
Abstract
Background:
The 2017 World Health Organization (WHO) Classification of Tumors of Endocrine Organs defines poorly differentiated thyroid carcinoma (PDTC) as a tumor with conventional criteria of malignancy (capsular penetration or vascular invasion) with solid, insular, or trabecular growth, a lack of nuclear features of papillary thyroid carcinoma, and increased mitotic activity, tumor necrosis, or convoluted nuclei. The extent of invasion has been shown to be prognostic in follicular thyroid carcinoma and Hürthle cell carcinoma. Our aim was to evaluate how extent of invasion impacts clinical outcome for PDTC.
Methods:
We retrospectively identified 47 consecutively diagnosed cases of PDTC that were resected between 2005 and 2018. All cases were reviewed to confirm that the tumors met the 2017 Endocrine WHO criteria of PDTC. In addition, tumors were categorized as follows: encapsulated with capsular penetration only, encapsulated with focal vascular invasion (fewer than four foci), encapsulated with extensive vascular invasion (four or more foci), or widely invasive. Histopathologic characteristics and clinical outcome data were recorded.
Results:
A total of 47 cases of PDTC, including 15 oncocytic tumors, were identified from 28 (60%) women and 19 (40%) men (mean age of 57 years at diagnosis). The mean tumor size was 4.3 cm. Mitoses numbered 8 per 10 high-power fields (HPF) on average (range: 1–34), and necrosis was present in 21 (45%) cases. Eight (17%) cases were encapsulated with capsular penetration only, 5 (11%) were encapsulated with focal vascular invasion, 18 (38%) were encapsulated with extensive vascular invasion, and 16 (34%) were widely invasive. Of the 42 (89%) patients with follow-up data, 7 (17%) died of disease (with a mean survival time of 6.4 years), 11 (26%) have distant metastatic disease, and 24 (57%) have no evidence of disease (mean follow-up 5.6 years). Eight (19%) patients presented with M1 disease at diagnosis. The 5-year disease-free survival (DFS) for patients with M0 disease at diagnosis was 100% for patients with tumors with capsular invasion only or focal vascular invasion (n = 7), 73% for patients with encapsulated tumors with extensive vascular invasion (n = 11), and 17% for patients with widely invasive PDTCs (n = 6). DFS estimates by Kaplan–Meier analysis were significantly different between these groups (p = 0.0016).
Conclusions:
Extent of invasion appears to be an important parameter that affects clinical outcome for patients with PDTC. In our cohort, patients with encapsulated PDTC with capsular invasion only or focal vascular invasion had an excellent outcome.
Introduction
Although poorly differentiated thyroid carcinoma (PDTC) accounts for <5% of thyroid malignancies in the United States, it is a major cause of cancer-related deaths (1). There is a slight female predominance, and the average age at diagnosis is 55–70 years (2 –5). The 2017 World Health Organization (WHO) Classification of Tumors of Endocrine Organs adopted the Turin criteria for PDTC (5,6). Thus, the WHO defines PDTC as a follicular cell-derived tumor with conventional criteria of malignancy (capsular penetration or vascular invasion) with solid, insular, or trabecular growth, a lack of nuclear features of papillary thyroid carcinoma (PTC), and increased mitotic activity, tumor necrosis, or convoluted nuclei. The same criteria for PDTC can be applied to oncocytic tumors (2,3). PDTC lacks the marked pleomorphism of anaplastic thyroid carcinoma (ATC), and the proliferative rate of PDTC, which is elevated compared with differentiated follicular cell-derived thyroid carcinomas, is not as high as that of ATC. In addition, unlike ATC that always lacks thyroglobulin expression and is usually negative for thyroid transcription factor-1 (TTF-1), thyroglobulin and TTF-1 expression are generally maintained in PDTC. The prognosis of tumors with a minor component of PDTC has not been established, although there is some evidence that tumors with even a minor poorly differentiated component can pursue an aggressive clinical course (7). As a result, the 2017 WHO indicates that any poorly differentiated component should be mentioned in the pathology report (6). The clinical outcome of PDTC is intermediate between differentiated follicular cell-derived thyroid carcinomas and undifferentiated (anaplastic) thyroid carcinoma. Distant metastases are common, with lung and bone being the most frequent sites of distant metastases (2,3,7 –9). The 5- and 10-year survival of patients with PDTC as defined by WHO criteria is ∼70% and 50%, respectively (2).
The extent of invasion has been shown to be prognostic in follicular thyroid carcinoma (FTC) and Hürthle cell carcinoma (HCC) (10 –16). The outcome of patients with FTC or HCC with capsular penetration only is significantly better than that of patients with encapsulated angioinvasive tumors, which, in turn, is significantly better than that of patients with widely invasive FTC or HCC. For example, D'Avanzo et al. reported a 10-year survival of 98%, 80%, and 38% for patients with FTC with capsular invasion only, those with encapsulated tumors with angioinvasion, and those with widely invasive tumors, respectively (10). It is not only the presence of vascular invasion that is important, but also its extent (11 –13). For example, Ito et al. found that in multivariate analysis, extensive vascular invasion in FTC (defined as four or more foci of vascular invasion) is associated with significantly worse cause-specific survival, with an odds ratio of 13.7 (17). Owing to the prognostic significance of extent of invasion, all foci should be counted (with foci in adjacent vessels counted separately), and extent of vascular invasion should be categorized as focal (fewer than four foci) or extensive (four or more foci) (18). Extent of vascular invasion has also been shown to be prognostic in HCC (11). As a result of these findings, the American Thyroid Association (ATA) risk stratification classifies FTC with capsular invasion or focal vascular invasion as low risk and FTC with extensive angioinvasion as high risk (19). In addition, the ATA and National Comprehensive Cancer Network indicate that management decisions should be based on extent of invasion (19,20). The prognostic significance of extent of invasion has not been established in PDTC. Therefore, our aim was to evaluate how extent of invasion impacts clinical outcome for PDTC.
Methods
Study population and data acquisition
Approval was obtained from the Brigham and Women's Hospital Institutional Review Board. We retrospectively identified 47 consecutively diagnosed cases of PDTC that were resected between 2005 and 2018. All cases were reviewed to determine whether they met the 2017 Endocrine WHO criteria for PDTC: trabecular/insular/solid growth, absence of nuclear features of PTC, and the presence of at least 1 of the following: ≥3 mitoses per 10 HPFs, necrosis, or convoluted nuclei (6). Tumors with any poorly differentiated component were included. Histopathologic characteristics, including tumor size, presence of a differentiated component, mitotic count per 10 HPF, tumor necrosis, presence of oncocytic cytomorphology, extent of the poorly differentiated component (characterized as <50% or >50% of the tumor), gross extrathyroidal extension, tumor stage, margin status, and lymph node metastases were recorded for each case. Tumor stage was determined using the criteria defined in the 8th edition of the American Joint Committee on Cancer TNM staging system (21).
PDTC was categorized by extent of invasion as follows: (i) encapsulated with capsular invasion only, (ii) encapsulated with focal (fewer than four foci) vascular invasion (with or without capsular invasion), (iii) extensive (four or more foci) vascular invasion (with or without capsular invasion), and (iv) widely invasive (widely invasive tumors are classified as tumors that grossly invade through the gland and often have extensive vascular invasion) (6). There was an average of 2.6 slides submitted per centimeter of tumor. The tumor periphery was entirely submitted in 31 (66%) cases. Of the cases not entirely submitted, all but two had extensive invasion (defined as encapsulated angioinvasive tumors with extensive vascular invasion or widely invasive tumors). Clinical information and follow-up data were obtained for each case from the electronic medical record. For cases with clinical follow-up data available, disease-free survival (DFS), defined as the time from initial diagnosis to disease recurrence (local or distant), and disease-specific survival (DSS), defined as the time from initial diagnosis to death from disease, were recorded.
Statistical analysis
A t-test or Fisher exact test was used to compare continuous and categorical variables, respectively. Survival was depicted using the Kaplan–Meier estimation method (Prism 5; GraphPad, La Jolla, CA). For all statistical methods, p-values <0.05 were considered significant.
Results
Cohort characteristics
Forty-seven cases of PDTC were identified from 28 (60%) women and 19 (40%) men (mean age of 57 years at diagnosis; range: 28–83). The clinicopathologic characteristics of the cohort are summarized in Table 1. Histologic features of the tumors are shown in Figure 1. Forty-six (98%) patients underwent a 1- or 2-step total thyroidectomy, while 1 (2%) had a hemithyroidectomy. The patient who had a hemithyroidectomy was lost to follow-up, and it is unknown whether a completion thyroidectomy was performed. Of patients with follow-up, additional treatment was variable and included radioactive iodine (RAI) only (62%), RAI/external-beam radiation therapy (EBRT) (7%), RAI/EBRT/targeted therapy (12%), chemotherapy/EBRT/targeted therapy (2%), RAI/EBRT/immunotherapy (5%), RAI/chemotherapy/EBRT (2%), RAI/chemotherapy/targeted therapy (2%), RAI/EBRT/chemotherapy/targeted therapy (2%), and unknown additional treatment (5%). Of the patients who died of disease (DOD), treatment was again variable and included RAI/EBRT/targeted therapy (43%), chemotherapy/EBRT/targeted therapy (14%), RAI/EBRT/immunotherapy (14%), RAI/chemotherapy/targeted therapy (14%), and RAI/EBRT/chemotherapy/targeted therapy (14%). Of the patients with recurrent/metastatic disease who received RAI, more detailed information regarding the degree of iodine uptake was only available for nine patients. These patients all had either widely invasive primary tumors or tumors with extensive angioinvasion. For the recurrent/residual disease, 6 had uptake while 3 did not. Two of the three patients who did not have significant uptake had oncocytic tumors.
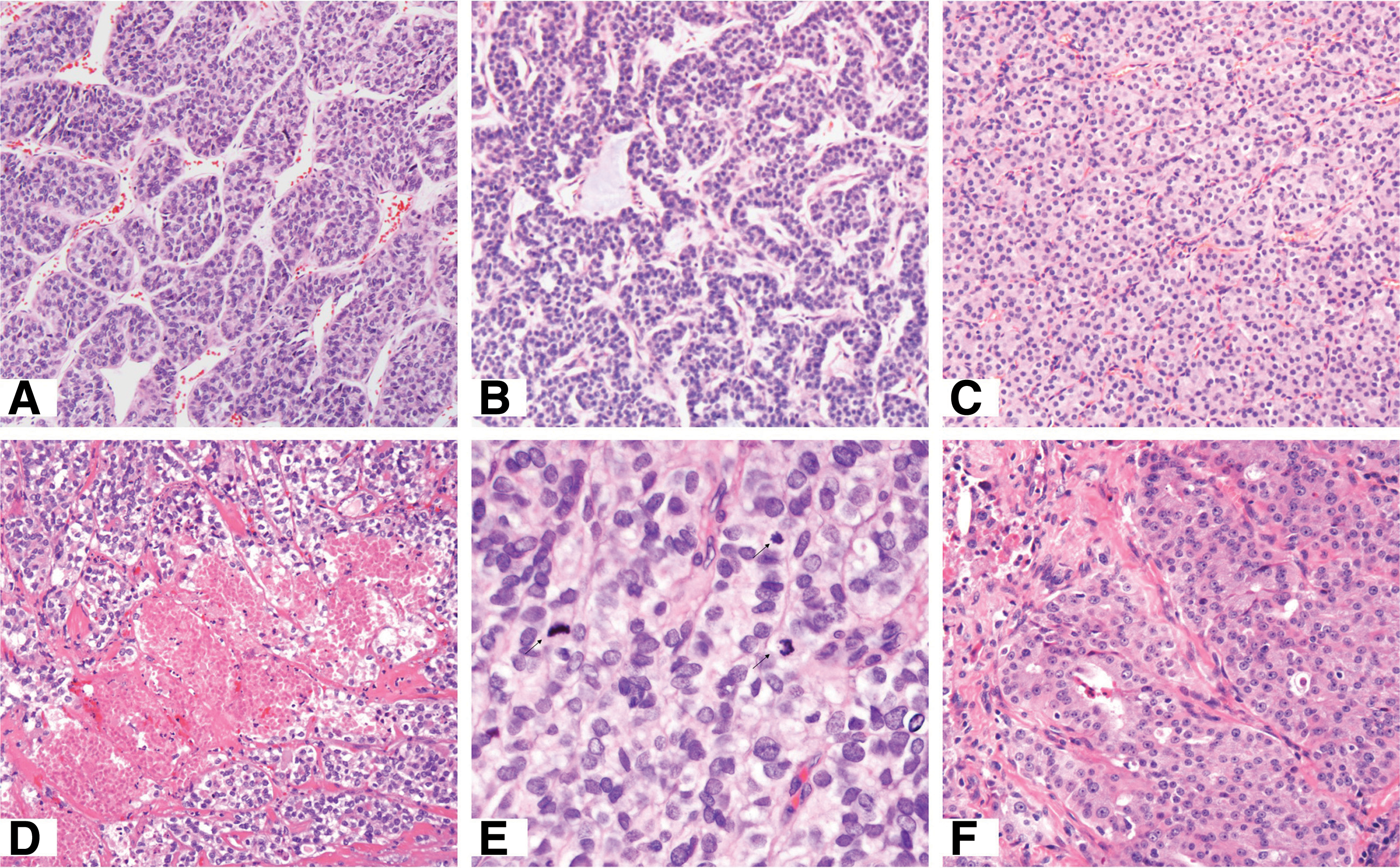
Examples of PDTC. All cases demonstrated insular (
Clinicopathologic Characteristics of Patients with Poorly Differentiated Thyroid Carcinoma (n = 47)
Of 21 (45%) patients with lymph nodes taken at the time of thyroid resection.
Of 42 (89%) patients with sufficient clinical follow-up.
CCV, columnar cell variant of papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; FVPTC, follicular variant of papillary thyroid carcinoma; HCC, Hürthle cell carcinoma; HPF, high-power fields.
The mean tumor size was 4.3 cm (range: 0.9–8.5 cm; standard deviation 1.8 cm). PDTC was a major component (>50%) of the tumor in 30 (64%) cases and a minor component in 17 (36%) cases. Within the poorly differentiated component, mitoses numbered 8 per 10 HPF on average (range: 1–34 per 10 HPF), and tumor necrosis was present in 21 (45%) cases. Although some cases had convoluted nuclei in the poorly differentiated component, all cases (in addition to having solid/trabecular/insular growth) had 3 or more mitoses per 10 HPF or tumor necrosis. There were no tumors that had the appropriate growth pattern and convoluted nuclei only. In addition, 15 (32%) cases had oncocytic cytomorphology. Evaluation of extent of invasion demonstrated that 8 (17%) cases were encapsulated with capsular penetration only, 5 (11%) were encapsulated with focal vascular invasion, 18 (38%) were encapsulated with extensive vascular invasion, and 16 (34%) were widely invasive. T4 disease was present in 6 (13%) cases, and 11 (23%) cases had positive resection margins. Twenty-one (45%) patients had lymph nodes taken at the time of primary resection, of which 10 (21%) were taken incidentally and 11 (23%) were from targeted biopsies or dissections. Of these 21 patients, 8 (38%) had lymph node metastases. All but one case with positive lymph nodes had a targeted biopsy or dissection.
Clinical outcome
Overall, 42 (89%) patients had follow-up data. Of these patients, 7 (17%) DOD, with a mean survival of 6.4 years (median: 6.3 years, range: 2.5–10 years, standard deviation 3.2 years). Eleven (26%) patients were alive with distant metastatic disease at last follow-up, and 24 (57%) had no evidence of disease (mean follow-up 5.6 years, median 6.4 years, standard deviation 4.1 years). Of the patients with residual or recurrent disease, 8 (19%) presented with distant metastases at diagnosis, while 10 (24%) developed distant metastases at recurrence. The most common distant metastatic sites were lung (83%) and bone (56%), with less commonly involved sites including brain (17%), soft tissue (17%), and visceral organs such as adrenal gland, kidney, and liver (22%). In addition, 8 patients with distant disease also developed local recurrences in the neck. In patients who were M0 at diagnosis, the mean time to recurrence (local or distant) was 2.8 years (median: 2.6 years; range: 0.3–7.5 years; standard deviation 2.5 years).
When comparing patients who DOD with those who were still alive with at least 5 years of follow-up, there was no significant difference in patient age, sex, tumor size, and extent of the poorly differentiated component (Table 2). However, patients who DOD were more likely to have tumors with oncocytic cytomorphology (p = 0.011) and distant metastases at diagnosis (p = 0.042). Distant metastases at diagnosis and oncocytic cytomorphology were also shown to be significant by Kaplan–Meier analysis for DSS (p = 0.0007 and p = 0.0093, respectively). The 5-year DSS for patients with distant metastases at diagnosis was 50% compared with 96% for patients without distant metastases at diagnosis. The 5-year DSS for patients with oncocytic PDTC was 75% compared with 95% for patients with PDTC without an oncocytic cytomorphology. There was no difference in M1 status at diagnosis or extent of invasion in oncocytic PDTC cases and cases of PDTC without an oncocytic cytomorphology.
Clinicopathologic Characteristics of Poorly Differentiated Thyroid Carcinoma (PDTC) Patients Dead of Disease and PDTC Patients Alive (With at Least 5 Years Follow-Up)
Of 21 (45%) patients with lymph nodes taken at the time of thyroid resection.
DOD, died of disease.
Clinical outcomes based on extent of invasion are summarized in Table 3. In patients with sufficient clinical follow-up, the 5-year DFS was 83% in patients with tumors with focal capsular invasion (the one patient with disease presented with distant metastases), 100% in patients with tumors with focal vascular invasion, 57% in patients with tumors with extensive vascular invasion, and 10% in patients with widely invasive tumors. In patients who were M0 at diagnosis, the 5-year DFS was 100% in patients with tumors with focal invasion (capsular or focal vascular invasion), 73% in patients with tumors with extensive vascular invasion, and 17% in patients with widely invasive disease. Using Kaplan–Meier analysis, the difference in DFS between these subgroups was significant (p = 0.0016; Fig. 2a). The difference in DFS between subgroups was also significant when only looking at patients with PDTC without an oncocytic cytomorphology (p = 0.019; Fig. 2b). Although the DSS was not significantly different between subgroups, it trended toward significance when comparing patients with tumors with focal invasion only (capsular invasion only or focal vascular invasion) and those with tumors with extensive invasion (encapsulated tumors with extensive vascular invasion or widely invasive tumors) (p = 0.13; Fig. 2c).
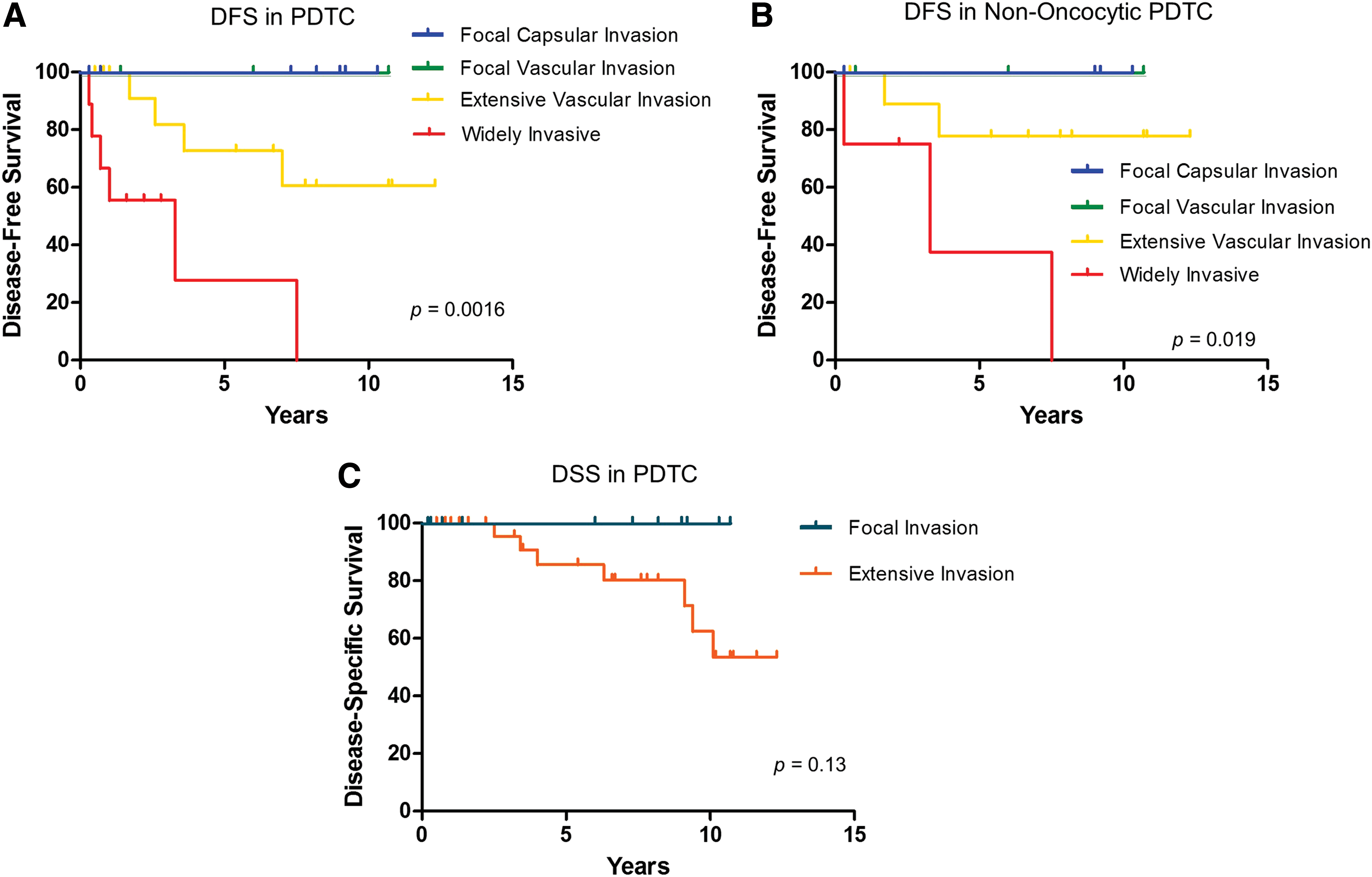
Outcomes of PDTCs by extent of invasion. DFS was significantly different between tumors with varying extents of invasion (
Outcome of Poorly Differentiated Thyroid Carcinoma by Extent of Invasion
Excluding 10 patients without sufficient clinical follow-up.
Excluding 15 patients without sufficient clinical follow-up.
Excluding 27 patients without sufficient clinical follow-up.
AWD, alive with disease; DFS, disease-free survival; DSS, disease-specific survival; Dx, diagnosis; NED, no evidence of disease; PDTC, poorly differentiated thyroid carcinoma.
Using Kaplan–Meier analysis, neither DSS nor DFS differed significantly based on pathologic tumor stage (p = 0.87 and 0.29, respectively). Most patients who were M0 at diagnosis had pT2 or pT3 tumors (35% and 47%, respectively), while 3 (9%) patients had pT1 tumors and 3 (9%) had pT4 tumors. Among patients with pT2 tumors, all 4 with focal invasion only (capsular or vascular) did not have evidence of recurrence, although 3 of the 8 patients with extensive invasion recurred. When comparing patients with pT3 tumors, all 5 patients with focal invasion did not recur compared with 5 of 11 patients with extensive invasion. Using Kaplan–Meier analysis, the difference in DFS among those with pT2 tumors when comparing extent of invasion did not reach significance (p = 0.27), although the difference was significant among those with pT3 tumors (p = 0.04).
Discussion
PDTC is both histologically and clinically intermediate between differentiated follicular cell-derived thyroid carcinomas and undifferentiated (anaplastic) thyroid carcinoma. The 2017 WHO Classification of Tumors of Endocrine Organs defines PDTC as a tumor with conventional criteria of malignancy (capsular penetration or vascular invasion) with solid, insular, or trabecular growth, a lack of nuclear features of PTC, and increased mitotic activity, tumor necrosis, or convoluted nuclei (6). The clinical outcome of FTC and HCC has been shown to depend on extent of invasion (10 –16). Therefore, the aim of our study was to evaluate the prognostic significance of extent of invasion in PDTC defined by current WHO criteria.
Our cohort included 47 consecutively diagnosed cases of PDTC. Consistent with the aggressive nature of PDTC, the majority of tumors showed extensive invasion, that is, most were widely invasive (34%) or were encapsulated but with extensive vascular invasion (38%). However, focal invasion was present in 28% of the cohort, with 17% of cases encapsulated with capsular penetration only and 11% encapsulated with focal vascular invasion. Approximately one-third of our cohort was comprised of oncocytic PDTC and approaching 20% presented with distant metastases at diagnosis. As has been shown previously for PDTC, FTC, and HCC (1,12,22), patients with M1 disease at diagnosis had a significantly worse outcome than those without distant metastases at diagnosis. Interestingly, patients with oncocytic PDTC also had a worse outcome than patients with PDTC without an oncocytic morphology. Although Asioli et al. found no difference in outcome for patients with oncocytic and nononcocytic PDTC (2), our results are consistent with those of Dettmer et al. (3). The difference in behavior of oncocytic PDTC could be a reflection of differences in underlying molecular alterations of oncocytic (Hürthle cell) tumors (23 –25) or could be a result of decreased iodine uptake (22,26,27).
We found that clinical outcome varied depending on extent of invasion. The 5-year DFS was 83% in patients with tumors with focal capsular invasion, 100% in tumors with focal vascular invasion, 57% in tumors with extensive vascular invasion, and 10% in widely invasive tumors. It has previously been shown that the rare FTC with capsular penetration only with distant metastases often have these metastases at initial clinical presentation (which means the aggressive nature of the tumors is clinically apparent at the time of diagnosis) (10,16). It is interesting that the one patient with a tumor with capsular invasion only and residual disease in our cohort presented with distant metastases at diagnosis. When only patients who were M0 at diagnosis were considered, the 5-year DFS was 100% in patients with tumors with focal invasion (capsular invasion or focal vascular invasion), 73% in tumors with extensive vascular invasion, and 17% in widely invasive disease. The difference in DFS between these subgroups was significant in Kaplan–Meier analysis and was maintained when only considering patients with PDTC without an oncocytic cytomorphology. Although the DSS was not significantly different between subgroups, it trended toward significance when comparing patients with tumors with focal invasion only and those with tumors with extensive invasion. Although extent of vascular invasion has been recorded in prior studies (2,5,28), the significance of extent of invasion has not been evaluated in tumors with the periphery thoroughly evaluated histologically. Although the periphery of the tumor was entirely submitted in only 66% of our cohort, it was predominantly the widely invasive tumors or the encapsulated tumors with extensive invasion with more limited sampling of the periphery. In fact, the entire capsule was submitted for all but two tumors with focal invasion only.
Although our findings are compelling, we acknowledge several weaknesses of our study. It is a retrospective study and a relatively small single-institution cohort. Moreover, because our cohort is small and the postoperative treatment strategy of patients was variable, we were not able to evaluate impact of adjuvant therapy on patient outcome. However, the efficacy of RAI, EBRT, or chemotherapy in PDTC is, at this time, not established (1).
In summary, extent of invasion appears to be an important parameter that affects clinical outcome for patients with PDTC. In our cohort, patients with encapsulated PDTC with capsular invasion only or focal vascular invasion had an excellent outcome. If our findings are confirmed, it raises the question of whether extent of invasion should be included to refine the risk stratification of PDTC.
Footnotes
Author Disclosure Statement
J.H.L. receives research support to the institution from Novartis, Bayer, and BMS and consulting honoraria from Bayer, Genentech, and Ignyta.
Funding Information
No funding was received for this article.