
Abstract
Background:
The prognosis of several human malignancies has dramatically improved after the introduction of tyrosine kinase inhibitors (TKIs); however, their use has been associated with a large spectrum of adverse events, including symptomatic biliary disorders. In the phase III trial of lenvatinib in radioactive iodine (RAI)-refractory differentiated thyroid cancer (DTC) patients, gallbladder (GB) and biliary duct (BD) diseases and complications were reported. We evaluated symptomatic biliary disorders during treatment with lenvatinib in real-life practice to provide a more exhaustive understanding of its toxicity.
Methods:
We retrospectively evaluated all consecutive patients treated with lenvatinib in our center for progressive RAI-refractory DTC, excluding those who underwent cholecystectomy before the start of therapy. We report all radiologically confirmed symptomatic GB/BD disorders, which were subsequently treated with cholecystectomy, and we describe their management along with relevant biochemical and histological findings. All available GB/BD imaging of patients who developed biliary toxicity during lenvatinib was reviewed by a single experienced radiologist, including computed tomography scans performed for tumor assessment at baseline and during TKI therapy.
Results:
Five patients (14.7%) developed symptomatic radiologically confirmed biliary disease after a median time of 4.4 months of lenvatinib treatment [interquartile range 3.4–14.4 months] and thus underwent cholecystectomy. A scheduled surgical approach was possible only in two cases; in the remaining patients, presurgical TKI interruption was shorter than one week. After wound healing, treatment was resumed by all subjects. Three patients showed mild biochemical alterations in the two previous monthly follow-up visits. Before the start of treatment, GB/BD abnormalities were radiologically detected only in one case.
Conclusions:
In our cohort, an unexpectedly high proportion of RAI-refractory DTC patients treated with lenvatinib developed a symptomatic biliary disorder with the need of surgical intervention. Further studies are required to optimize the diagnosis and treatment of patients at higher risk of developing a symptomatic GB/BD disease during assumption of lenvatinib.
Introduction
Differentiated thyroid cancer (DTC) represents the majority of thyroid neoplasms; the remaining tumors deriving from follicular cells are classified as poorly differentiated thyroid carcinoma (PDTC) or anaplastic thyroid carcinoma (1). The initial treatment of DTC includes surgery followed by radioactive iodine (RAI) treatment, if needed, and levothyroxine therapy (2). Although these patients generally have a favorable prognosis, nearly 10% of them develop RAI-refractory distant metastases, with a significant worsening in survival rates (3).
In RAI-refractory DTC, traditional chemotherapy and external beam radiotherapy showed low efficacy and high toxicity. In recent years, the development of molecular therapies—targeting aberrant signaling pathways involved in thyroid tumorigenesis—has radically changed the management of RAI-refractory DTC patients (4). Sorafenib and lenvatinib, two oral multitargeted receptor tyrosine kinase inhibitors (TKIs), have been recently approved for the treatment of locally recurrent or metastatic progressive RAI-refractory DTC after the encouraging results observed in phase III studies (5,6). Lenvatinib inhibits the vascular endothelial growth factor receptor (VEGFR) 1–3, fibroblast growth factor receptor (FGFR) 1–4, platelet-derived growth factor receptor (PDGFR) α, rearranged during transfection (RET), and KIT proto-oncogenes.
In the multicenter, randomized, double-blind, placebo-controlled, phase III SELECT trial, treatment with lenvatinib significantly prolonged the median progression-free survival (PFS) and improved response rate in comparison to placebo in patients with RAI-refractory DTC. However, almost all patients experienced adverse events (AEs) during therapy, requiring reduction of dosage and drug interruption or discontinuation (6). These findings were later compared with those observed in real-life clinical practice, leading to increasing awareness of drug-related complications (7 –10).
Gastrointestinal (GI) AEs, such as abdominal pain, nausea, and vomiting, occur in a relevant percentage of patients treated with lenvatinib. A limited number of gallbladder (GB) and biliary duct (BD) diseases and complications were reported among treatment-related serious AEs in the SELECT trial (6). The summary of product characteristics (SPC) of lenvatinib, approved by both the Food and Drug Administration (FDA) and the European Medicines Agency (EMA), includes cholecystitis and pancreatitis among possible AEs (11,12). However, a focused evaluation of biliary disorders during treatment with lenvatinib in real-life practice is still lacking.
In recent years, other TKIs have shown to cause or worsen GB/BD disorders (13,14). Table 1 summarizes the most relevant studies that showed associations between TKI therapies and occurrence of GB/BD disorders. Even if the pathophysiological mechanisms underlying these drug-related AEs are not completely understood, clinicians need to be aware of this potentially life-threatening toxicity when managing advanced cancer patients. Before the start of treatment with lenvatinib, baseline evaluation includes liver and biliary tract function tests, which should be monitored during the whole treatment (11,12). There is still no evidence supporting a routine GB/BD-focused evaluation by ultrasound (US) at baseline and during therapy.
Summary of Relevant Studies About Tyrosine Kinase Inhibitors and Gallbladder/Biliary Tract Complications
Case report/case series.
CML, chronic myeloid leukemia; CRC, colorectal cancer; DTC, differentiated thyroid cancer; GB, gallbladder; GIST, gastrointestinal stromal tumor; HCC, hepatocellular carcinoma; MTC, medullary thyroid cancer; NA, not available; NSCLC, nonsmall-cell lung cancer; RCC, renal cell carcinoma.
The aim of our retrospective study was to describe the main characteristics, the management, and the outcomes of symptomatic biliary disorders during treatment with lenvatinib in a cohort of patients with advanced RAI-refractory thyroid cancer consecutively treated at a tertiary referral center.
Materials and Methods
We retrospectively analyzed all patients who started treatment with lenvatinib for advanced RAI-refractory DTC or PDTC at our center from June 2012 to December 2018. Patients were defined RAI-refractory if there was no further indication for RAI therapy, because of a partial or complete lack of RAI uptake, or with progressive disease despite RAI avidity, or after having received a cumulative RAI activity ≥600 mCi (15). Patients with progressive and symptomatic disease and with contraindication to RAI therapy were also included in this category. All patients showed progression within the previous six months, according to the RECIST 1.1 criteria (16).
To assess treatment efficacy, subsequent contrast-enhanced computed tomography (CT) scan evaluations were performed nearly at three months after the start of treatment and then at three- or six-month intervals. Physical examination and laboratory analysis (including liver and biliary tract function tests) were performed at baseline and subsequently at monthly follow-up visits. The daily starting dose of lenvatinib ranged from 10 to 24 mg, depending on the characteristics of the disease and the patient clinical conditions. Dose reductions and/or drug interruptions were performed in case of drug-related AEs, defined according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) version 4.03 (17).
The definition of GB/BD disorders or complications included the following: GB/BD stones or sludge; GB mucocele, empyema, perforation, or fistula; cholecystitis or cholangitis; and pancreatitis. We excluded from the study those patients who underwent cholecystectomy before the start of lenvatinib.
During treatment, we collected all GB/BD disorders that were radiologically confirmed after the onset of suggestive symptoms (e.g., dyspepsia, fever, upper abdominal pain, nausea, or vomiting) and treated with cholecystectomy. In these subjects, a radiological diagnosis of GB/BD disorder was performed by US, contrast-enhanced CT, and/or magnetic resonance imaging. We describe the management of these patients, together with all relevant clinical and laboratory abnormalities, such as increase in serum alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, gamma-glutamyltransferase (GGT), bilirubin, amylase, C reactive protein, and/or leukocytosis on whole blood cell count. All histological findings are also reported.
All available GB/BD images of patients who developed biliary toxicity during treatment with lenvatinib were reviewed by a single experienced radiologist, including CT scans performed for tumor staging at baseline and during TKI therapy. We examined the presence of radiological biliary alterations (GB dilatation and wall thickening, pericholecystic fluid, GB/BD stones) both before the start of and during treatment with lenvatinib until the onset of symptomatic biliary disease. Changes in GB thickness were determined through a direct comparison of the last CT scan performed before the symptomatic biliary event and during the acute event (if a CT scan was performed).
Baseline characteristics of patients are summarized descriptively using numbers and percentages or median and interquartile range (IQR).
All procedures performed were in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This study was approved by the institutional review board (IRB).
Results
From June 2012 to December 2018, 36 patients started treatment with lenvatinib for advanced RAI-refractory DTC or PDTC at our center. Two of them had undergone laparoscopic cholecystectomy before the start of treatment and were therefore excluded from our analysis. Median age at the start of treatment with lenvatinib was 67.2 years [IQR 57.6–72.7 years] and 61.8% were female; The median follow-up was 16.1 months [IQR 5.3–30.3 months].
After a median time of 4.4 months [IQR 3.4–14.4 months] from the start of therapy, 5 of 34 patients (14.7%) experienced a symptomatic GB/BD disorder and underwent cholecystectomy.
In this group, lenvatinib was taken at a daily dosage of 24 mg in two cases, 20 mg in two other cases, and 14 mg in the remaining one. The first transient interruption and the first drug dose reduction were required after a median time of 2.8 months [IQR 1.9–3.7 months] and 4.2 months [2.8–6.0 months] of treatment, respectively. The median weight loss from the start of therapy to the diagnosis of symptomatic GB/BD disorder was 15.9% [9.2–25.7%] of baseline body weight. At the first radiological tumor assessment during treatment, a partial response was observed in one patient, while the remaining subjects showed stable disease as their best response. None of them had liver metastases.
Radiological detection of GB/BD disorders was obtained after the onset of acute abdominal symptoms, which led to admission of the patients to the emergency department. Among them, three patients showed mild blood test abnormalities during the two previous monthly follow-up visits (increased GGT values in all cases), as reported in Figure 1. Two patients showed transient resolution of symptoms, one through medical treatment and the other through the placement of a biliary stent. For these patients, a cholecystectomy could be programmed, and a scheduled presurgical lenvatinib interruption of one week was planned accordingly. In the remaining subjects, urgent surgical procedures were necessary and an adequate drug interruption before intervention was not feasible.
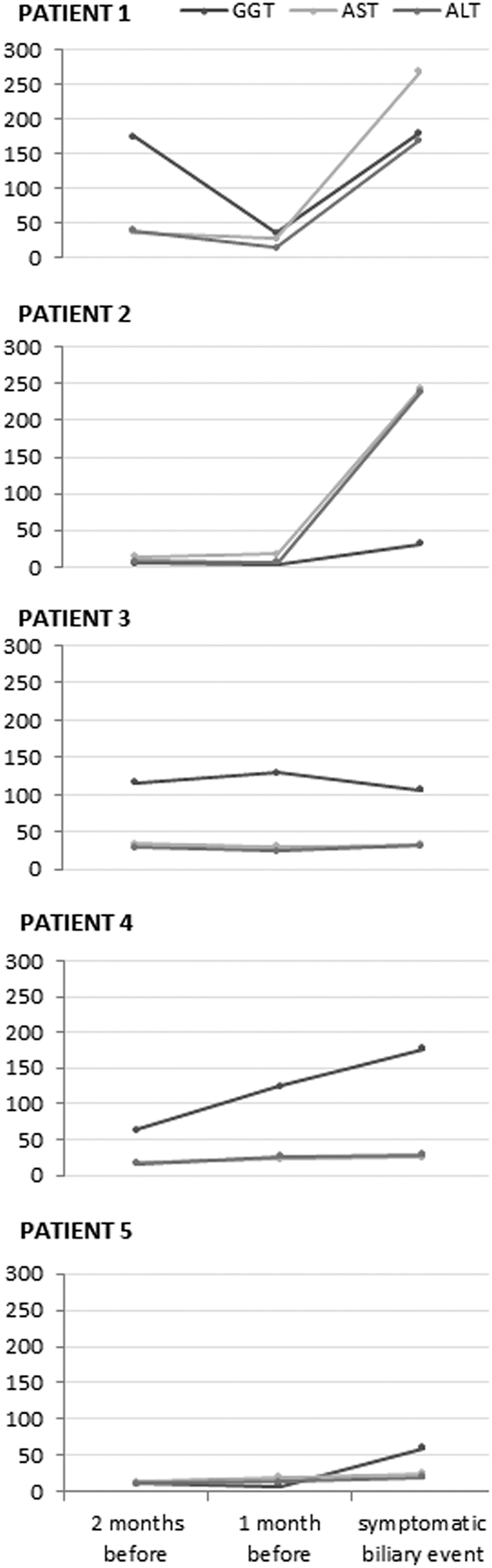
Serum ALT, AST, and GGT levels in occasion of the symptomatic biliary event and during the two previous monthly follow-up visits. ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyltransferase.
All patients underwent laparoscopic cholecystectomy, which was converted to open cholecystectomy only in a single case. In this subject, there was also a need to subsequently perform a postsurgical endoscopic retrograde cholangiopancreatography and to position a biliary stent for cystic duct dehiscence. Wound healing process after surgical intervention was good in four patients, and lenvatinib was restarted at the same dosage one week after the surgery. However, a subcutaneous hematoma and delayed wound healing occurred in one patient who could not perform a presurgical interruption of the lenvatinib therapy. In this case, lenvatinib was resumed after a month of interruption. All relevant clinical, biochemical, radiological, and histological findings related to the symptomatic biliary disorders are summarized in Table 2.
Summary of Clinical, Biochemical, Radiological, and Pathological Findings at the Onset of Symptomatic Biliary Disease
ALT, alanine transaminase; AST, aspartate transaminase; BD, biliary ducts; CBD, common bile duct; CPR, C-reactive protein; CT, computed tomography; ERCP, endoscopic retrograde cholangiopancreatography; GGT, gamma-glutamyltransferase; MRI, magnetic resonance imaging; US, ultrasound.
A single radiologist retrospectively reviewed all available GB/BD images of the lenvatinib-treated patients submitted to cholecystectomy. Baseline contrast-enhanced CT scans were performed 3.3 months [IQR 2.1–4.2 months] before the initiation of therapy. Only one patient showed cholelithiasis before the start of lenvatinib; in the remaining cases, no significant radiological GB/BD abnormalities could be found before TKI therapy but occurred during treatment, as illustrated in Figure 2. During treatment, an isolated slight GB wall thickening was retrospectively detected in three patients in the restaging CT scans performed before the symptomatic biliary event. In the remaining two cases, GB/BD disease occurred before the first radiological tumor evaluation during therapy with lenvatinib.

Radiological gallbladder/biliary ducts characteristics before the start of therapy (left) and during symptomatic biliary disease (right) in one patient of our cohort.
Comparison of the last CT scan performed before the symptomatic biliary event and the CT scan performed during the acute event (when available) showed a change in GB wall thickness ranging from 0.8 to 1.6 mm; the median time interval between the two CT assessments was 5.4 months [IQR 4.8–6.7 months].
Discussion
In the SELECT trial, lenvatinib led to a significant prolongation of the PFS and improved response rates in comparison to placebo in patients with RAI-refractory DTC (6). However, this drug showed relevant toxicity, and almost all patients required supportive care combined with dose reduction and/or transient drug interruption to manage AEs (18,19). These findings have also been confirmed in real-life experiences with lenvatinib (7,8,10). GI toxicity occurred in a high percentage of patients. The most frequent GI AEs reported both in the SELECT trial and in the real-life setting were diarrhea, nausea, and decreased appetite; abdominal pain was reported in nearly 10–15% of patients (6,9). In very few cases, these symptoms might be warning signs of a more serious medical disease with potentially life-threatening consequences. However, because these symptoms are extremely unspecific, early detection of an underlying condition can be difficult.
In our population of patients treated with lenvatinib, we found an unexpectedly high incidence of severe symptomatic GB/BD disease requiring surgical intervention (14.7%). In the SELECT trial, only a small number of biliary disease or complications were reported among lenvatinib-related serious AEs (GB mucocele 0.4%, GB perforation 0.4%, pancreatitis 0.4%) (6). In the SPC issued by the EMA for lenvatinib, cholecystitis and pancreatitis are included among “common” and “not common” AEs, respectively (12). Cholecystitis and pancreatitis are reported in the FDA SPC among the AEs detected during postapproval use of lenvatinib, although neither the incidence nor a correlation to drug exposure has been established (11).
During the past years, previous studies found an association between GB/BD disorders and treatment with TKIs; the most relevant studies are summarized in Table 1. Sunitinib was associated with GB toxicity, either in patients with GI stromal tumors (20) or in patients with metastatic renal cell carcinoma (13,21 –23). Motesanib was associated with GB alterations (increased GB volume, decreased GB function, development of gallstones, and biliary sludge) in advanced solid tumors (14,24 –29). Furthermore, the development of cholecystitis and cholelithiasis was reported during treatment with imatinib in patients with chronic myeloid leukemia and GI stromal tumors (30 –32), and single case reports or postmarketing warnings regarding the onset of cholecystitis or cholelithiasis were described for axitinib (33) and sorafenib (34).
The pathophysiological mechanisms underlying the TKIs AEs on the biliary system are not completely known. Physiologically, cholangiocytes express VEGFR-2 and VEGFR-3, and the secretion of VEGF by hepatocytes and cholangiocytes influences the proliferation of the BD epithelium and the peribiliary arterial plexus. Therefore, inhibition of the VEGF pathway by TKIs may alter the interaction of the endothelium and platelets and result in local endothelial dysfunction, BD epithelium ischemia (35), and thrombotic events, such as arteriolar occlusion of the GB wall (34,36), with subsequent development of biliary system disorders.
Moreover, some TKIs (e.g., imatinib) inhibit the cytochrome system, thus interfering with the metabolism of other drugs and favoring biliary excretion of cholesterol while reducing excretion of biliary salts (31,37).
All these effects could be worsened by the prevalent biliary excretion of some TKIs, such as motesanib and lenvatinib (11,14), which leads to accumulation of these drugs and their metabolites in the biliary fluids.
In our cohort, symptomatic biliary disorders occurred after a median time of 4.4 months [IQR 3.4–14.4 months] after the start of lenvatinib, suggesting that symptomatic GB/BD can be detected even in the first months of therapy. This finding is similar to those reported with sunitinib and motesanib, as GB alterations appeared early in the course of treatment.
Since we decided to focus on a homogeneous group of patients with a clinically significant disease, only patients with symptomatic GB/BD disorders submitted to surgery were evaluated, excluding those patients with biliary disease accidentally detected during restaging CT scan, who never developed a symptomatic acute event, from the analysis.
Gallstone disease derives from a complex interaction of genetic, environmental, and metabolic factors. Rapid weight loss, in case of bariatric surgery or very-low-calorie diet, was reported among the risk factors of gallstone formation. In this group of patients, the temporary use of ursodeoxycholic acid (at least 500 mg per day) may be recommended until body weight is stabilized (38). Rapid weight loss represents one of the most frequent AEs during lenvatinib treatment (6). In our patients with biliary toxicity, the median weight loss from the start of TKI therapy to diagnosis of symptomatic GB/BD disorders was remarkable with 15.9% of the baseline body weight, and this might have contributed to gallstone formation. Nevertheless, no clear relationship can be established on the basis of retrospective studies.
The presence of a possible correlation between the initial dose of lenvatinib and the onset of biliary disorders could not be explored due to the small sample size. However, it is worth underlining that three of the five patients who developed symptomatic GB/BD disease did not take the maximum lenvatinib dosage, and biliary toxicity became clinically significant with an intermediate dose of lenvatinib (14 or 20 mg per day) in all cases.
Evaluation of the GB/BD by US was not routinely performed at baseline and during therapy with lenvatinib in our cohort of DTC patient. To examine GB/BD characteristics at baseline and during treatment in the subjects who underwent cholecystectomy, a single radiologist retrospectively reviewed all available imaging, which included CT scans performed for tumor staging. Taking into account the limits of this radiological technique for the study of the biliary tree, it emerged that only one patient already showed cholelithiasis at baseline, while in the remaining cases, no radiological GB/BD abnormality could be found before the start of lenvatinib. This suggests that lenvatinib may lead to the development of biliary disease also in the absence of pre-existing GB/BD alterations.
During TKI treatment, mild biliary alterations were retrospectively detected in patients who had at least one CT scan while on therapy before the onset of symptomatic biliary disease; however, the true impact of these changes remains unknown.
The small sample size represents the main limitation of this analysis. However, RAI-refractory DTC is a relatively rare disease, and only a limited number of patients are treated with lenvatinib. Moreover, we gathered the first real-life data focusing on symptomatic biliary disorders during treatment with this drug in this cohort of patients treated at a single tertiary referral center.
Our findings draw attention to a potential lenvatinib-related AE with remarkable clinical implications. The retrospective nature of this study, which was triggered by the observation of several biliary events in our patients, cannot allow to draw definite conclusions on this issue, which needs to be further explored in prospective multicentric studies with larger cohorts of patients.
If the findings reported here will be confirmed, patients should be informed about the possibility of GB/BD toxicity, and adequately warned to suspend lenvatinib before and after the surgery. Endocrinologists and oncologists should cooperate with radiologists to gain increased awareness about this issue. Biliary alterations should be sought and reported on all restaging CT scans, even in the absence of pre-existing GB/BD disease.
The utility of a focused biliary US evaluation at baseline and during treatment with lenvatinib needs to be prospectively explored. There is still insufficient evidence to recommend medical treatment with ursodeoxycholic acid to prevent cholesterol gallstone formation, and/or a prophylactic surgical intervention in patients with biliary alterations before the start of treatment or during TKI therapy.
In conclusion, symptomatic biliary disorders can occur during treatment with lenvatinib for DTC, also in patients with absent GB/BD disease at baseline, and lead to a need for surgical intervention. Further investigations are needed to define the real impact of this problem and the proper management of these cases with the aim to improve their clinical outcome.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.