
Abstract
Background:
The correlation between the injured recurrent laryngeal nerve (RLN) with incomplete loss of signal (LOS) and the outcomes of vocal cord function is still not well understood. This large cohort validation study was aimed to evaluate the effectiveness of the warning criterion, the reduction of the R2p/R2d ratio, in neuromonitoring during thyroidectomy.
Methods:
A total of 1108 consecutive patients (1764 nerves) with normal vocal cord function undergoing monitored thyroidectomy were included. Standardized intraoperative neuromonitoring procedures were strictly followed, after complete dissection of RLN, the exposed RLN was routinely stimulated at the lowest proximal end (R2p signal) and the most distal end near the laryngeal entry point (R2d signal). If the reduction of the R2p/R2d ratio (([R2d − R2p]/R2d) × 100%) reached >20%, the whole exposed RLN would be checked to pinpoint the injured area of the nerve.
Results:
Visual anatomical integrity of the RLN was ensured in all 1764 nerves. Eighteen nerves had complete LOS, and the other 97 nerves had incomplete LOS where the reduction of the R2p/R2d ratio ranged from 21% to 84%. Postoperative temporary vocal cord paralysis (VCP) was noted in 11 (61.1%) RLNs with complete LOS and 16 (16.5%) RLNs with incomplete LOS, where the reduction of the R2p/R2d ratio ranged from 63% to 84%. The positive predictive value of a R2p/R2d ratio >63% for postoperative VCP was 79.4%.
Conclusions:
Testing and comparing the R2p and R2d signals were useful to detect RLN neurophysiologic injury, elucidating the mechanism of nerve injury and predicting vocal cord function. Determining R2p-R2d was found to be essential and can be applied in routine neuromonitoring thyroidectomy.
Introduction
Intraoperative neuromonitoring (IONM) is helpful in thyroid surgery as visual anatomic integrity is not equal to functional integrity of the recurrent laryngeal nerve (RLN) (1). Application of intermittent IONM (I-IONM) during monitored thyroidectomy enables the early localization of the RLN, avoiding excessive manipulation to the nerve and possible extralaryngeal branches, or anatomic variations (2). An additional advantage of IONM is the evaluation of the laryngeal nerve function before, during, and after dissection, and confirmation of the nerve's functional integrity. RLN injury resulting in vocal cord paralysis (VCP) is an infrequent but potentially detrimental complication of thyroidectomy. However, no significant benefit of IONM over visualization alone in reducing the rate of RLN injuries could be proven in some studies (3,4). It does help with elucidating the mechanism of nerve injury and with reorienting the surgical strategy when a loss of signal (LOS) occurs after resection of the first lobe during bilateral thyroidectomy (5 –7). The International Neuromonitoring Study Group (INMSG) recommends that neural monitoring information should be obtained and utilized in the strategy of a planned bilateral procedure by staging the surgery in the setting of ipsilateral LOS (8).
However, the possibility to have false-positive (FP) (LOS without post-VCP) results has been widely documented in the literature, and was found to be as high as 85% (5). The positive predictive value (PPV) of VCP prediction was reported to vary from 35% to 75% (9). During standardized IONM procedures, the postsurgical dissection electromyographic (EMG) amplitudes from RLN and vagal nerve stimulation (R2 and V2 signals) are often used for comparison with the predissection signals and prediction of vocal cord function (10,11). Improved or unchanged postdissection EMG signals confirm the intraoperative functional integrity of the RLN and indicate a normal vocal cord function, while postdissection LOS often indicates postoperative VCP (12). A severely weakened signal might reflect impaired vocal cord mobility, but there are no data in the literature on the correlation between weakened signals and vocal cord function. During the operation, the baseline amplitude (R1 and V1 signals) may change frequently and significantly due to EMG endotracheal tube position changes caused by traction or manipulation of the thyroid or trachea, and that makes the comparison of relative quantitative values of the postdissection and predissection EMG signal (R2/R1 or V2/V1) less reliable for the prediction of vocal cord dysfunction (13).
The evaluation of RLN injury with incomplete LOS during monitored thyroidectomy and its functional outcome has not been well described. Wu et al. tested and compared the relative amplitude reduction from the most proximal and distal ends of the RLN exposed during thyroidectomy (R2p and R2d) at the end of surgery (14). Weakened or disrupted point of nerve conduction on the exposed RLN could be detected with this procedure, which excluded a bias from the baseline amplitude change. They compared the risks of VCP for the amplitude reduction exceeding 20%, 30%, 40%, 50%, and 60%, not providing an exact cutoff value for the prediction of VCP. Herein, we prospectively collected data from 1764 nerves in a single institution to identify a clear cutoff value of the R2p/R2d ratio that ensures good vocal cord mobility. The second aim of the study was to apply the R2d-R2p determination in standardized IONM to improve the correlation between the results of EMG signals and the outcomes of vocal cord function.
Methods
Patients
Prospectively collected data from consecutive patients undergoing thyroid surgery with or without neck dissection were analyzed at a single tertiary referral academic medical center, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, P.R. China. From May 2017 to January 2018, 1119 consecutive patients undergoing neuromonitoring during thyroidectomy for various thyroid diseases were performed by the same surgeon (G.W.). Six patients were excluded because of preoperative unilateral VCP and 5 patients because of non-RLNs, thus a total of 1108 patients with 1764 RLNs (656 total thyroidectomies and 452 hemithyroidectomies) at risk were enrolled in this study. The medical ethic committee of Zhongnan Hospital of Wuhan University approved the 10 procedures of IONM for all patients in this study.
IONM setup and surgical procedures
Neuromuscular blockade was not administered during general anesthesia for all of the patients. IONM was performed using NIM-Response 3.0 (Medtronic, Jacksonville, FL) and an EMG tube with integrated surface electrodes, which were placed in contact with the vocal cords to monitor the electrophysiological activity of RLNs. Proper position of the electrodes was ensured through laryngofiberoscopic examination after positioning the patient for surgery. Standardized IONM procedures were strictly followed, and V1-R1-R2-V2 signals were recorded intraoperatively. After complete dissection of the RLNs, the exposed RLN was routinely stimulated at the lowest proximal end and R2p signal was obtained; when stimulated at the most distal end near the laryngeal entry point R2d signal was obtained (Fig. 1). The electrophysiological changes of R2p and R2d signals were compared. If the reduction of the R2p/R2d ratio (([R2d − R2p]/R2d) × 100%) reached >20%, we would check the whole exposed RLN to pinpoint the injured area of the nerve. During the operation, any resection adjacent to the nerve was performed after confirming an absent signal response by the stimulating probe. This procedure allowed for maximal protection of the nerve and avoiding inadvertent nerve injury due to misidentification. To exclude the possibility of false LOS, all procedures were managed through the troubleshooting algorithm described in the current guidelines (10,11).
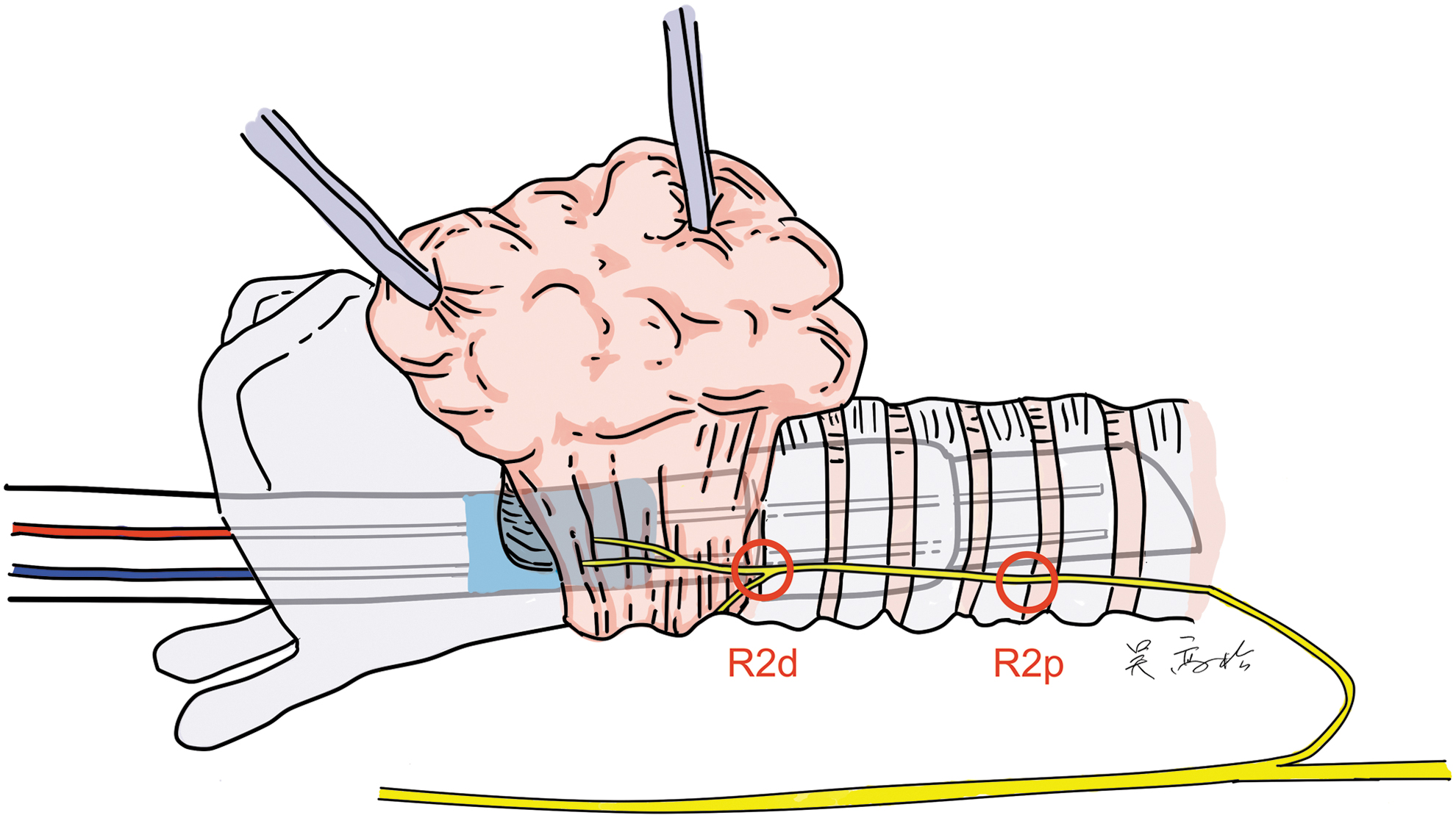
At the end of the surgery, the most proximal (R2p) and distal (R2d) points of the exposed recurrence laryngeal nerve were stimulated by a handheld stimulating probe.
In this study, complete LOS was defined as amplitude value of the final R2 < 100 μV after applying the troubleshooting algorithm. Incomplete LOS was defined as an absolute amplitude value of the final R2 > 100 μV and with reduction >50% of R1 at the end of the operation (11), or percentage of amplitude reduction >20% when comparing the R2p and R2d signals at the end of the operation (R2p/R2d ratio) (14). Injury mechanism was divided into two types: (a) segmental type 1 injury was diagnosed with a LOS proximal to a specific focal point in the operative field on the RLN, (b) global type 2 injury was diagnosed in the absence of a point of injury and on electrophysiological demonstration of LOS alongside the entire course of the ipsilateral vagal nerve and RLN. In addition, depending on the location of the injury, segmental type 1 injuries were classified as superior to, at, and inferior to the intersection of the RLN with the inferior thyroid (15). The detailed procedures of IONM are described in Table 1. Thyroidectomy was performed in accordance with the procedure established by Dr. Gaosong (16 –20). Identification and preservation of the external branch of the superior laryngeal nerve and parathyroid were routinely performed according to our previous experience (21 –23).
Ten Procedures of Intermittent Intraoperative Neuromonitoring in This Study
EBSLN, external branch of the superior laryngeal nerve; RLN, recurrent laryngeal nerve.
Follow-up
Postoperative VCP was defined as no vocal cord mobility with laryngofiberoscopic examination. Vocal cord function was routinely checked with laryngofiberoscopy on the second day after surgery. If VCP occurred, the laryngofiberoscopic examination would be performed monthly postoperatively until complete recovery of vocal cord function. All patients underwent a preoperative and postoperative laryngofiberoscopic examination by an independent laryngologist. VCP lasting for >6 months was considered as permanent VCP.
Statistical analysis
Continuous variables between groups were compared using nonparametric tests. Mann–Whitney U test and chi-square test were used to compare differences between patients with the reduction of R2p/R2d >20% and patients with normal EMG signal (Table 2). The reduction of R2p/R2d ratio was calculated as ([R2d − R2p]/R2d) × 100%. To investigate the cutoff value to predict the functional outcome after thyroidectomy, different measures based on the receiver operating characteristic (ROC) curve technique and accuracy (defined as the probability that test and diagnosis agree: [True positive + True Negative]/Total) were used (Fig. 4). p-Values <0.05 were considered statistically significant. All statistical analyses were performed using SPSS17.0 for Windows (SPSS, Inc., Chicago, IL) except for the cutoff value, which was calculated by MedCalc for Windows, version 15.2.2 (MedCalc Software, Ostend, Belgium).
Demographic Characteristic of Patients with Loss of Signal
LOS: the reduction of R2p/R2d >20%.
Mann–Whitney U test.
Chi-square test.
EMG, electromyographic; LOS, loss of signal.
Results
Outcomes of the RLNs with electrophysiological changes
All the 1764 RLNs were visually identified, and preserved anatomical integrity was confirmed. The demographic characteristics of the patients detected to have a reduction of the R2p/R2d ratio >20% and patients who did not are described in Table 2. No significant differences in age, sex, rate of malignancies, and side were found between the groups, and a difference was found in the extent of surgery. One hundred fifteen RLNs were detected with an injury on the exposed segment of the nerve. Eighteen nerves had a complete LOS and 97 nerves had an incomplete LOS where the reduction of the R2p/R2d ratio ranged from 21% to 84%. In the 97 nerves with an incomplete LOS, 68 nerves were found to have a traction injury, and among them 36 nerve injuries were located superior to the intersection of the RLN with the inferior thyroid artery, 32 nerve injuries were located inferior to the intersection of the RLN with the inferior thyroid artery. Seventeen nerves suffered from a mechanical trauma during extensive dissections because of cancer adhering to the RLN. The EMG signal of 12 nerves decreased because of the use of an energy-based device (EBD) adjacent to the nerve. Of the 18 nerves detected with complete LOS, 12 nerves were injured by traction. The remaining six nerve injuries were caused by thermal injury adjacent to the nerve. A study flow chart is presented in Figure 2.
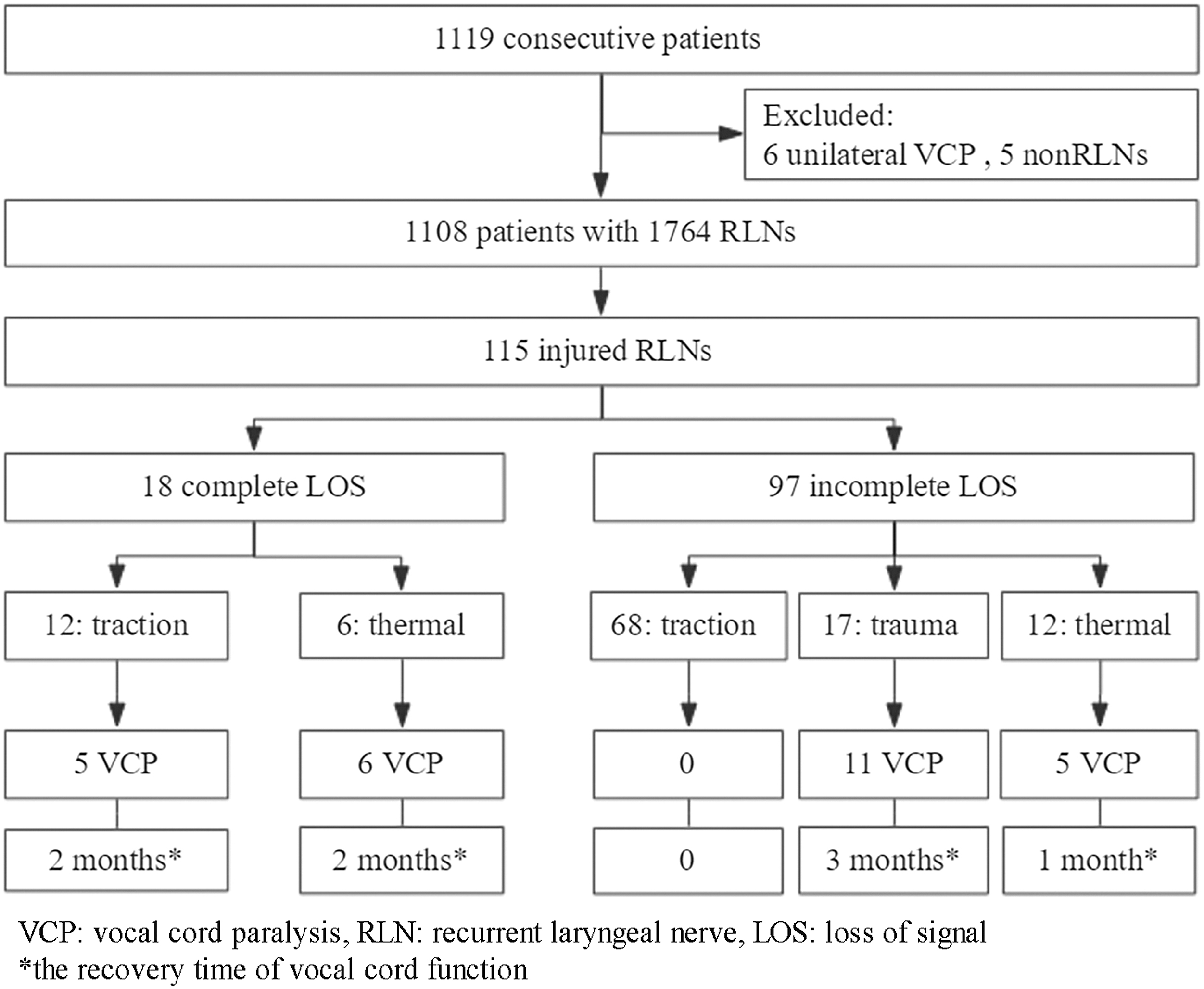
The study flow chart.
Complete dissection of the RLNs was performed in all patients, and the mean distance between the R2p and R2d was 3.8 (3.1–5.5) cm. In this study, 45 (2.6%) of 1764 nerves experienced a true episode of complete LOS during the surgery (Table 2). Of these 45 nerves, 15 nerves had a complete amplitude recovery without an injury detected on the exposed RLN at the end of the operation, and all had normal vocal cord function after surgery, 12 nerves had a partial recovery with a weakened RLN area detected, and 3 of these developed temporary VCP, 18 nerves had persistent LOS (no recovery) with an injury detected before closing the wound, and 11 of these developed temporary VCP.
Correlation between the reduction of the R2p/R2d ratio and postoperative vocal cord function
Among the 1764 nerves, the percentages of EMG amplitude reduction ranged from 21% to 84% comparing the amplitude between the distal and proximal ends of the injured area. Of the 18 RLNs with complete LOS (final vagal signal, R2 < 100 μV) before closing the wound, temporary VCP was found in 11 cases (61.1%). Among the 97 RLNs with incomplete LOS (reduction of the R2p/R2d ratio 21–84%; R2 153–765 μV), 16 cases (16.5%) developed VCP, and the reduction of the R2p/R2d ratio ranged from 63% to 84%, while the remaining 81 cases with a R2p/R2d ratio <63% (R2 231–1876 μV) all showed normal vocal cord function (Fig. 3). Five of the 16 nerve injuries were caused by usage of EBD adjacent to the nerve with thermal injury; normal vocal cord mobility returned ∼1 month after the operation in these cases. The remaining 11 nerve injuries that were caused by trauma functioned well ∼3 months after the operation. Eleven of the 18 nerves with complete LOS developed temporary VCP and recovered within 2 months after operation. In the 1649 RLNs without an identified injury and without a significant reduction of the EMG amplitude, 3 nerves (0.2%) developed postoperative VCP but vocal cord function recovered well in all cases within 1 month postoperatively. Thus, there were 30 nerves (1.7%) that developed temporary VCP and no permanent VCP occurred in the 1764 nerves.
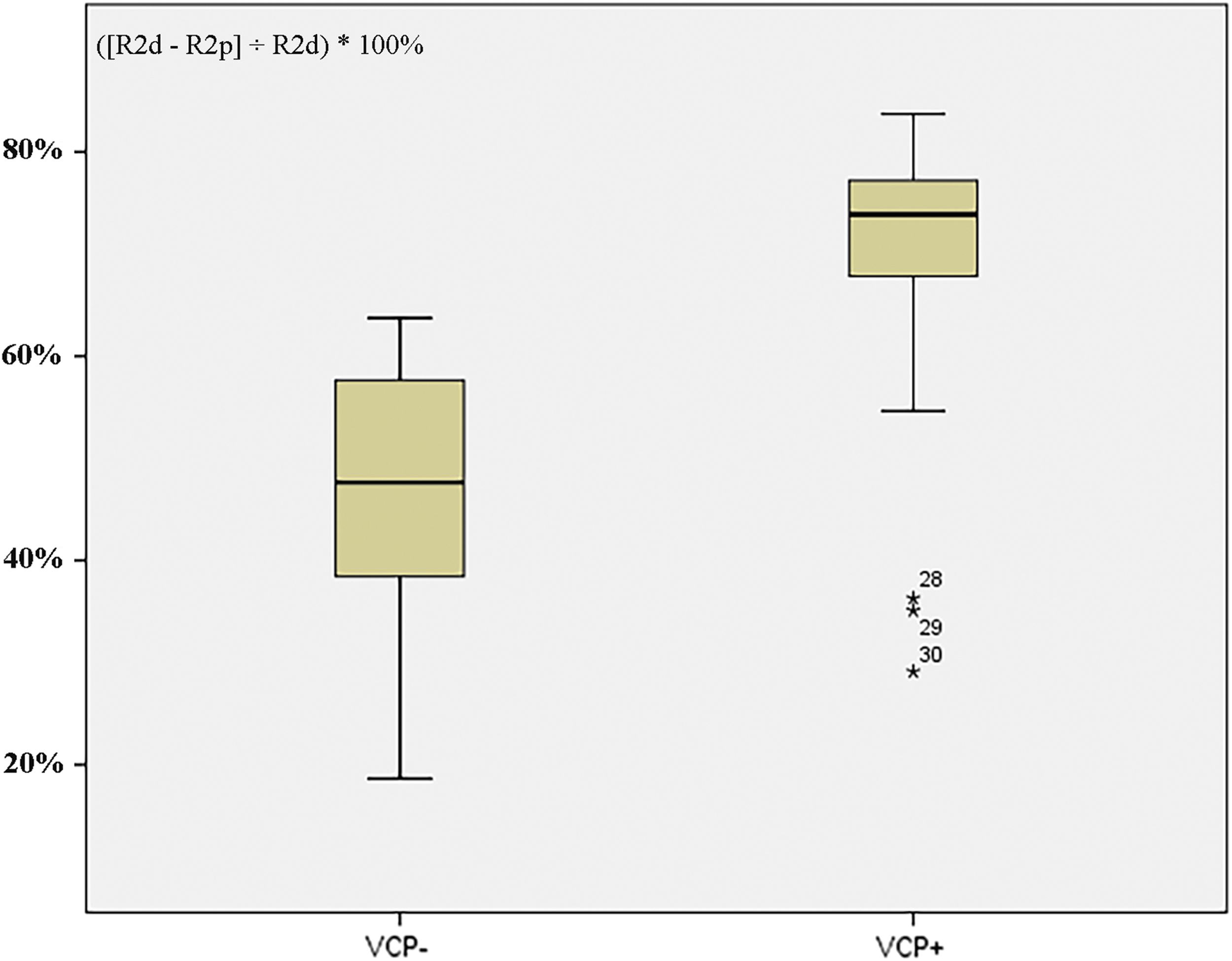
Reduction in R2p/R2d ratio in patients with and without VCP. The reduction of R2p/R2d ratio was calculated as ([R2d − R2p]/R2d) × 100%. VCP+, patients with vocal cord paralysis; VCP−, patients without vocal cord paralysis.
Cutoff criteria for VCP
In this study, 1764 R2p and R2d values have been used to determine the threshold value, and 30 (1.7%) of these 1764 nerves developed postoperative temporary VCP. Using the area under the curve (AUC) for ROC analysis, the cutoff value of percentage reduction of the amplitude of the R2p/R2d ratio to predict postoperative vocal cord dysfunction was 63% (Fig. 4). The true positive (LOS with post-VCP), FP (LOS without post-VCP), true negative (normal EMG signal without post-VCP), and false negative (FN) (normal EMG signal with post-VCP) of patients with the reduction of R2p/R2d >63% (incomplete LOS) or R2 < 100 μV (complete LOS) were 27, 7, 1727, and 3, respectively. Sensitivity, specificity, PPV, and negative predictive value (NPV) of patients with the reduction of R2p/R2d >63% (incomplete LOS) or R2 < 100 μV (complete LOS) were 90.0%, 99.8%, 79.4%, and 99.8%, respectively.
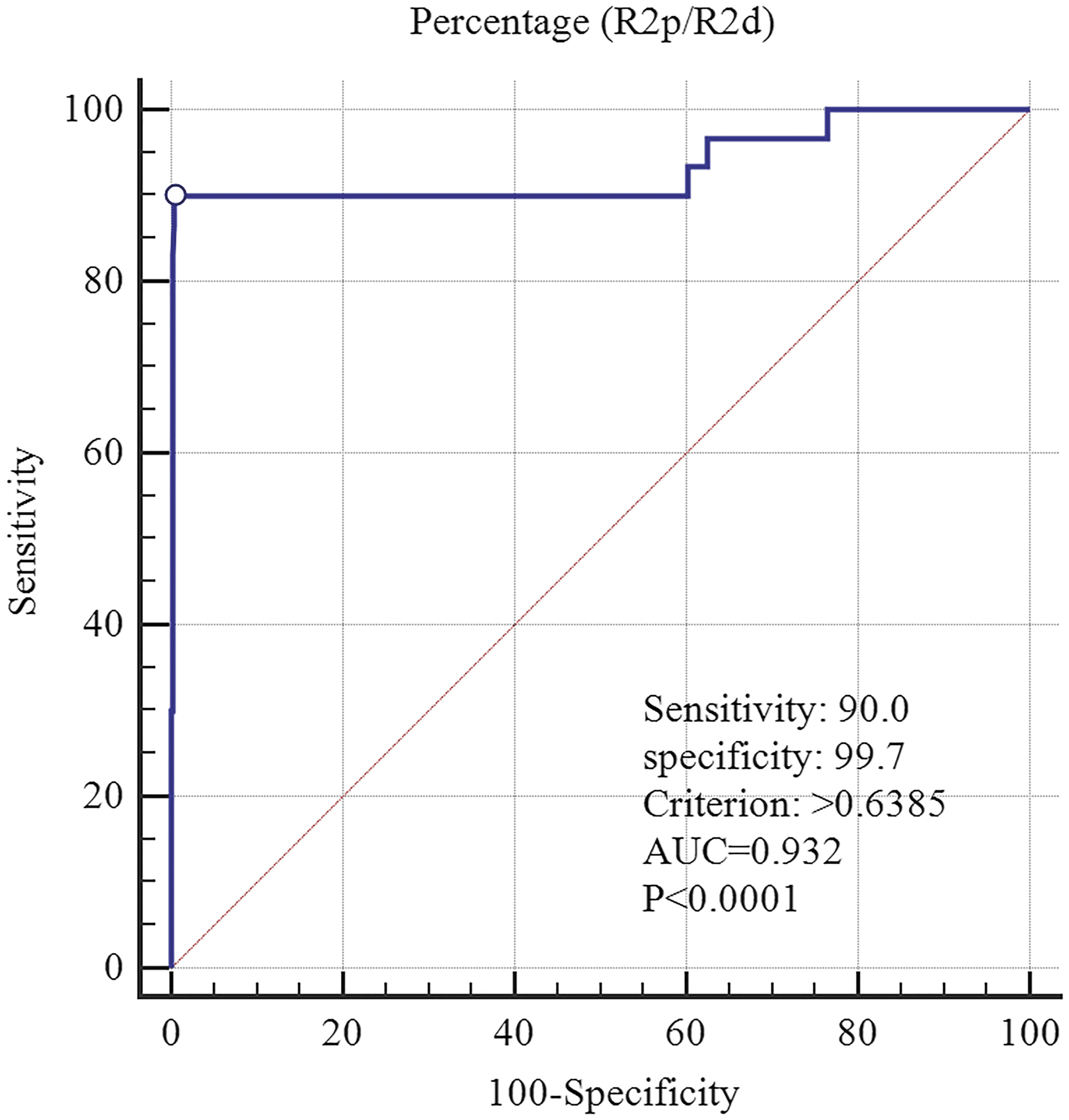
ROC curve at 63% amplitude percentage reduction of R2p/R2d. The percentage reduction of R2p/R2d was calculated as ([R2d − R2p]/R2d) × 100%. ROC, receiver operating characteristic.
Discussion
IONM is an adjunct tool for early identification and functional evaluation of RLN during thyroid and other neck surgeries (24). However, the correlation between amplitude and vocal cord function remained unclear. Based on the four-step procedure of IONM (V1-R1-R2-V2), at the end of the operation, complete LOS (absolute threshold value <100 μV) often indicates postoperative VCP. However, criteria forewarning incomplete LOS have not been clearly delineated (12). The relative threshold value of the R2p/R2d ratio was proposed as a warning criterion to exclude bias from the baseline and stability of the evoked EMG signal response by Wu et al. for the prediction of vocal cord dysfunction (14). In this validation study with a larger cohort, we routinely tested and compared the EMG signals from the lowest proximal end (R2p signal) to the most distal end at the laryngeal entry point (R2d signal) of the exposed RLN (Fig. 1). We also checked the whole exposed RLN to pinpoint the injured area if the R2p/R2d reduction reached >20%.
Testing and comparing the R2p and R2d signals is a simple and useful procedure to evaluate RLN neurophysiologic injury after its dissection, and predicts VCP. In this study, we prospectively collected the data from 1764 nerves in a single institution to test and compare the R2p and R2d signals. One hundred fifteen injured RLNs with LOS were identified by the reduction of the R2p/R2d ratio with segmental type 1 injury, which might have not been identified if only standardized procedures were applied in this study. During the detection of the RLN, checking the exposed RLN from the lowest proximal end (R2p signal) to the most distal end near the laryngeal entry point (R2d signal) was useful to pinpoint the injured area of the nerve and elucidate the mechanism, distinguishing segmental type1 from global type 2 injuries. All the complete and incomplete LOS nerves in this study could be localized with an injury point (LOS type 1). However, the reported proportion of type 2 lesions was 48.7% (56/115) in a multicenter pilot study by INMSG (15). Wu et al. found that the two types of injury mechanisms, segmental type 1 and global type 2, could only be applied to the cases of “complete LOS” (14).
Monitoring with a positive response provides formal identification of the RLN. However, monitoring with a negative response does not equal to an injured nerve; some nerves with LOS may reflect a transient neuropraxia of short duration, and they may therefore regain signal before the end of the operation (2). A prospective observational study by Sitges-Serra et al. demonstrated that there was a 90% chance of intraoperative signal recovery after LOS of the RLN (5). Once the nerve was detected with complete LOS, 5 mL dexamethasone was used locally to soak the nerve. In this study, if there has been a problem with persistent complete LOS, the event threshold was turned up to 20 μV. With these settings, low-level EMG signals of the injured nerve <100 μV would trigger “evoked events” on the monitor. The triggered EMG signal of the 18 nerves with complete LOS ranged from 26 to 91 μV, and 7 of them showed normal postoperative vocal cords with EMG signals close to 100 μV.
When a reduced EMG signal was observed on initially operated side, some surgeons decide not to perform total thyroidectomy to avoid the risk of bilateral RLN injury. A questionnaire revealed that 93.5% of surgeons changed the resection plan for the other side during a bilateral thyroid surgery after LOS had occurred on the initially operated side (25). However, high FP rates indicate the need for internal review of clinical standards to avoid unnecessary two-stage thyroidectomy. Using AUC for ROC curve analysis, the cutoff value of the reduction of the amplitude of the R2p/R2d ratio to evaluate the postoperative laryngeal mobility is 63%. The ability of IONM to predict postoperative VCP was 79.4%. The high PPV of 79.4% indicates that the surgeon should consider that a certain degree of RLN injury has occurred, and that the possibility of postoperative VCP is 79.4%, even in cases with a persisting positive EMG response from the final RLN and vagal nerve stimulation.
These data might be very useful and helpful for decision making in patients in which a bilateral thyroid operation is planned. Wu et al. proposed three options for surgery on the contralateral side in the case of intraoperative LOS on the first operated side in a planned total thyroidectomy: (a) perform staged thyroidectomy, (b) perform subtotal resection on the contralateral side ventrally to the RLN plane at a safe distance from the nerve, and (c) perform total thyroidectomy as planned for advanced thyroid carcinoma (26). In this study, no staged thyroidectomy was performed and no permanent VCP occurred. Thirty nerves developed temporary VCP, and most of them recovered within 3 months. FN result was found in three RLNs (0.2%) showing no apparent EMG amplitude reduction but developing postoperative temporary VCP.
To correlate the final evoked EMG after stimulation of the RLN with immediate postoperative vocal cord function after thyroid surgery, Genther et al. reported a threshold value of 280 μV to assure postoperative vocal cord mobility and the risk of VCP with this value is ∼72% (27). Similarly, Pavier et al. concluded that with a threshold value of 200 μV, the risk of immediate postoperative VCP is ∼50% (28). However, the absolute threshold values could be influenced by the changed and unstable evoked EMG amplitude response, such as EMG tube position changes caused by traction or manipulation on the thyroid or trachea. Stopa and Barczynski identified not only an absolute threshold (189 μV, PPV: 77.4% NPV: 99.9%) but also a relative value (the reduction of V2 of >81.6% of V1, PPV: 76.6%, NPV: 99.8%) to define the risk of vocal cord palsy (29). In this study, we tested and compared the EMG signal reduction from the most distal and proximal ends of the RLN exposed during thyroidectomy (R2p and R2d) at the end of surgery. Compared with the reduction of R2/R1, the bias from the baseline amplitude change can be excluded by comparing the R2p signal with the R2d signal. When the percentage reduction of the amplitude of the R2p/R2d ratio was >63%, the PPV and accuracy of the method for predicting postoperative VCP were 79.4% and 99.4%, respectively. This information is especially useful for cases in which bilateral thyroid surgery is being considered.
This is a single tertiary referral center validation study, and the results might be affected by the surgical techniques used and the specific system monitoring the electrophysiological activity of the RLN. Therefore, this IONM protocol requires a learning curve to be applied and replicated in nontertiary referral centers where the surgeons might not have the same degree of expertise in thyroid surgery and the use of neuromonitoring. Our study concentrated on specific EMG parameters, amplitude, and threshold. Among the EMG parameters, latency is the other useful variable in nerve monitoring. However, it was not recorded in our intermittent IONM. Continuous IONM was applied in our institution to investigate the effectiveness of concordant amplitude and latency changes (combined events) during thyroidectomy (30).
Conclusion
Based on the four-step standardized IONM procedures, determining R2p-R2d is useful and could be applied in routine thyroidectomies with IONM. This validation study has confirmed that testing the exposed RLN at the lowest proximal end (R2p signal) and the most distal end near the laryngeal entry point (R2d signal) is a simple and useful procedure not only to detect neurophysiologic RLN injuries and to elucidate the mechanism of nerve injury but also to predict vocal cord function. A 63% difference in proximal to distal amplitude was significant and associated with a PPV of 79.4% for vocal cord dysfunction.
Footnotes
Acknowledgments
The authors thank the study patients for their willingness to participate in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.