
Abstract
Background:
Cribriform–morular variant of papillary thyroid carcinoma (CMV–PTC) is a rare subtype of PTC, which occurrs predominantly in young women. This disease much more frequently presents in patients with familial adenomatous polyposis (FAP). FAP is an autosomal dominant inherited disease, which arises from germline mutations in the adenomatous polyposis coli (APC) gene. To clarify the distinctive clinical features of CMV–PTC, a comparison study was performed between familial types and sporadic types.
Methods:
Between 2007 and 2018, 15 CMV–PTC patients underwent thyroidectomy in Samsung Medical Center. The clinical features of these patients were retrospectively reviewed.
Results:
All patients were women with a median age of 26 years (range 17–46 years). The median maximum diameter was 1.0 cm (range 0.4–3.5 cm). All tumors underwent immunostaining and showed nuclear and/or cytoplasmic staining for β-catenin. On ultrasonography, most nodules had benign-looking features (well-defined, hypoechoic, and oval to round shapes without calcification), but a few nodules had capsular invasion and taller than wide shape. On preoperative fine-needle aspiration cytology, five patients (33%) were diagnosed as CMV–PTC, nine (60%) as PTC, but one (7%) as follicular neoplasm or PTC–follicular variant. Six patients (40%) had FAP, and four of them had total colectomy due to FAP. Five of them had a family history of FAP or colon cancer, or thyroid cancer. Germline mutations in the APC gene were found in all six patients with CMV–PTC associated with FAP, and five of them had de novo mutations. All patients with FAP-associated CMV–PTC had multiple tumors. All CMV–PTC patients had excellent response to initial therapy.
Conclusions:
Because of the association between FAP or colon cancer with multifocal CMV–PTC, we confirm that mutational analysis of the APC gene and colonoscopy should be carried out in these patients when multiple thyroid tumors are found.
Introduction
The cribriform–morular variant of papillary thyroid carcinoma (CMV–PTC) is a rare subtype of PTC that is histologically characterized by distinctive cribriform, follicular, papillary, trabecular, solid, and epithelial morular pattern (1). It is well known that CMV–PTC much more frequently presents in patients with familial adenomatous polyposis (FAP) but it can also occur as sporadic disease (2,3). FAP is an autosomal dominant inherited disease, characterized by the development of multiple colorectal polyps that develop due to germline mutations of the adenomatous polyposis coli (APC) gene, although up to 25% of all FAP cases occur de novo (4). PTC is one of the well-known extracolonic manifestations affecting ∼1–2% of FAP patients (5,6).
APC is a tumor suppressor gene located on chromosome 5q21–22. APC is a multiprotein complex including an oligomerization domain, an armadillo repeat domain, a 15- or 20-residue repeat domain, an SAMP repeats domain, a basic domain, and C-terminal domains (7). Most mutations are frameshift or nonsense variants leading to a truncated protein (5,8). The majority of APC germline mutations occur in the 5′ half of the gene, leading to lack of the 20-amino acid repeat domain that is required for binding to β-catenin (5,9). As a result, β-catenin accumulates in the nucleus and cytoplasm because the normal APC protein leads to degradation of β-catenin oncoprotein (6). CMV–PTC is not only associated with germline APC mutations, but can also develop secondary to somatic mutations in the APC gene and components that regulate β-catenin turnover (10,11). The accumulation of β-catenin is the hallmark of CMV–PTC in both familial and sporadic cases (12,13).
Many researchers have reported the relationship between PTC and FAP in FAP patients or thyroid cancer patient registries (6,14). However, the nature of CMV–PTC with regard to patient FAP status has not been well characterized due to the extremely low prevalence of CMV–PTC. The aim of this study was to investigate the unique features of FAP-associated CMV–PTC by comparison with cases without FAP.
Materials and Methods
Patients
A retrospective review was performed on 15 CMV–PTC patients who had undergone thyroidectomy at Samsung Medical Center between 2007 and 2018. Diagnoses were confirmed histopathologically with surgical specimens. The patients comprised six FAP-associated CMV–PTC cases and nine sporadic CMV–PTC cases, defined by family history, colonoscopy, and genetic analysis. In case 3, the patient's father and older sister had FAP, and two paternal aunts had colon cancer. Case 4 had two family members affected by FAP: her father underwent prophylactic total colectomy due to FAP, and her older sister had FAP and PTC. In case 10, the patient's mother had thyroid cancer with FAP, and a maternal uncle had colon cancer. In case 12, the patient's father had died of colon cancer. Case 13 had a father with colon cancer and a younger brother with FAP. Case 14 had no family history of FAP or colon cancer. All 15 patients underwent colonoscopy. Cases 3, 4, 10, 12, and 14 showed hundreds of colon adenomas, and 15 adenomas were shown in case 13. Cases 4 and 13 had been undergoing colonoscopic polypectomy annually. Cases 3, 10, 12, and 14 had undergone total colectomy. Clinical information was obtained from medical records.
This study was approved by the Institutional Review Board. Nine patients underwent mutational analysis for APC germline mutations, and informed consent was obtained for the genetic study.
Ultrasonographic thyroid screening and fine needle aspiration
All 15 patients underwent ultrasonographic examination of the thyroid gland. A retrospective review of ultrasonography (US) images and US characteristics of tumors determined by radiologists was performed. US-guided fine needle aspiration (US-FNA) and cytological examination were also performed by experienced radiologists. Aspirates were spread on frosted-end glass slides and then immediately fixed in 95% ethanol and stained with hematoxylin and eosin and Papanicolaou staining. Final results were determined based on cytology and pathology reports.
Immunohistochemistry
Immunohistochemistry for β-catenin was performed using a mouse monoclonal antibody (224M-16, dilution 1:200; Cell marque, Rocklin, CA) in a BenchMark XT (Roche/Ventana Medical Systems, Tucson, AZ) according to the manufacturer's instructions.
Genetic analysis
Mutational analysis for germline mutations in the APC gene was performed in nine patients by sequencing DNA obtained from peripheral blood leukocytes. Patients with a family history of FAP or colon cancer were included. Genomic DNA was extracted from EDTA-anticoagulated whole blood using the Wizard® Genomic DNA Purification Kit according to the manufacturer's instructions (Promega, Madison, WI). Entire coding exons and intron-exon junctions were amplified by PCR using primer pairs designed with Primer3 software. The primers are available upon request. Direct sequencing was conducted using a BigDye Terminator Cycle Sequencing Ready Reaction Kit (Applied Biosystems, Foster City, CA) and an ABI Prism 3100 Genetic Analyzer (Applied Biosystems). Variant interpretation was done according to the American College of Medical Genetics and Genomics guidelines.
Statistical analysis
Statistical analyses were performed with Mann–Whitney using SPSS (version 25.0; IBM Corp., Armonk, NY). A p-value ≤0.05 was considered statistically significant.
Results
Clinical features of patients with CMV–PTC
The median age of the 15 patients with CMV–PTC was 26 years (range 17–46 years) at the time of diagnosis. All CMV–PTC patients were women. Tumors were solitary located in the right lobe (n = 5), left lobe (n = 4), or multifocal (more than three tumors) in both lobes (n = 6). Median tumor size was 1.0 cm with a range from 0.4 to 3.5 cm. On US, most had benign-looking features: well defined, oval to round, hypoechoic, and solid without calcification. Some tumors showed internal cystic changes (Fig. 1). Only two tumors had capsular invasion or taller-than-wide shape. US–FNA was performed for all patients. Only five patients were diagnosed with CMV–PTC by FNA—the remainder were reported as classical PTC or follicular neoplasm versus follicular variant of PTC (Table 1). This suggests that a precise diagnosis of CMV–PTC by US and US–FNA is difficult.
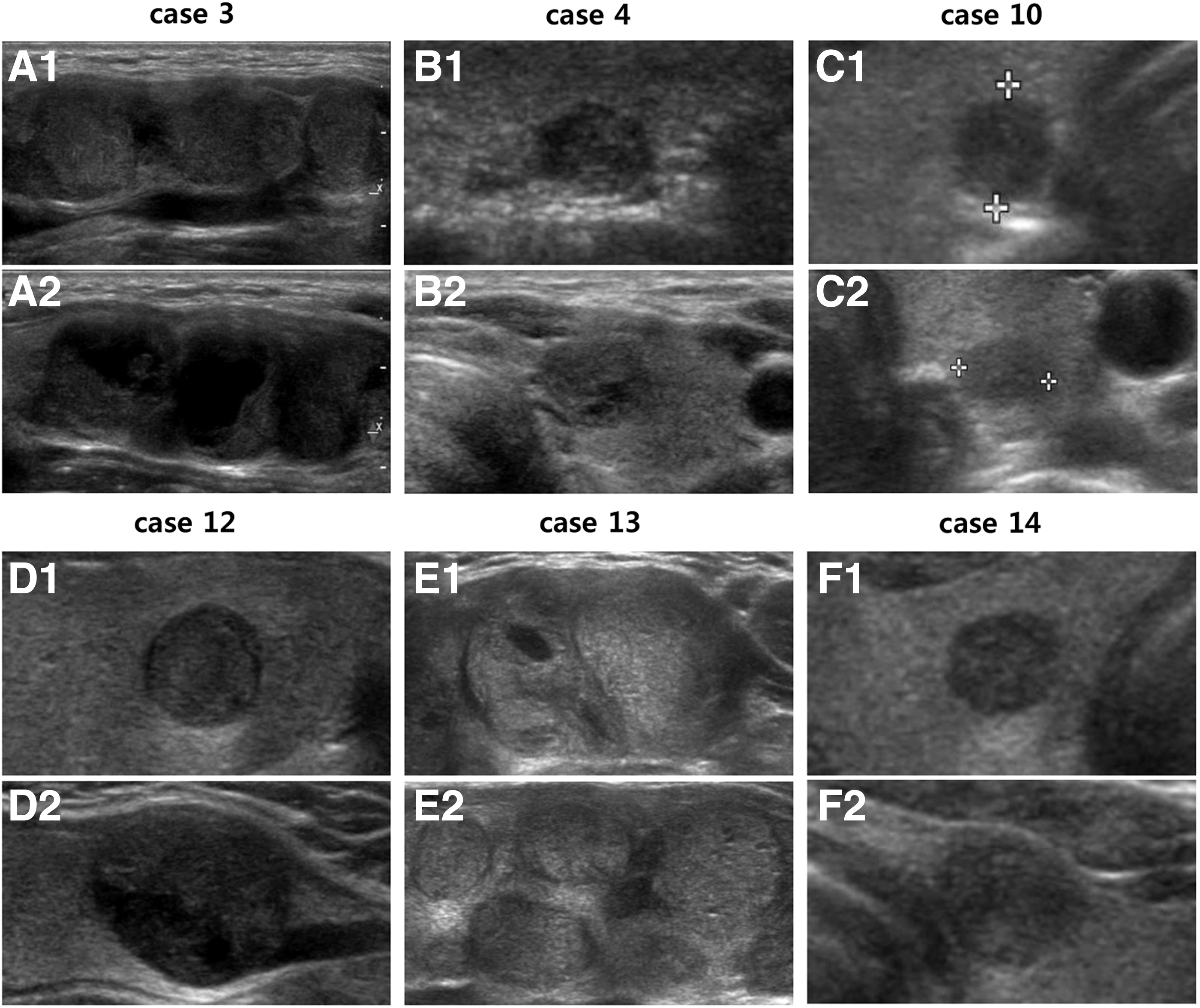
Ultrasonograms of thyroid glands of CMV–PTC patients with FAP. All patients with FAP-associated CMV–PTC presented with multiple tumors. Longitudinal sonograms in the right (
Preoperative Ultrasonography and Fine-Needle Aspiration Findings of the Patients with Cribriform–Morular Variant of Papillary Thyroid Carcinoma
Bi, bilateral; CMV–PTC, cribriform–morular variant of papillary thyroid carcinoma; F, female; FN, follicular neoplasm; FNA, fine-needle aspiration; Lt, left; PTC, papillary thyroid carcinoma; PTC–FV, papillary thyroid carcinoma–follicular variant; Rt, right; US, ultrasonography.
All patients underwent hemithyroidectomy (n = 5) or total thyroidectomy (n = 10) with or without central neck dissection. Minimal lymphatic invasion and extrathyroidal invasion were found in one and two patients, respectively. No lymph node metastases was detected. The tumors were well demarcated, and showed predominately cribriform and follicular patterns formed by morules containing cells with peculiar nuclear clearing. Immunohistochemistry for β-catenin was performed in 12 of the 15 patients. β-catenin was positive in the nucleus and/or cytoplasm in all cases tested (Fig. 2). Eight patients underwent radioactive iodine therapy after thyroidal surgery, and all 15 patients showed complete remission (Table 2).
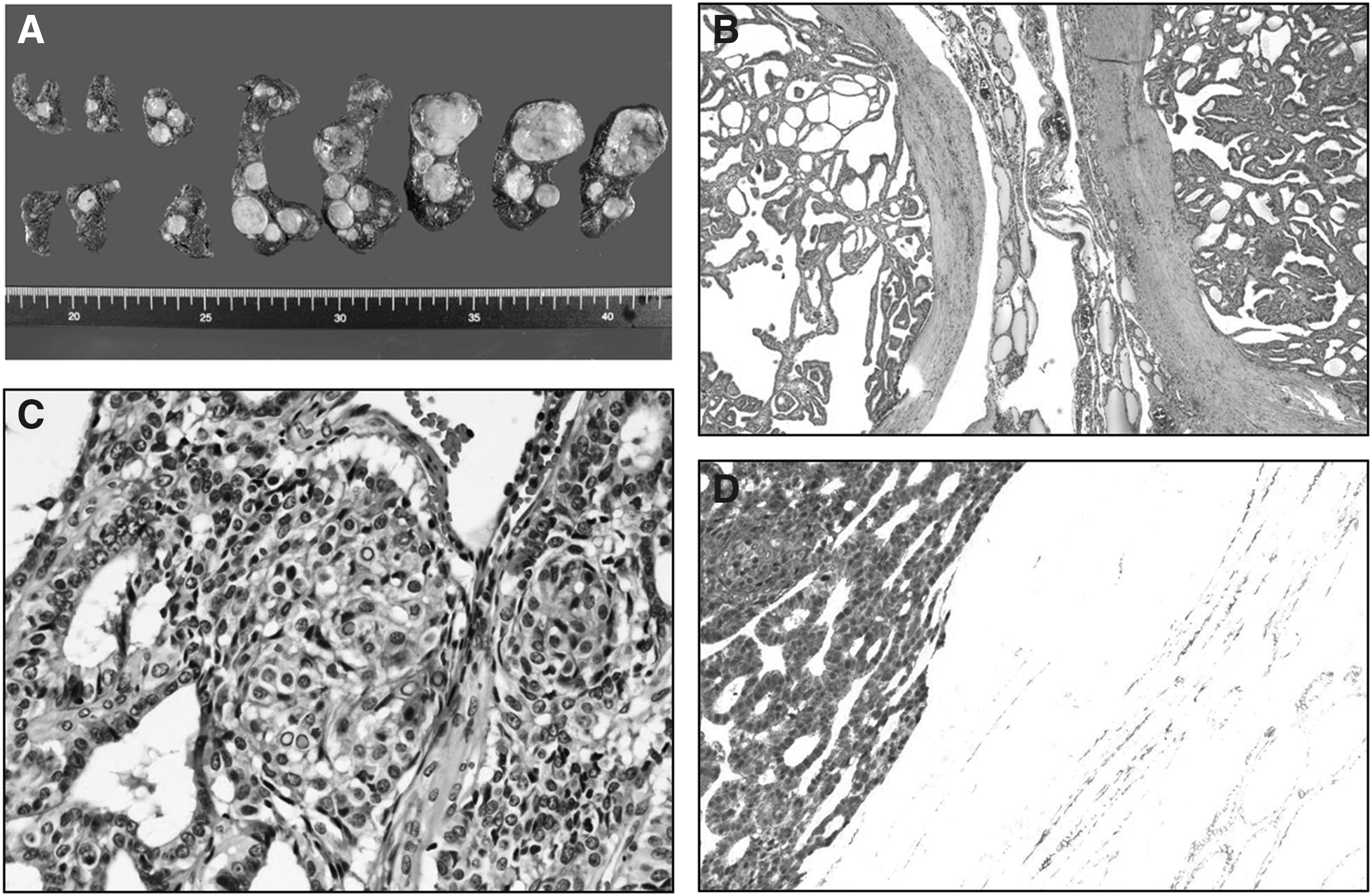
Gross and histopathological findings of thyroid tumors in case 13. (
Postoperative Histopathological Findings and Clinical Outcomes of the Patients with Cribriform–Morular Variant of Papillary Thyroid Carcinoma
Case 1 underwent a two-stage operation: first, left hemithyroidectomy then right hemithyroidectomy after pathological confirmation.
CND, central neck dissection; ETI, extrathyroidal invasion minimal; F, female; hemi, hemithyroidectomy; ND, not done; RAI, radioactive iodine; total, total thyroidectomy.
Comparison of FAP-associated CMV–PTC with nonassociated CMV–PTC
Among the 15 patients with CMV–PTC, 6 (40%) were FAP associated, and 9 were sporadic. The median ages of the groups were 25.5 and 28.0 years, and the median tumor sizes were 1.15 and 1.0 cm, respectively. There were no significant differences in age, tumor size, US findings, and clinical outcomes between FAP-associated and sporadic patients. By US criteria, most lesions in both groups had benign-looking features, and only 3 (50%) and 2 (22%) patients were diagnosed with CMV–PTC by FNA, respectively. However, all patients with FAP-associated CMV–PTC had multifocal tumors, while all patients with sporadic CMV–PTC had a solitary tumor. All patients demonstrated expression of β-catenin and excellent response to initial therapy irrespective of FAP status (Table 3). As a result, unless taking a personal/family history or undergoing a germline APC gene mutation test, there was no distinct clinical difference except tumor multifocality in patients with FAP-associated CMV–PTC compared with sporadic CMV–PTC.
Characteristics of the Patients with Familial Adenomatous Polyposis-Associated and Sporadic Cribriform–Morular Variant of Papillary Thyroid Carcinoma
One capsular invasion and one taller-than-wide sign. Age and tumor size are expressed as median (IQR).
APC, adenomatous polyposis coli; FAP, familial adenomatous polyposis; n, number of patients.
FAP-associated CMV–PTC and APC gene mutation
Germline APC gene mutation analysis was performed in nine patients. Mutations of APC gene were found in all six patients with CMV–PTC associated with FAP. Four underwent total colectomy—three for prophylaxis and one for colon cancer therapy. Five had a family history of FAP or colon cancer, while one showed sporadic FAP. Five of the CMV–PTC patients who were diagnosed with FAP or colon cancer presented with multiple thyroid tumors before the colonic manifestations, while case 14 was first diagnosed with FAP and CMV–PTC was detected five years later (Fig. 3). Interestingly, case 15 patient had three primary malignancies (breast cancer, colon cancer, and CMV–PTC), but she did not have a family history or an APC germline mutation.
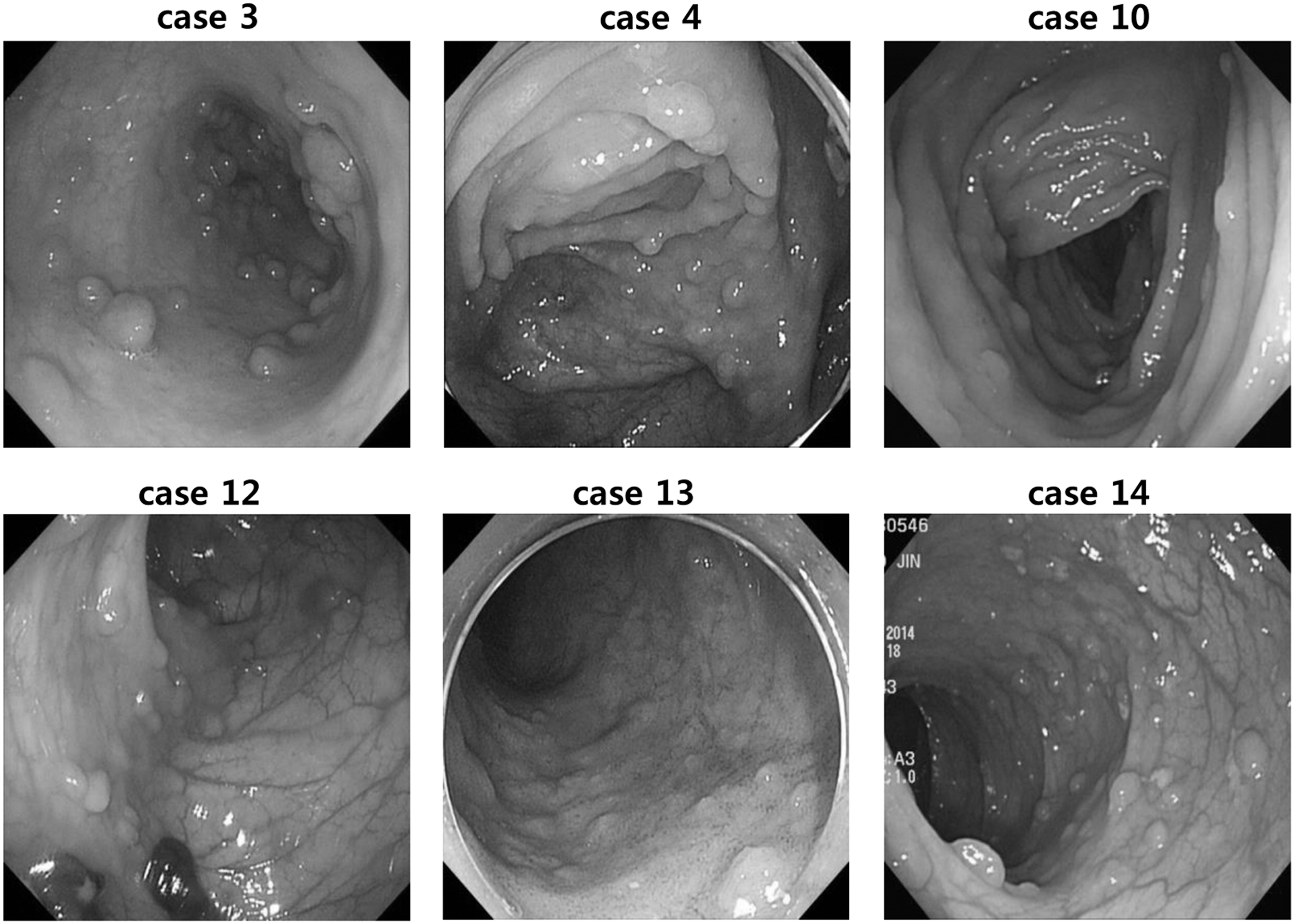
Colonoscopic findings of CMV–PTC patients with multiple thyroid tumors. All six patients presented hundreds of colon polyps.
All germline APC mutations were truncating mutations leading to premature terminations, mainly due to frameshifts or nonsense variants. Only one (codon 1062, case 3) mutation was a well-known pathological germline mutation of the APC gene, the others were novel mutations not previously reported in the human genome mutation database (Fig. 4). Only one (codon 1394, case 13) of these germline mutations was in the mutation cluster region (codon 1286–1514). The specific mutations are given in Table 4.
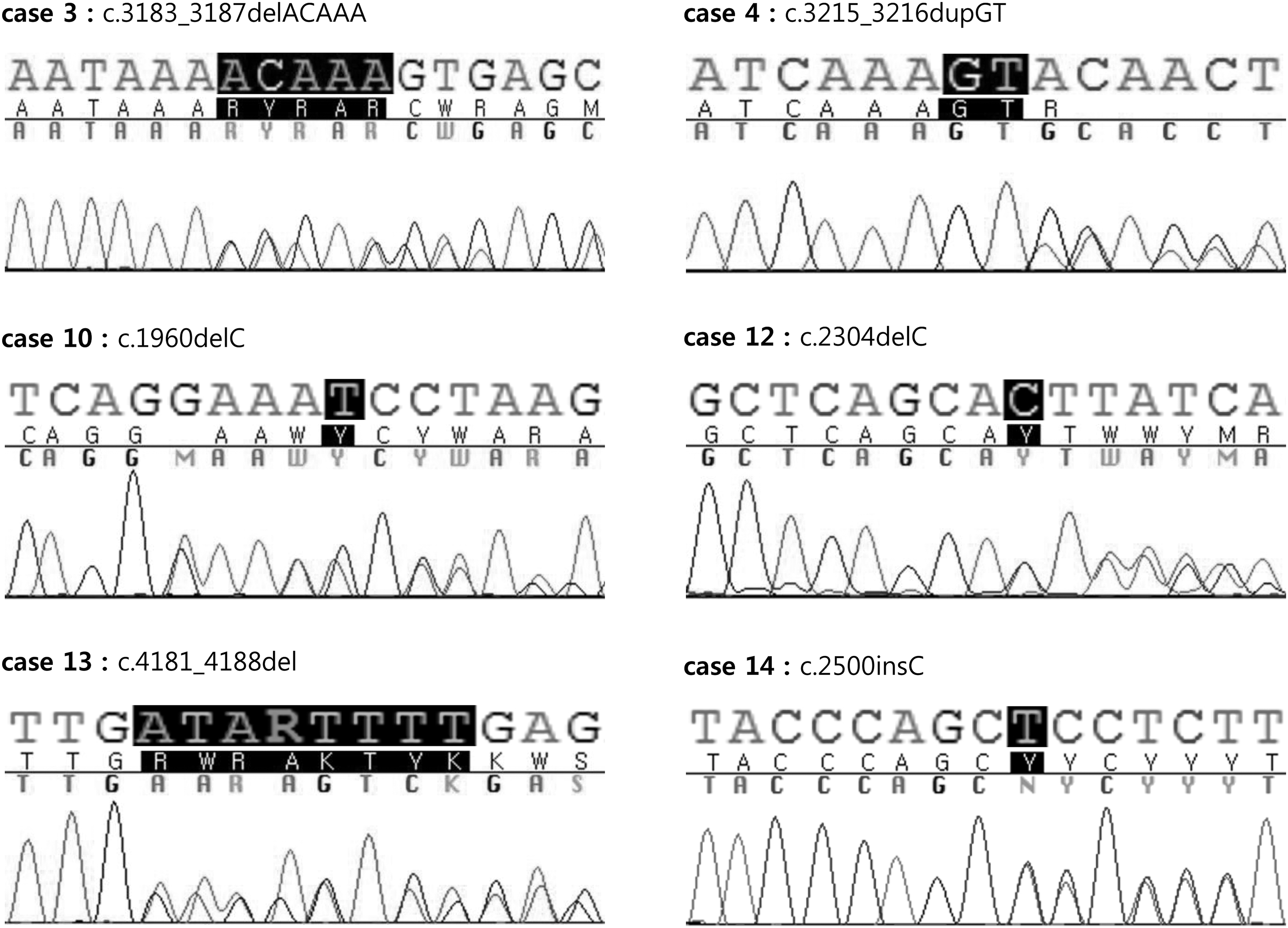
Sequence analysis of the APC gene from six FAP-associated CMV–PTC patients, showing germline mutations. One known pathologic mutation (case 3) and the other de novo mutations are presented. APC, adenomatous polyposis coli.
Pathological Germline Mutations of APC Gene in the Patients with Familial Adenomatous Polyposis-Associated Cribriform–Morular Variant of Papillary Thyroid Carcinoma
Family history of colon cancer or FAP.
AA, amino acid; Asp, aspartic acid; d/t, due to; del, deletion; dup, duplication; Gln, glutamine; Gly, glycine; Het, heterozygous; ins, insertion; Leu, leucine; Lys, lysine; NT, nucleotide; Ser, serine; TC, total colectomy; Thr, threonine; Tyr, tyrosine; Val, valine.
Discussion
CMV–PTC is extremely rare, accounting for ∼0.16% of all thyroid cancers and 0.2% of all PTCs (1,2,10,15). Many researchers have published case reports of CMV–PTC or reported on its relationship with FAP, but the number of included patients is typically very small with usually <10 patients with CMV–PTC (14 –20). Because of its rarity, CMV–PTC characteristics have not been clearly established. There are two types of CMV–PTC, the FAP-associated type and sporadic type (10). However, not much research has been conducted comparing the two types. We have summarized the clinical features of patients with FAP-associated or sporadic CMV–PTC reported in the previous English literature, based on reports that had at least five or more CMV–PTC cases given in Table 5 (2,6,11,20 –24).
Clinical Summary of the Patients with Familial Adenomatous Polyposis-Associated and Sporadic Cribriform–Morular Variant of Papillary Thyroid Carcinoma Reported in Previous Studies
n, total number of patients; F, female.
In the previous studies, ∼50–60% of the patients with CMV–PTC were FAP-associated cases (10,15), and those patients represented 40% in the present study sample. There were no significant differences in age, sex, US, and FNA findings, and clinical outcomes between the FAP-associated and sporadic CMV–PTC groups except number of tumors. In this study, all patients with multifocal tumors were found to be FAP associated. This finding may be an important clue for the diagnosis of FAP in patients with CMV–PTC.
All patients with FAP-associated CMV–PTC had germline APC mutations. Among various germline APC mutations, codons 1309 and 1061 are well-known mutational hotspots for thyroid cancer and other extracolonic manifestations of FAP (25,26). More than 90% of APC mutations generate premature stop codons, resulting in stable truncated APC proteins rather than a complete loss of the protein. Up to 60% of mutations occur within codons 1286–1514, which is referred to as the mutation cluster region (27). However, in our cohort, only one (case 13) mutation was located in the mutation cluster region, while the other five mutations were found proximal to the mutation cluster region.
The majority of germline APC mutations are in the 5′ half of the gene. The C-terminally truncated proteins are missing a 20-amino acid repeat domain that is required for binding β-catenin and, therefore, the truncated APC protein cannot contribute to degradation of β-catenin (28,29). As a result, β-catenin accumulates in the cytoplasm and nucleus, leading to activation of the Wnt/β-catenin pathway (7). Therefore, even if not registered in the database, every mutation that produces a premature truncated protein can be a pathological variant. In fact, there are 4449 pathogenic APC gene mutations reported among total 5157 public variants in the Leiden Open Variation Database. This study identified five novel germline APC mutations, and all were truncating mutations. Interestingly, patients with non-FAP-associated CMV–PTC also demonstrated strong β-catenin expression on immunohistochemistry even though they did not have germline APC mutations. This suggests that somatic mutations of APC gene or mutations of the β-catenin gene (CTNNB1) itself might be related to development of CMV–PTC (11). Indeed, overall 30% of CMV–PTC cases showed somatic mutations of the APC gene, and 50% of patients with FAP also had somatic APC mutations (10). β-catenin was diffusely detected in all CMV–PTC tumor cells, with especially strong nuclear accumulation, whereas staining limited to the membrane or the cytoplasm (similar to normal thyroid tissue) has been reported in classical PTC (6). Because many cytological features overlap between CMV–PTC and classical PTC, the accumulation of β-catenin is a hallmark feature that can be helpful to diagnose CMV–PTC in both FAP-associated and nonassociated cases (10).
The female-to-male ratio of PTC is 3 to 4:1 (30), but CMV–PTC much more dominantly occurs in females (almost 99%), and tumor cells of CMV–PTC are always positive for estrogen and progesterone receptors (6,10). This suggests that hormonal factors such as estrogen and/or progesterone may be involved in the development of CMV–PTC, and further study is needed to clarify its mechanism (10).
In conclusion, we performed a comparison study between six FAP-associated CMV–PTCs and nine sporadic CMV–PTCs. There were no significant differences except the finding of multifocal tumors in FAP-associated cases, while all sporadic cases had a single tumor. When CMV–PTC is diagnosed in clinical practice, it is difficult to routinely perform APC mutation testing because of the low availability and high cost. Therefore, the diagnosis of CMV–PTC requires a well-trained thyroid pathologist because these tumors are often mistaken for other PTCs such as columnar PTC. This misclassification can have dire consequences since the diagnosis of FAP can be delayed. In family history, as case 13 of the present series, clinicians should consider performing screening colonoscopy in all patients diagnosed with CMV–PTC especially if they have multiple tumors.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No competing financial interests exist.