
Abstract
Background:
Health insurance has been shown to be a key determinant in cancer care, but it is unknown as to what extent insurance status affects treatments provided to papillary thyroid cancer (PTC) patients. We hypothesized that insured patients with PTC would have lower-risk tumors at diagnosis and be more likely to receive adjuvant therapies at follow-up.
Methods:
The American College of Surgeons' National Cancer Database was queried to identify all patients diagnosed with PTCs >2 mm in size from 2004 to 2015. Patients were grouped according to insurance status, and frequency of high-risk features and microcarcinoma at diagnosis were assessed. Multivariable analyses were used to identify independent predictors of more extensive treatment: total thyroidectomy (vs. lobectomy), lymphadenectomy, and radioactive iodine (RAI).
Results:
There were 190,298 patients who met inclusion criteria; the majority of patients had private insurance (139,675 [73.4%]) and were female (144,824 [76.1%]). Uninsured patients, as compared with privately insured patients, had higher rates of extrathyroidal extension of their cancers (25.2% vs. 18.9%, p < 0.001), lymphovascular invasion (16.2% vs. 12.0%, p < 0.001), and positive margins on final pathology (16.0% vs. 12.2%, p < 0.001). Conversely, patients with private insurance were 51% more likely to have microcarcinomas at diagnosis (odds ratio [OR] = 1.51 [confidence interval {CI} 1.35–1.68], p < 0.001) than uninsured patients, controlling for demographic, socioeconomic, and hospital factors. Private insurance was an independent predictor for treatment with total thyroidectomy (OR = 1.18 [CI 1.01–1.37], p < 0.05), formal lymphadenectomy (OR = 1.22 [CI 1.09–1.36], p < 0.001), and adjuvant RAI therapy (OR = 1.35 [CI 1.18–1.54], p < 0.001) as compared with no insurance, adjusted for socioeconomic, demographic, hospital, and oncologic differences. Patients with Medicare or Medicaid were no more likely to receive these treatments than uninsured patients.
Conclusions:
Privately insured patients have less aggressive PTCs at diagnosis, and they are more likely to be treated with total thyroidectomy, lymphadenectomy, and RAI compared with uninsured patients. Clinicians should take caution to ensure proper referral and follow-up for under- and uninsured patients to reduce disparities in treatment.
Introduction
Papillary thyroid carcinoma (PTC) is the most common subtype of thyroid cancer, and its incidence has risen dramatically (1). These cancers are typically relatively indolent, yet can vary widely in aggressiveness, resulting in treatment strategies ranging from close observation to surgical and adjuvant therapies (2). Socioeconomic disparities have been shown to affect treatment and outcomes for patients with a variety of cancers, including PTC (3 –5). The American Thyroid Association (ATA) provides comprehensive guidelines for the management of patients with PTC (6); however, socioeconomically disadvantaged patients often receive care that deviates from these guidelines (7). Further, these disadvantaged patients often struggle to obtain and maintain health insurance (8). However, to date, the degree to which insurance status determines the extent of treatment for PTC patients is unclear.
Health insurance has a central role in enabling patients in the United States to both access and receive care (9,10). In addition to providing financial stability in the event of an illness, health insurance allows patients to better receive longitudinal care. Cancer patients, in particular, often need to be treated and followed for long periods, and thus may be particularly vulnerable to lapses in insurance coverage (11). In fact, a recent study by Ellis et al. (12) demonstrated that from 1997 to 2014, survival for Californian patients with prostate, lung, and colorectal cancers was lower for uninsured or publicly insured patients as compared with patients with private insurance. Perhaps most worrisome is that the disparity grew over the study period (12). Similarly, expansion of Medicaid in Kentucky improved early diagnosis and survival for patients with colon cancer (13).
In addition to affecting treatment access and survival for cancer patients after diagnosis, health insurance status has also been shown to correlate with cancer stage at diagnosis. Expansion of insurance coverage for young women following the Affordable Care Act resulted in increased likelihood of women being diagnosed with early-stage cervical cancer (14). This was not specific to cervical cancer; Medicaid expansion in 2014 resulted in an increased number of total cancer diagnoses in counties that expanded coverage, particularly of early-stage tumors (15). Importantly, this pattern may occur in thyroid cancer as well; Weeks et al. (16) showed that patients with private insurance were more likely to have less aggressive tumors at diagnosis. Similar studies have also documented discrepancies based on race/ethnicity and socioeconomic status in the care of PTC patients (7,17). However, these studies did not address the independent effect of insurance status on the treatment of patients with PTC.
PTC patients, in particular, may be especially vulnerable to insurance-based diagnostic and treatment disparities given the wide range of therapeutic options for this disease. We hypothesized that insured patients with PTC would have lower-risk tumors at diagnosis and be more likely to receive adjuvant therapies at follow-up.
Methods
This study was exempt from institutional board review due to the use of nationally available de-identified data. The American College of Surgeons' (ACS) National Cancer Database (NCDB) was queried to identify all patients with PTCs >2 mm treated from 2004 to 2015. The NCDB is a hospital-based cancer registry that currently includes patients treated at more than 1500 hospitals in the United States, comprising >70% of U.S. cancer patients (18). Diagnosis of PTC was determined by using International Classification of Diseases for Oncology, Third Edition (ICD-O-3) codes 8050/3, 8260/3, 8340/3, 8341/3, 8342/3, 8343/3, and 8344/3. Primary outcomes assessed were microcarcinoma at diagnosis, total thyroidectomy (vs. lobectomy), formal lymphadenectomy, and adjuvant radioactive iodine (RAI) treatment. Microcarcinomas were defined as tumors <1 cm on final pathology, with no preoperative clinical cervical lymphadenopathy (cN0 or cNX) or distant metastases (cM0 or cMX). Patients who did not undergo anatomic thyroid resection (lobectomy or greater) were excluded. Patient demographics, socioeconomic factors, and oncologic data were analyzed retrospectively. In the 2015 NCDB, income is represented as median income in each patient's primary zip code, at the time of diagnosis, derived from 2012 American Community Survey data. Similarly, a percentage of the population graduating from high school is derived from the same database and coded by patients' zip codes. All other variables used in these analyses are patient-level data. Patients were divided into four groups based on insurance status: Privately Insured, Medicare, Medicaid, and No Insurance. Other insurance types were excluded, as they represented primarily unique patient populations (e.g., military members).
In a separate analysis, Surveillance, Epidemiology, and End Results (SEER) and United States Census data were collected from the National Cancer Institute's website to determine state-by-state thyroid cancer incidence and the percentage of population in each state that was uninsured, respectively (19).
Descriptive statistics are reported as means and standard deviations for continuous, normally distributed data or median with interquartile range (IQR) for ordinal or nonparametric continuous data. Categorical variables are listed as number and percent. The NCDB has changed over time, and as a result some data were not available for the entire cohort; in these cases, the data presented represent only the available information, with the exception of clinical staging for microcarcinomas (as previously mentioned), M stage, lymphadenectomy, and RAI. Patients with unknown M staging were considered as not having distant metastases; likewise, patients with unknown lymphadenectomy or RAI status were considered as not undergoing each respective treatment. Patients staged as pNX were included as a distinct group, since lymphadenectomy is not always performed with thyroidectomy and thus these patients may be appropriately staged rather than representing missing or unknown data. Missing or unknown data for variables used in the multivariable logistic regression and Cox proportional hazards analyses are listed in Supplementary Table S4.
Pearson's chi-squared test was used to compare categorical variables, continuous normally distributed variables were tested by using t-tests, and nonparametric or ordinal variables were compared by using Wilcoxon rank-sum tests or Kruskal–Wallis tests. Multivariable logistic regressions, using cluster-robust standard errors clustered by hospital ID, were used to determine independent predictors of microcarcinoma at diagnosis, total thyroidectomy, lymphadenectomy, and RAI treatment. In these analyses, each hospital is considered a unique cluster of patients; therefore, variations in hospital volume or payor mix (or other hospital-level variables) are accounted for in the regression models. Multivariable Cox proportional hazards modeling, again using the same cluster-robust standard errors, was used to identify predictors of overall survival. All variables were treated as categorical with the exception of age, which was treated as a continuous variable in these regressions. Pearson R was used to measure correlation between state-by-state uninsured population (U.S. census data) and thyroid cancer incidence (SEER). Variance inflation factors (VIFs) were calculated for all variables used in the multivariable or Cox regressions to assess for multicollinearity; variables were excluded if VIF was >10 or tolerance was <0.5. No variables were found to be collinear using these criteria. All statistical analyses were performed by using Stata software, version 13.1 (StataCorp., College Station, TX).
It is acknowledged that the NCDB remains the full and exclusive copyrighted property of the ACS. The ACS is not responsible for any claims arising from works based on the original data, text, tables, or figures.
Results
There were 190,298 patients who met inclusion criteria, and the majority of patients had private insurance (139,675 [73.4%]). Most patients were female (144,824 [76.1%]), and the median age at diagnosis was 48 years (IQR 38–59). Privately insured patients were more likely to be white race/ethnicity, non-Hispanic, and from neighborhoods in the highest income quartile (Table 1). Patients with any type of insurance were more likely to be treated at a high-volume hospital than those without insurance (Table 1).
Demographics and Tumor Characteristics by Insurance Status
Data represent number and (percent), unless otherwise specified.
IQR, interquartile range.
Patients with private insurance were the least likely to have cancers with high-risk features at pathologic diagnosis. Compared with privately insured patients, a higher percentage of uninsured patients had extrathyroidal extension (micro or macroscopic) of their cancers (25.2% vs. 18.9%, p < 0.001), lymphovascular invasion (16.1% vs. 12.0%, p < 0.001), and positive margins on final pathology (16.1% vs. 12.2%, p < 0.001). Approximately twice the proportion of uninsured patients had distant metastases compared with privately insured patients (1.2% vs. 0.6%, p < 0.001) (Table 1). Notably, uninsured patients also had a higher prevalence of these aggressive features than patients with Medicaid. However, both Medicaid and Medicare patients had a higher prevalence of aggressive features than those with private insurance (Table 1).
Patients with private insurance, Medicare, or Medicaid were more likely to have a papillary microcarcinoma at diagnosis than those without insurance, adjusting for other socioeconomic, demographic, and hospital factors (Table 2). Similarly, in a separate analysis using SEER and United States Census data, a significant inverse correlation was noted between the percentage of 18–64 years old that were uninsured in each state and state-by-state incidence of all thyroid cancers (correlation coefficient −0.34, R 2 = 0.31, p < 0.001) (Fig. 1).

Percentage of uninsured patients (age 18–64 years) and thyroid cancer incidence (age <65 years, cases per 100,000) by state. Nevada was excluded due to lack of thyroid cancer incidence data (Pearson R correlation coefficient −0.34, R 2 = 0.31, p < 0.001).
Clustered Multivariable Regression Identifies Independent Predictors of Microcarcinoma at Diagnosis
CI, confidence interval.
Privately insured patients were also more likely to receive more extensive treatments for their cancers on a stage-by-stage basis. At each American Joint Committee on Cancer (AJCC) stage, the proportion of privately insured patients undergoing lymphadenectomy and receiving adjuvant RAI treatment was higher than those without insurance (Fig. 2). This same pattern occurred when comparing patients with Medicare or Medicaid to those with private insurance.
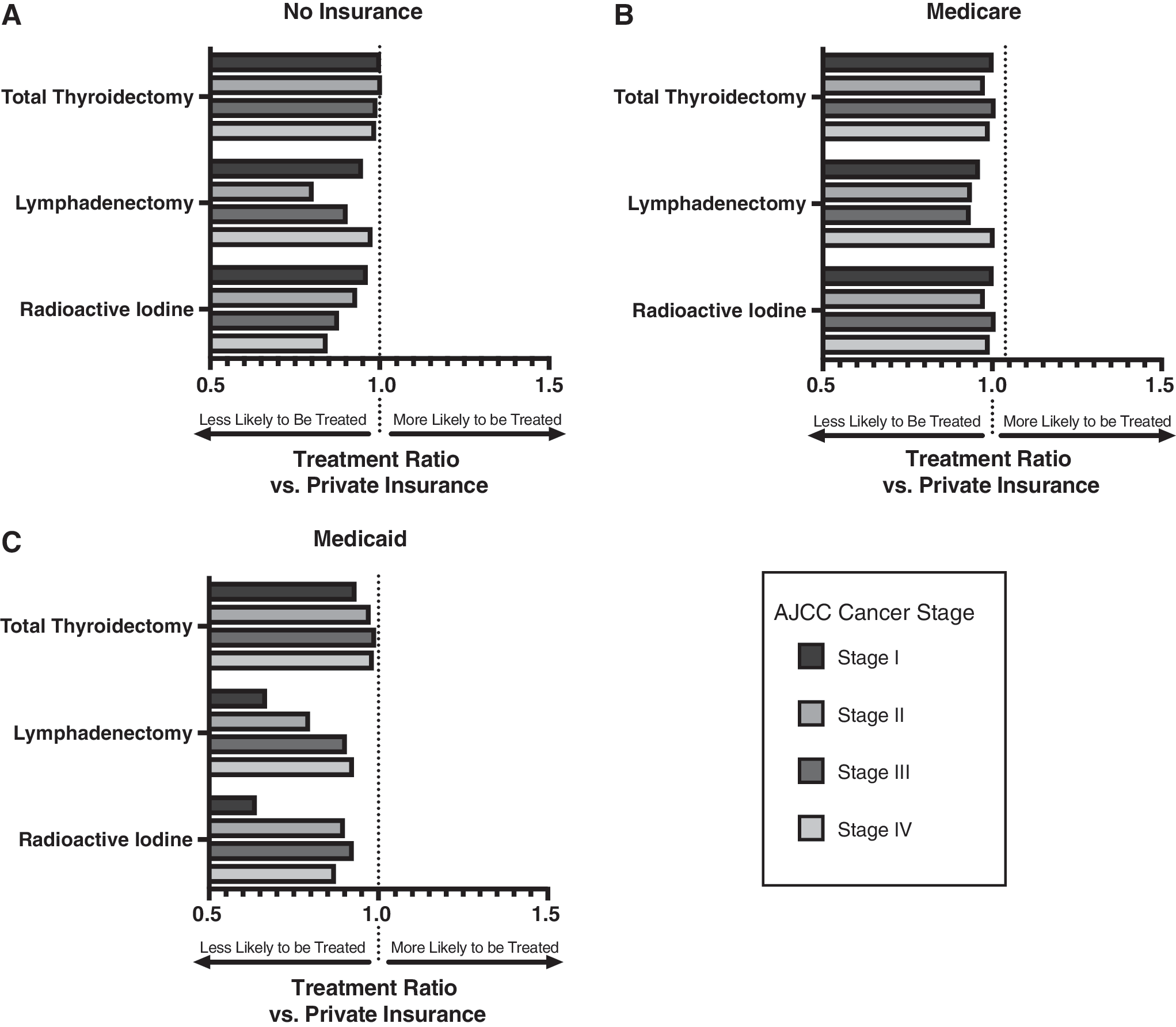
Ratio of percentage of patients with no insurance (
Multivariable regressions clustered by hospital and adjusted for socioeconomic (local household income quartile, local educational attainment), demographic (race/ethnicity, age, sex, Hispanic ethnicity), facility (via clustering by hospital), and oncologic (pathologic T, N, and M stages) differences showed that private insurance was an independent predictor for treatment with total thyroidectomy (odds ratio [OR] = 1.18 [confidence interval {CI} 1.01–1.37], p < 0.05), formal lymphadenectomy (OR = 1.22 [CI 1.09–1.36], p < 0.001), and adjuvant RAI therapy (OR = 1.35 [CI 1.18–1.54], p < 0.001) (Fig. 3 and Supplementary Tables S1, S2, S3). Importantly, Medicaid and Medicare patients were no more likely to undergo any of these treatments than uninsured patients. Cox proportional hazards ratio, adjusted for these same variables, with the additions of Charlson–Deyo comorbidity index, positive margins after resection (gross or microscopic), and tumor multifocality, demonstrated that total thyroidectomy and RAI treatments had a survival advantage, and patients with lymph node metastases had a survival disadvantage. Patients with private insurance also had a survival advantage compared with those without insurance, while patients with Medicaid were at a disadvantage (Table 3).

Odds ratios (symbols) and confidence intervals (lines) for receiving each treatment by insurance status, relative to uninsured. Graphs represent the results of multivariable analyses adjusted for demographic, socioeconomic, and oncologic variables listed in Supplementary Tables S1, ve to uninsured. Graphs represent the results of multivariable analyses adjusted for demographic, socioeconomic, and oncologic variables listed in S2, ve to uninsured. Graphs represent the results of multivariable analyses adjusted for demographic, socioeconomic, and oncologic variables listed in S3.
Clustered Cox Proportional Hazards Model Identifies Independent Predictors of Overall Survival Among Patients Who Underwent Anatomic Thyroidectomy for Papillary Thyroid Cancer
pN1 not otherwise specified in the National Cancer Database.
HR, hazard ratio.
Discussion
This study is the first to demonstrate that insurance status independently affects treatments provided to PTC patients. In addition, in agreement with previous reports, we found that privately insured patients had lower-risk cancers at diagnosis (16), as illustrated by the disparity in the presence of high-risk features at diagnosis and the odds of microcarcinoma at diagnosis. Papillary thyroid microcarcinomas are indolent cancers, and in response to recent data showing that the increase in thyroid cancer incidence was largely attributable to a rise in these small, low-risk tumors, the most recent ATA guidelines recommend consideration of observation alone for these patients (6). These tumors have been used as a surrogate marker for over-screening and over-diagnosis of thyroid cancers (20 –22). Therefore, this pattern suggests that insured patients are over-diagnosed with low-risk PTCs.
Importantly, insured patients are not only more likely to be diagnosed with a low-risk tumor, but they have also been shown to be more likely to be diagnosed with thyroid cancer overall. Altekruse et al. (23) analyzed the SEER database and found that higher socioeconomic status and insurance status were associated with higher incidence of thyroid cancer. Other studies have found that thyroid cancer incidence correlates with insurance rates and access to care (16,24 –26). Similarly, we have documented an inverse correlation between the state-by-state percentage of uninsured residents and the overall thyroid cancer incidence on a national level. Our analysis of statewide insurance rates and thyroid cancer incidence, therefore, adds to the growing body of evidence, supporting a connection between insurance status and thyroid cancer incidence.
In addition, we have demonstrated that thyroid cancer patients with private insurance undergo more extensive treatments than their uninsured counterparts, adjusting for demographic, socioeconomic, and oncologic characteristics. Notably, there are also disparities in treatment by stage; a higher proportion of privately insured patients underwent lymphadenectomy and RAI at each AJCC stage than uninsured, Medicare, or Medicaid patients (Fig. 2). In fact, the disparity in adjuvant RAI treatment widened with increasing cancer stage for patients without insurance, but it decreased with increasing stage for those patients with Medicaid. This is concerning, because it is possible that the highest risk patients (those with stage IV disease) have the highest disparity in adjuvant treatment. In contrast, when stratified by stage, there was little difference in the proportion of patients undergoing total thyroidectomy between the private insurance, Medicare, Medicaid, and no insurance groups.
Cox proportional hazards modeling demonstrated that there was a survival advantage for RAI treatment, and patients with nodal metastases had worse overall survival, suggesting that lymphadenectomy may be of benefit for staging purposes. This is in agreement with an analysis done by Adam et al. (27). In contrast, we found that total thyroidectomy did confer a slight survival advantage (hazard ratio = 0.91 [CI 0.84–0.99], p = 0.03). However, we did not exclude patients with tumors >4 cm in size, or those with the more aggressive tall cell or columnar variants, which likely explains this discrepancy. Therefore, privately insured patients may have benefited from more frequent treatment with total thyroidectomy, lymphadenectomy, and RAI. Privately insured patients also had a survival advantage relative to those without insurance, while those with Medicaid were at a disadvantage (Table 3).
Similarly, the largest disparities in stage-by-stage care appear between those patients with private insurance and those with Medicaid, rather than no insurance. This pattern may be multifactorial, potentially due in part to heterogeneity in the no insurance group. It is possible that some patients in the no insurance group were, in fact, privately paying patients who chose “out-of-network” or concierge physicians rather than paying through insurance. This hypothesis is supported by the fact that there is a higher percentage of patients from socioeconomically advantaged neighborhoods in the no insurance group (Table 1). Further, there are more minority patients in the Medicaid group, which may exacerbate insurance-based differences in care, as race/ethnicity has been shown to be a determinate of care (Table 1). Finally, there are likely differences between physicians and hospitals treating patients with no insurance versus those accepting Medicaid patients, although we have attempted to control for hospital-level discrepancies by using clustered analyses.
There are several possible sources for the disparities in cancer care for PTC patients documented here. One possibility is that clinicians are offering different treatment strategies to their patients based on their insurance provider, or that physicians who do not accept Medicare, Medicaid, or uninsured patients have different treatment patterns than those that do. Alternatively, patients with different insurance types may have differing treatment goals or desires and thus be inclined to make different choices regarding their care. There are also data to suggest that clinicians may treat PTC patients differently based on their fear of litigation (28). Insurance status may affect how often patients are referred to other specialists, for example from surgeons to nuclear medicine specialists for RAI. The availability of many of these specialists is likely also affected by the insurance coverage that they will accept. Uninsured or underinsured patients may also be at higher risk for loss to follow-up, which is critical for adjuvant treatments such as RAI. Perhaps the most likely scenario is that the disparities documented here result from a combination of all of these factors.
There are several limitations to this study. First, it is retrospective, so causal relationships between variables cannot be determined. In addition, as with all large database studies, the conclusions are dependent on the accuracy of the data entered. Complete data are not available for all patients, and in particular preoperative staging information was inconsistent, necessitating, for example, that the definition of “microcarcinoma” includes patients with cNX and cMX disease. All patients with unknown metastatic staging were considered as not having metastases, so some may have incorrectly been considered as M0. This missing data may bias the results, however >90% of data were available for the majority of variables used in our analyses (Supplementary Table S4). We excluded patients who did not undergo anatomic surgical resection, and therefore there were no patients managed with observation for microcarcinomas in the study cohort. This may have biased our results if these patients were predominantly privately insured, for example, resulting in an underestimation of the association between private insurance and microcarcinoma at diagnosis. Education and income data are only available at the zip-code level, so they do not provide patient-level granularity, and therefore they may not be representative of each individual patient's socioeconomic status. Finally, the NCDB includes only thyroid cancer patients with pathologically confirmed cancer diagnoses; thus, some patients may have had cancers that were diagnosed only postoperatively after surgery for indeterminate nodules or other indications, for example, Graves' disease.
In conclusion, thyroid cancer incidence in the United States is correlated with insurance coverage on a state-by-state basis, and insured patients are more likely to be diagnosed with lower-risk PTCs and papillary thyroid microcarcinomas. Privately insured patients are also more likely to be treated with total thyroidectomy, lymphadenectomy, and adjuvant RAI than uninsured patients. Clinicians should be mindful of these disparities when considering appropriate treatments, and they should take caution to ensure proper referral and follow-up for uninsured and underinsured patients. Further research is needed to identify factors driving these disparities in treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded directly by the Weill Cornell Department of Surgery.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4