopic MLNs diagnosed after surgery were defined as pathological N1 (pN1). Neck dissection in patients with cN0 was classified as prophylactic neck dissection and neck dissection in patients with cN1 was classified as therapeutic neck dissection. The lateral neck was defined as levels II–V, while the central neck was defined as levels VI and VII nodal basins using criteria outlined in the ATA description for central neck dissection (11). Based on the location of metastatic LNs, cervical LN metastases were categorized into no cervical LN metastasis (N0/Nx), central cervical LN metastasis alone (N1a), and lateral cervical LN metastases (N1b). This classification was adopted from the eighth AJCC TNM staging system (12). Formerly, US resolution was low, and preoperative evaluation for cervical MLNs was not satisfactory. Before 2000, prophylactic modified neck dissection (pMND) including central and lateral neck dissection, was routinely performed for clinical N0 patients with a preoperative diagnosis of malignancy. Since 2000, clinical N0 patients have been undergoing prophylactic unilateral central neck dissection (pCND) alone. Therapeutic MND is indicated only for cN1 patients, because the resolution power of US has much improved. As for the extent of thyroidectomy, a rather conservative approach, as in adult patients, was adopted (13). Ipsilateral lobectomy has been a standard procedure except for patients with preoperative distant metastasis, patients with bilateral disease detected by US, patients with concomitant benign thyroid disease, and patients with cN1 or gross extrathyroidal extension (ETE). All M1 patients underwent total thyroidectomy as the initial surgical procedure, and subsequent RI therapy was recommended. Every patient was usually followed and examined at ∼1 month, 3 months, 6 months, 12 months, and every 6 months thereafter after thyroidectomy. The serum thyroglobulin (Tg) level was routinely measured at every hospital visit, and, regardless of the serum Tg level, neck US and chest CT were performed once a year. Whenever a gradual increase in the postoperative Tg level was observed in patients who had undergone lobectomy, and neck US was normal, chest CT or positron emission computerized tomography was performed. Patients with positive anti-Tg antibodies were followed by CT and US. If these examinations resulted in detection of metastasis, completion thyroidectomy was performed and followed by RAI scintigraphy. Because total thyroidectomy was not performed for all patients, all recurrences were defined as structural recurrence, and biochemical recurrences were excluded.
The data were analyzed with a statistical software program (JMP 12.0; SAS Institute, Inc., Cary, NC). The Chi-square test was used to compare categorical variables. A receiver operating characteristics curve analysis was performed to determine the optimal cutoff points for variables associated with outcomes. DFS rates were calculated by the Kaplan–Meier method. The factors analyzed in this study were sex, age, histology, cN1, ETE, primary tumor size, number of metastatic lymph nodes (NMLNs), location of MLNs, extent of thyroidectomy, extent of neck dissection, and the period of initial thyroidectomy. Univariate analyses were conducted in relation to DFS, and differences between groups were analyzed for significance by the log-rank test. Multivariate analysis was performed using the Cox proportional hazard model. Risk stratification was performed according to the factors related to survival. Hazard ratios with confidence intervals were also estimated. All p-values were two-sided, and a p < 0.05 was considered significant.
The protocol of this study was reviewed and approved by the Institutional Review Board, and the study was performed in accordance with the Declaration of Helsinki.
Results
Patient characteristics and follow-up outcomes
The patient characteristics are given in Table 1. The subjects were 136 females and 17 males, with a median age of 16 years and ranging in age from 7 to 18 years, including 58 patients at age 15 years or younger. Histological diagnoses of papillary carcinoma and follicular carcinoma were made in 130 and 23 patients, respectively. Eight patients (5.2%) had diffuse sclerosing variant papillary thyroid carcinoma (PTC). Median primary tumor size was 25 mm ranging from 4 to 87 mm. At presentation, 30 patients (19.6%) had cN1 disease, and ETE was observed during thyroidectomy in 9 patients (5.9%). The sites of extension were as follows: the recurrent laryngeal nerve in 7, the trachea in 4, and the esophagus in 2, including overlapping cases.
Patients' Characteristics
Values are given as n (%) except where indicated otherwise.
cN1, clinical metastatic lymph node detected preoperatively; CND, central node dissection; DSVT, diffuse sclerosing variant; ETE, extrathyroidal extension; IQR, interquartile range; MLNs, metastatic lymph nodes; MND, modified neck dissection; N1a, metastatic lymph nodes located in the central neck; N1b, metastatic lymph nodes located in the lateral neck; RAI, radioactive iodine.
Total thyroidectomy was performed in 37 patients (24.2%) and neck dissection was performed in 127 patients (83%). Thirty patients underwent therapeutic modified radical neck dissection, and 97 patients underwent prophylactic neck dissection (pCND for 30 and pMND for 67). Of the 97 cN0 patients, MLNs at level VI were diagnosed histologically in 81 patients (83.5%). Of these, 43 patients (81%) with a primary tumor size ≤4 cm had histological MLNs at level VI, and 55 patients (86%) with primary tumor size >4 cm had histological MLNs at level VI. There was no significant difference in the node-positive patient ratio by the primary tumor sizes. Only eight patients (5.2%) underwent postoperative ablation. No patient died of the disease and 34 patients (22.2%) developed recurrences. Recurrences were observed in regional lymph nodes in 24, in distant organs (lung) in 9, and in remnant thyroid in 6, including overlapping cases. The 34 patients with recurrences consisted of 33 patients with PTC and 1 patient with follicular thyroid carcinoma (FTC). Recurrence was observed in the remnant thyroid in one patient with FTC, and no patient with FTC developed distant metastases.
The 10-, 20-, and 30-year DFS rates were 83.8%, 71.7%, and 53.5%, respectively (Fig. 1).

DFS curve of all patients. The 10-, 20-, and 30-year DFS rates are 83.8%, 71.7%, and 53.5%, respectively. DFS, disease-free survival.
Risk factor analyses and risk stratification
Results of univariate and multivariate analyses are given in Table 2-A. Significant factors related to poorer DFS on univariate analysis were histology (PTC), cN, ETE, neck dissection (MND), NMLNs (≥10), and location of MLNs (lateral neck). Multivariate analysis showed that significant risk factors related to poorer DFS were cN, ETE, and NMLNs (≥10). Based on the three factors identified on multivariate analysis, subjects were stratified into three categories (risk stratification A): low risk (no risk factors, n = 89); intermediate risk (1 risk factor, n = 37); and high risk (≥2 risk factors, n = 27). Recurrences were observed in 6 patients (6.7%), 12 patients (32.4%) and 16 patients (59.3%) in the low-, intermediate-, and high-risk groups, respectively. DFS according to the risk stratification is given in Figure 2A, and it was significantly different among the risk groups. The 10- and 20-year DFS rates were 96.1% and 90.1% in the low-risk group, 66.1% and 54.1% in the intermediate-risk group, and 48% and 28% in the high-risk group, respectively (Fig. 2A). As mentioned in the Patients and Methods section, routine pMND was formerly performed in cN0 patients and cN0 patients who recently underwent no dissection or pCND only. However, DFS was not significantly different in the low-risk group patients between those with and without pMND (Fig. 2B). The risk of recurrent disease was evaluated according to the risk stratification and is given in Table 2-B. The risk of recurrent disease was significantly lower in the low-risk group than in the high-risk group and in the intermediate-risk group. The background characteristics of the patients in these risk groups are given in Table 2-C. Significant differences among the groups were observed in age, sex, tumor size, neck dissection, and ablation. Concerning the extent of thyroidectomy in these risk groups, total thyroidectomy was performed in 12.4%, 32.4%, and 51.9% of the low-, intermediate-, and high-risk groups, respectively; the difference among the groups was significant.
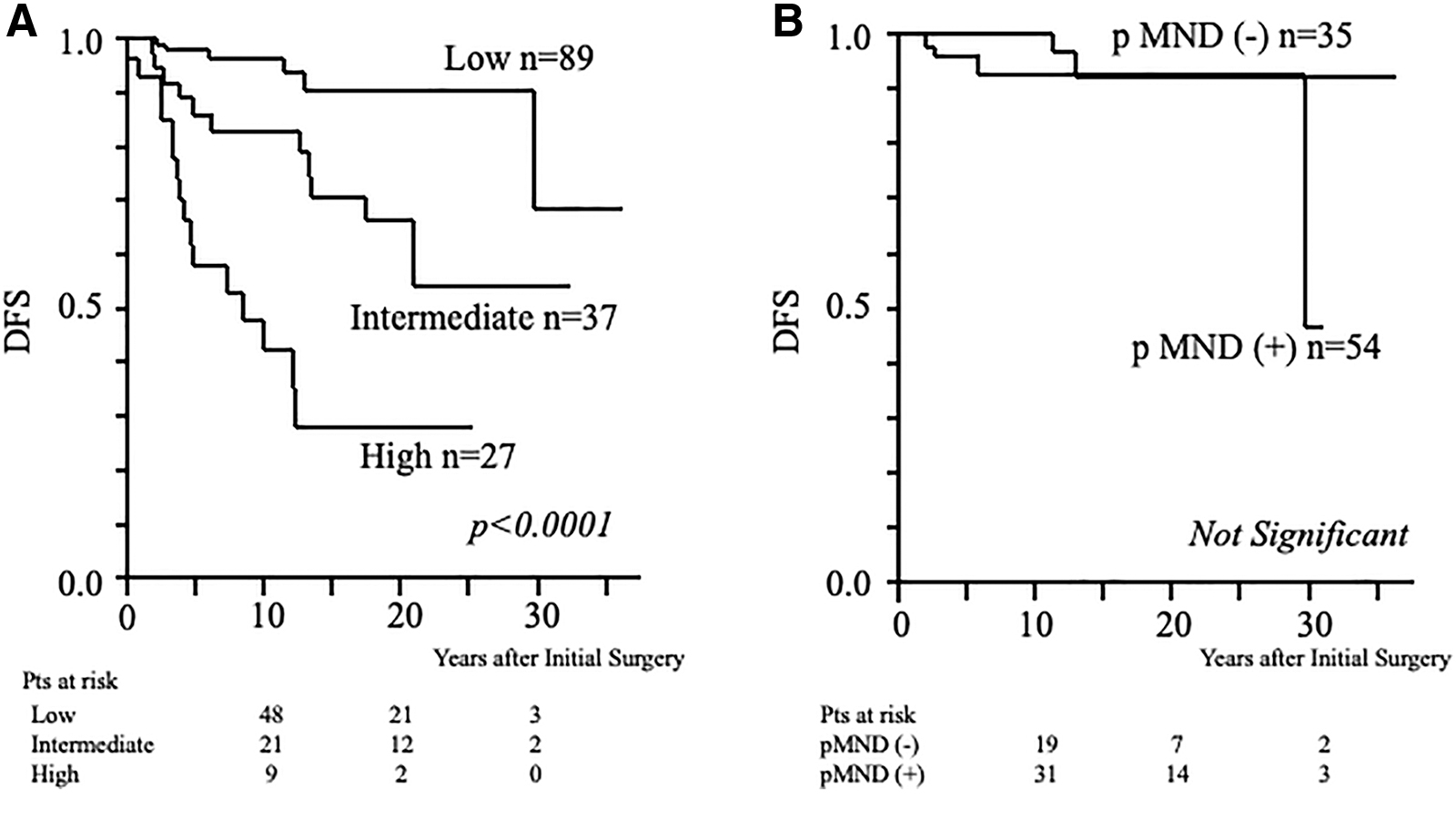
Comparison of DFS curve among risk groups stratified by factors related to poor DFS on multivariate analysis (risk stratification A). (
Risk Factor Analyses Related to Poor Disease-Free Survival and Risk Stratification Including Data of Metastatic Lymph Nodes Diagnosed After Surgery (Risk Stratification A)
Median (years).
CI, confidence interval; cN1, clinical metastatic lymph node detected preoperatively; HR, hazard ratio; LMLN, location of metastatic lymph nodes; Neck dissection, central node dissection and/or modified radical neck dissection; NMLNs, numbers of metastatic lymph nodes; Period, year of initial surgery; PTC, papillary thyroid carcinoma.
Because not all cN0 patients underwent the same extent of neck dissection, NMLNs was not the same between patients with pCND and patients with pMND. Thus, another analysis was performed after excluding NMLNs, and multivariate analysis showed that significant factors related to DFS were cN and ETE (Table 3-A). Risk stratification was attempted according to these two risk factors (risk stratification B). Low-risk patients had no risk factor (n = 117), intermediate-risk patients had one risk factors (n = 33), and high-risk patients had two risk factors (n = 2). DFS according to the risk stratification is given in Figure 3A, and it was significantly different among the risk groups. The 10- and 20-year DFS rates were 92.4% and 81.8% in the low-risk group, 55.7% and 40.6% in the intermediate-risk group, and 0% and 0% in the high-risk group, respectively. In low-risk group patients, DFS was not significantly different between those with and those without pMND (Fig. 3B). The risk of recurrent disease was evaluated according to risk stratification B and is given in Table 3-B. In risk stratification B, as in risk stratification A, a significantly lower risk of recurrent disease was observed in the low-risk group than in the high-risk group and the intermediate-risk group. As to the extent of thyroidectomy in these risk groups, total thyroidectomy was performed in 12.8%, 60.6%, and 66.7% of the low-, intermediate-, and high-risk groups, respectively. Figure 4 shows DFS compared between patients with total thyroidectomy and patients with lobectomy in the low-risk groups obtained from the two risk stratifications. In both groups of low-risk patients, DFS in the patients treated by lobectomy was not significantly inferior to that in the patients treated by total thyroidectomy.
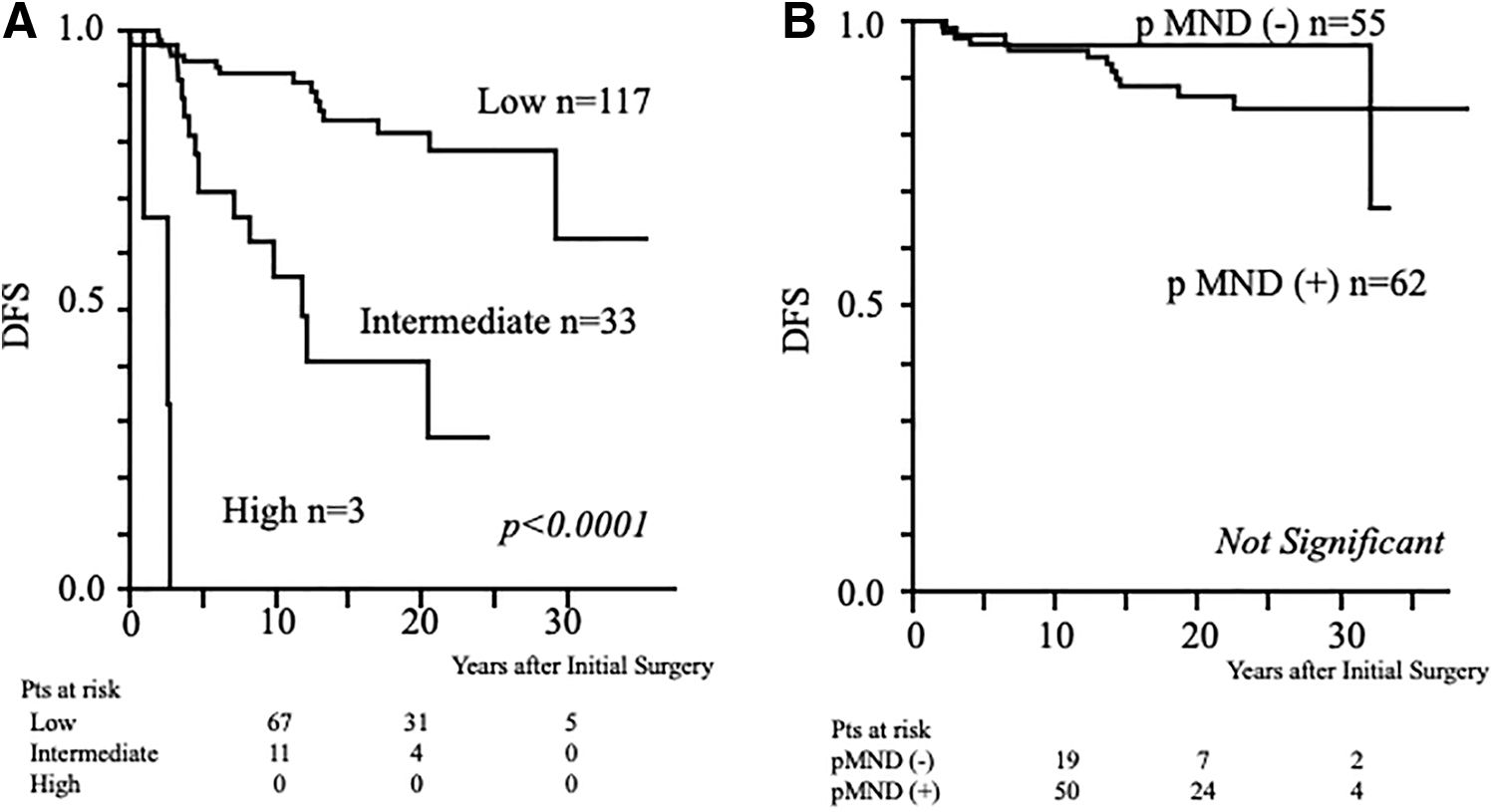
Comparison of DFS curves among risk groups stratified by factors related to poor DFS on multivariate analysis excluding data of metastatic lymph nodes diagnosed after surgery (risk stratification B). (
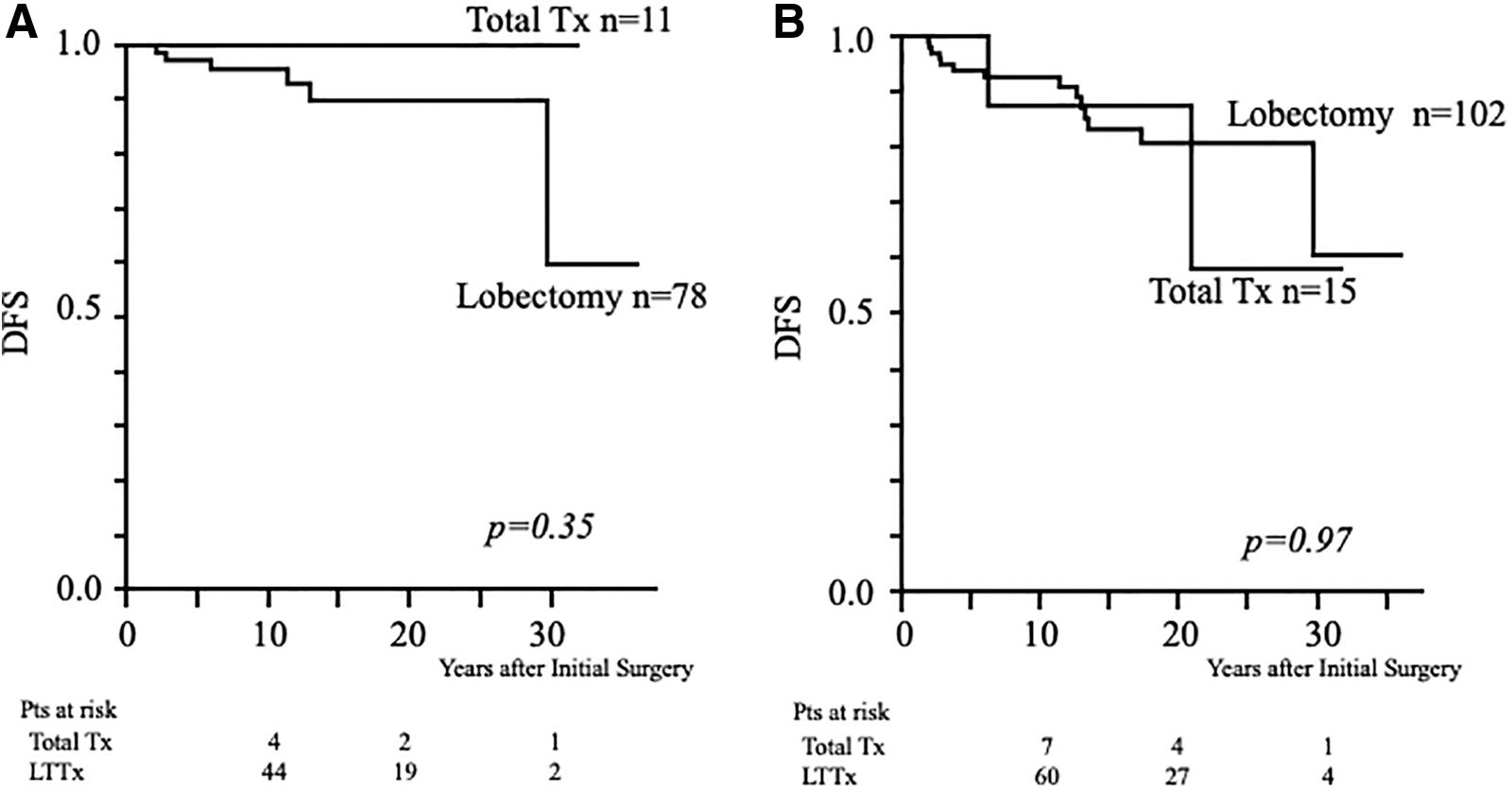
Comparison of DFS between patients with total thyroidectomy and those with lobectomy in the low-risk groups. (
Risk Factor Analyses Related to Poor Disease-Free Survival and Risk Stratification Excluding Data of Metastatic Lymph Nodes Diagnosed After Surgery (Risk Stratification B)
Median (years).
Discussion
For many years, clinical management for adult DTC has been total thyroidectomy followed by radioiodine therapy. However, in the most recent ATA guidelines for adult DTC, specific risk stratification has been introduced, and lobectomy can be considered for low-risk patients (9). Guidelines from other associations (14) also recommend lobectomy for low-risk DTC patients as a surgical option. For pediatric DTC, a single clinical guideline, published by the ATA, exists and recommends total thyroidectomy for all patients regardless of disease extent. In addition, risk stratification is proposed primarily based on the degree of lymph node involvement. However, this risk stratification is not as specific as the risk stratifications in the ATA guidelines for adult DTC. Several studies reported initial and dynamic risk stratifications for pediatric DTC according to their own risk factors or the ATA guidelines (15 –18). These reports showed that DFS was significantly different among the risk groups. The present risk stratification based on our own experience also showed a significant difference in DFS among the risk groups. However, this study differs from these previous reports in several respects. Of the present subjects, only 25% underwent total thyroidectomy, whereas most patients underwent total thyroidectomy in the previous studies. The aim of this study was not only to develop risk stratification for pediatric DTC patients, but to also identify whether total thyroidectomy is necessary for patients at any risk. As in previous reports, the present subjects had excellent disease-specific survival, although recurrences were frequently observed. In this study, ETE, cN, and NMLNs were significant factors related to DFS similar to other studies (17,19,20). Recent studies (15 –17) reported that patients without risk factors, most of whom were treated by total thyroidectomy, had excellent prognoses. Jeon et al. reported their own risk stratification and showed excellent DFS in low-risk patients (17). However, most of their patients were treated by total thyroidectomy with rather short median follow-up (5.5 years). We previously reported that lobectomy, which has been the main surgical procedure in our hospital, was sufficient for low-risk “adult” DTC patients (13). Based on this study, we also suggest that, in the pediatric population, lobectomy is sufficient for low-risk DTC patients, as for adult low-risk DTC patients. Previously, Newman et al. (21) studied 329 DTC patients at age 20 years or younger and concluded that there was no significant difference in DFS between the types of primary thyroid surgery. They analyzed a large number of patients with long-term follow-up and showed that lobectomy was possibly a treatment of choice for low-risk pediatric DTC patients. In their report, patients with more extensive thyroid tumors had an increased likelihood of being treated with total thyroidectomy and patients with less advanced disease were treated with lobectomy. On the contrary, several studies (5,22 –25) concluded that recurrence risk could be reduced by total thyroidectomy. These studies did not consider risk factors related to recurrence. However, the ATA guidelines for pediatric DTC patients were based on consideration of these studies and, thus, recommended total thyroidectomy for all pediatric DTC patients at any risk. Nevertheless, performing total thyroidectomy for all pediatric DTC patients without any exception seems to result in overtreatment. Treatment strategies for pediatric DTC patients should be considered in the light of risk factors related to clinical outcomes, as in adult DTC patients. Risk-adapted management for adult DTC patients is evolving as we consider the high sensitivity of neck ultrasound to stage thyroid cancer and diagnose recurrences. The same consideration should apply for pediatric DTC patients, particularly given the results presented in this study.
There are several limitations in this study. PTC and FTC, although they differ in clinical behaviors, were analyzed together, and most recurrences were observed in patients with PTC. However, the same investigation was conducted only in the 130 patients with PTC and resulted in the same conclusions (data not shown). The clinical behavior of DTC in the pediatric population is reported to differ between the prepubertal and postpubertal periods (26,27). Aggressive disease and poor outcomes were observed in prepubertal DTC patients. However, because of the rarity of prepubertal DTC, it remains unclear whether younger children are at higher risk for recurrence than postpubertal adolescents (10). In this study, age was not a significant factor related to DFS, but only five patients were <10 years old, three of whom were categorized as high risk and two as low risk. The relationship between histological subclassification and DFS was not examined. Unlike in adult DTC, there is no consensus about the relationship between histological subtype and clinical outcomes in pediatric populations. In the study by Balachandar et al. (28), the authors concluded that, “unlike in the adult population, ‘high-risk’ histologic subtypes did not independently predict extent of disease at presentation or event-free survival in this pediatric population with DTC.” However, several studies reported a significant relationship between histological subtype and clinical outcomes (22,29). Another limitation is that NMLNs is usually proven after surgery. At present, no definite method to quantify NMLNs preoperatively is available. Thus, another analysis was performed after excluding NMLNs. Multivariate analysis showed that significant risk factors related to DFS were cN and ETE. Risk stratification was performed according to the number of risk factors. DFS was significantly different among these risk groups, and 10- and 20-year DFS rates of low-risk patients were 92.4% and 81.8%, respectively. Although this risk stratification resulted in an increase of low-risk group patients and a decrease of high-risk group patients, DFS in the low-risk group was almost equivalent to that of the low-risk group derived from the initial analysis including NMLNs. In the present study, the role or benefit of pCND for cN0 patients could not be clarified because we routinely perform prophylactic neck dissection (although the extent of dissection has changed) for all patients with a preoperative diagnosis of malignancy. In this series, 97 cN0 patients underwent pCND (including 67 patients with pMND), and MLNs at level VI were diagnosed histologically in 81 patients (83.5%). There was no significant difference in the node-positive patient ratio by the primary tumor size. Pathological lymph node metastasis is frequently observed at level VI, even in patients with small primary tumors. In our opinion, the main purpose of pCND is not only to reduce the possibility of recurrence at level VI, but also to reduce the possibility of damaging the recurrent laryngeal nerve at the time of lymph node recurrence at level VI.
In conclusion, compared with the risk stratification in the current ATA guidelines, our risk stratification is composed of more specific factors derived from patients who were treated mainly by lobectomy. Although total thyroidectomy was not performed in 88% of the low-risk group patients, excellent DFS was observed in low-risk pediatric DTC patients. A conservative therapeutic strategy may be acceptable for low-risk pediatric patients, as for adult low-risk DTC patients.
Authors Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.