
Abstract
Background:
Serum thyroglobulin (Tg) is used in the follow-up of patients with differentiated thyroid cancers (DTC), but the presence of antithyroglobulin antibodies (TgAbs) makes Tg measurements unreliable. TgAb decline after total thyroidectomy and persistent/increasing levels may indicate cancer persistence/recurrence. Hence, we aimed to determine whether TgAb might be a reliable prognostic marker for DTC.
Methods:
We conducted a meta-analysis and systematic review. A comprehensive literature search was performed to identify studies of patients with DTC with known TgAb status and prognostic outcomes in five databases (Medline, Embase, PubMed, Google Scholar, and Scopus). We used a random-effects model to calculate pooled odds ratios (ORs) and 95% confidence intervals (CIs) for TgAb status and its association with DTC prognosis.
Results:
After analysis of 34 studies, we found that TgAb+ patients have a higher risk of lymph node metastasis (OR = 1.18 [CI 1.47–2.25]) and cancer persistence/recurrence (OR = 2.78 [CI 1.55–4.98]) than TgAb− patients. However, no significant differences in mean/median tumor size, risk of extrathyroidal extension, tumor multifocality, and cancer mortality were found between the two groups. In a comparison of TgAb trends, patients with persistent/increasing TgAb levels were found to have a higher risk of cancer persistence/recurrence (OR = 9.90 [CI 4.36–22.50]) and cancer mortality (OR = 15.18 [CI 2.99–77]) than patients with decreasing TgAb levels.
Conclusions:
TgAb positivity and persistent/increasing trends were associated with compromised DTC prognosis. These results suggest that TgAb may be used as a prognostic marker in the follow-up of patients with DTC.
Introduction
Differentiated thyroid cancer (DTC) accounts for only 1% of all cancers but are the most common endocrine malignancies. DTC has several subtypes, among which papillary thyroid cancers (PTCs) account for 85% of cases, follicular thyroid cancers (FTC) and Hürthle cell thyroid cancers (HCC) together account for 12%, and poorly differentiated cancers account for <3% (1). DTCs retain characteristics of thyroid follicular cells, including the expression of thyroglobulin (Tg), which serves as a useful tumor marker in the follow-up of patients with DTC (2). Tg levels should decrease or become undetectable after treatment; if Tg levels increase or remain high, the cancer is suspected to be persisting or recurring (3). Twenty percent of the population with DTC is positive for thyroglobulin antibodies (TgAb), whose presence may result in inaccurate Tg measurements. Thus, TgAb testing has expanded from being used to test thyroid autoimmunity to being ordered concurrently with Tg levels to rule out the presence of TgAb interference (2,4). The utility of TgAb in determining DTC prognosis has only recently been recognized, as studies have shown that after total thyroidectomy, TgAb gradually declines, whereas an increasing or a persistent high level may indicate cancer persistence or recurrence (4,5). Therefore, in this study, we aimed to determine whether TgAb might be a reliable prognostic marker for the follow-up of patients with DTC, especially in TgAb+ patients, via conducting a meta-analysis and systematic review.
Methods
We conducted a meta-analysis and systematic review of observational studies to assess the prognostic significance of TgAb status in patients with DTC according to the PRISMA Statement (6).
Literature search strategy
We searched articles in four electronic databases (Medline, Embase, PubMed, Google Scholar, and Scopus) with no limit placed on publication dates and languages up to January 2020. The search terms used included “anti-thyroglobulin antibody” OR “anti-thyroglobulin” OR “thyroglobulin autoantibodies” AND “prognosis” AND “papillary thyroid cancer” OR “papillary thyroid carcinoma” OR “follicular thyroid cancer” OR “follicular thyroid carcinoma” OR “Hürthle cell thyroid cancer” OR “Hürthle cell thyroid carcinoma” OR “differentiated thyroid cancer” OR “differentiated thyroid carcinoma.” We also manually searched the reference lists from eligible studies and clinical reviews and included additional references identified in the reference lists.
Inclusion criteria
We included studies that satisfied the following inclusion criteria: (i) primary studies with full text available, not just abstracts; (ii) studies classifying TgAb status with ± trends; (iii) studies using a comparator antibody group; (iv) studies with known patient numbers in each classified antibody group; (v) studies with available or complete prognostic data of interest; and (vi) studies associating TgAb status with DTC prognosis.
Data extraction
Microsoft Excel was used to extract the following information from eligible studies: (i) first author's last name; (ii) publication year; (iii) study type; (iv) study temporal direction (retrospective or prospective); (v) country; (vi) pre/postoperative TgAb measurements; (vii) population type; (viii) age; (ix) follow-up period; (x) total number of patients with DTC studied; (xi) number of patients with DTC in TgAb± trend groups; (xii) mean/median tumor sizes in TgAb± groups; (xiii) extrathyroidal extension in TgAb± groups, (xiv) tumor multifocality in TgAb± groups; (xv) lymph node metastasis in TgAb± groups; (xvi) cancer persistence/recurrence in TgAb± trend groups; and (xvii) cancer mortality in TgAb± trend groups. Some authors were contacted to request or clarify their study data before the information was included in our data sheet. The extracted data were further confirmed by other authors (S.E. and G.D.E.).
Quality assessment
The Newcastle–Ottawa scale (NOS) was used to assess the risk of bias in the included studies. The NOS score consists of three domains examining studies on the basis of participant selection, comparability, and outcome/exposure. Three NOS assessment forms were used to assess cohort, case–control, and cross-sectional studies (Supplementary Figs. S1, S2, S3) (7,8).
Statistical analysis
The pooled odds ratio (ORs) and 95% confidence intervals (CIs) were calculated with a random-effect model to assess the effect of TgAb status on risk estimates of extrathyroidal extension, tumor multifocality, lymph node metastasis, cancer persistence/recurrence, and cancer mortality (9). Heterogeneity was assessed with the I2 statistic, and I2 values of 25%, 50%, and 75% were considered to indicate low, moderate, and high levels of heterogeneity, respectively (10). Publication bias was assessed quantitatively with Egger's regression model; a p-value <0.05 was considered to indicate publication bias (11). Independent sample t-test was performed to compare the mean/median tumor sizes between TgAb+ and TgAb− patients with DTC.
Results
Study selection
According to Figure 1, 34 studies were selected from the identified 643 records for our meta-analysis after exclusion of duplicate studies (n = 288), studies with irrelevant abstracts (n = 274), and studies not satisfying the inclusion criteria (n = 47).

Flowchart illustrating selection of studies.
Study characteristics
Table 1 shows the characteristics of the 34 eligible studies. These studies were conducted in various geographical regions and included 15 studies assessing European populations, 12 studies assessing Asian populations, 3 studies assessing North American populations, 1 study assessing a South American population, and 3 studies assessing Middle Eastern populations. In terms of study types, 27 were cohort studies, 4 were case–control studies, and 3 were cross-sectional studies. The DTC subtypes in these studies included PTC, FTC, and HCC, and PTC was the most commonly studied malignancy. Sample sizes ranged from 17 to 1240, and ages ranged from 8 to 89 years. The follow-up periods were as early as immediately after the thyroidectomy up to 11.6 years after the thyroidectomy. Surgical parameters (e.g., tumor size, extrathyroidal extension, tumor multifocality, and lymph node metastasis) and/or long-term outcomes (e.g., cancer persistence/recurrence and cancer mortality) were explored across studies. According to the NOS scores listed in Table 1, both cohort and cross-sectional studies were higher in quality than case–control studies. The detailed distribution of scores across NOS domains is shown in Supplementary Tables S1, S2, S3.
Characteristics of the 34 Eligible Studies
DTC, differentiated thyroid cancer; EE, extrathyroidal extension; F, follicular; H, Hurtle cell; LN, lymph node metastasis; MF, tumor multifocality; NA, not applicable; NOS, Newcastle–Ottawa scale; P, papillary; persist, cancer persistence; recurr, cancer recurrence; TgAb, thyroglobulin antibody.
TgAb status and tumor sizes
Using independent sample t-test, we analyzed four (12 –15) and two studies (16,17) for the association of TgAb positivity with mean and median tumor sizes, respectively. According to Tables 2–3, the combined mean tumor sizes in 513 TgAb+ and 3077 TgAb− patients were 1.85 and 1.77 cm, respectively, and there was no significant difference between groups (p = 0.91). The combined median tumor sizes in 250 TgAb+ and 1063 TgAb− patients were 1.65 and 2 cm, respectively, and there was no significant difference between groups (p = 0.65).
Thyroglobulin Antibody Positivity and Tumor Sizes
Mean (standard deviation) in centimeters.
Thyroglobulin Antibody Positivity and Tumor Sizes
Median (range) in centimeters.
TgAb positivity and extrathyroidal extension
Four studies were included in our meta-analysis to examine the association between TgAb positivity and risk of extrathyroidal extension in patients with DTC (12,15,17,18). According to Supplementary Figures S4 and S5, 50% of 555 TgAb+ patients developed extrathyroidal extension, compared with 46% of 2751 TgAb− patients. However, the forest plot in Figure 2 did not indicate a significant difference in the risk of extrathyroidal extension between TgAb+ and TgAb− patients (OR = 1.17 [CI 0.76–1.81], p = 0.47). There was no evidence of publication bias shown in Egger's regression model, p = 0.51 (Fig. 2). There was a moderate level of heterogeneity (Fig. 2).

TgAb positivity and risk of extrathyroidal extension. Forest plot illustrating individual (black square) and pooled (gray diamond) OR and CI. CI, confidence interval; OR, odds ratio; TgAb, thyroglobulin antibody.
TgAb positivity and tumor multifocality
Four studies were included to examine the relationship between TgAb positivity and risk of tumor multifocality in patients with DTC (12,15,17,19). According to Supplementary Figures S6 and S7, 45% of 560 TgAb+ patients had multifocal tumors, compared with 34% of 2733 TgAb− patients. However, the forest plot in Figure 3 did not indicate a significant difference in the risk of tumor multifocality between TgAb+ and TgAb− patients (OR = 1.46 [CI 0.99–2.17], p = 0.06). There was no evidence of publication bias shown in Egger's regression model, p = 0.06 (Fig. 3). There was a moderate level of heterogeneity (Fig. 3).
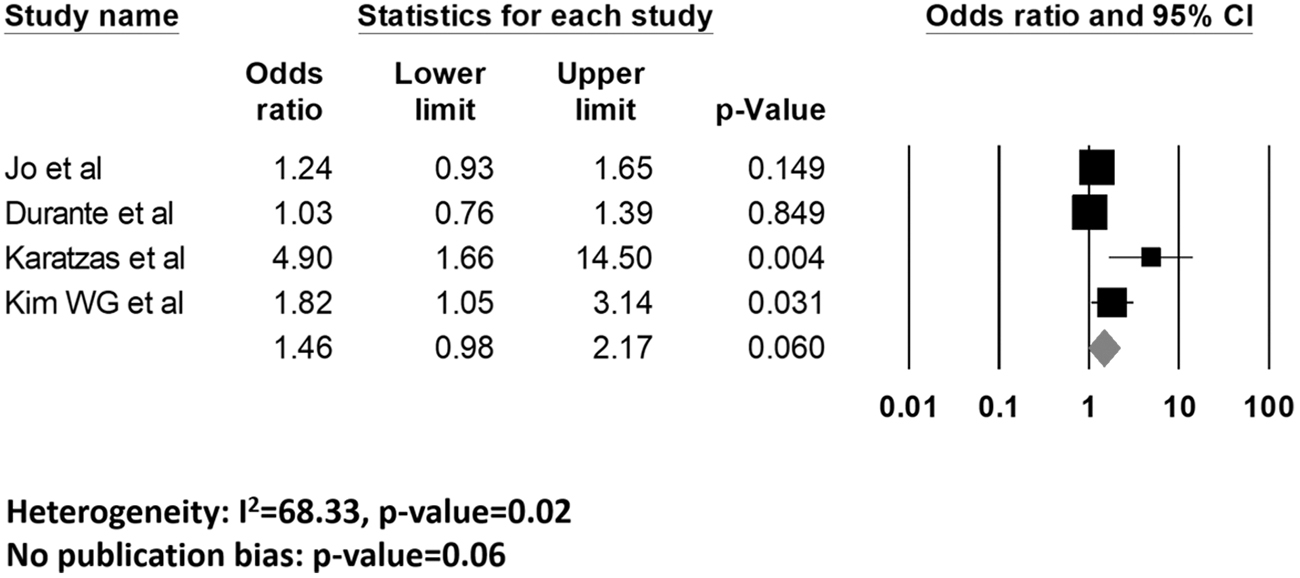
TgAb positivity and risk of tumor multifocality. Forest plot illustrating individual (black square) and pooled (gray diamond) OR and CI.
TgAb positivity and lymph node metastasis
Eleven studies were included to examine the association between TgAb positivity and risk of lymph node metastasis in patients with DTC (12,14 –23). According to Supplementary Figures S8 and S9, 50% of 1251 TgAb+ patients developed lymph node metastases, compared with 34% of 4955 TgAb− patients. This finding was concordant with the forest plot in Figure 4, in which TgAb+ patients were found to have a significantly higher risk of developing lymph node metastasis than TgAb− patients (OR = 1.81 [CI 1.47–2.25], p < 0.001). There was no evidence of publication bias in Egger's regression model, p = 0.08 (Fig. 4). There was a moderate level of heterogeneity (Fig. 4).
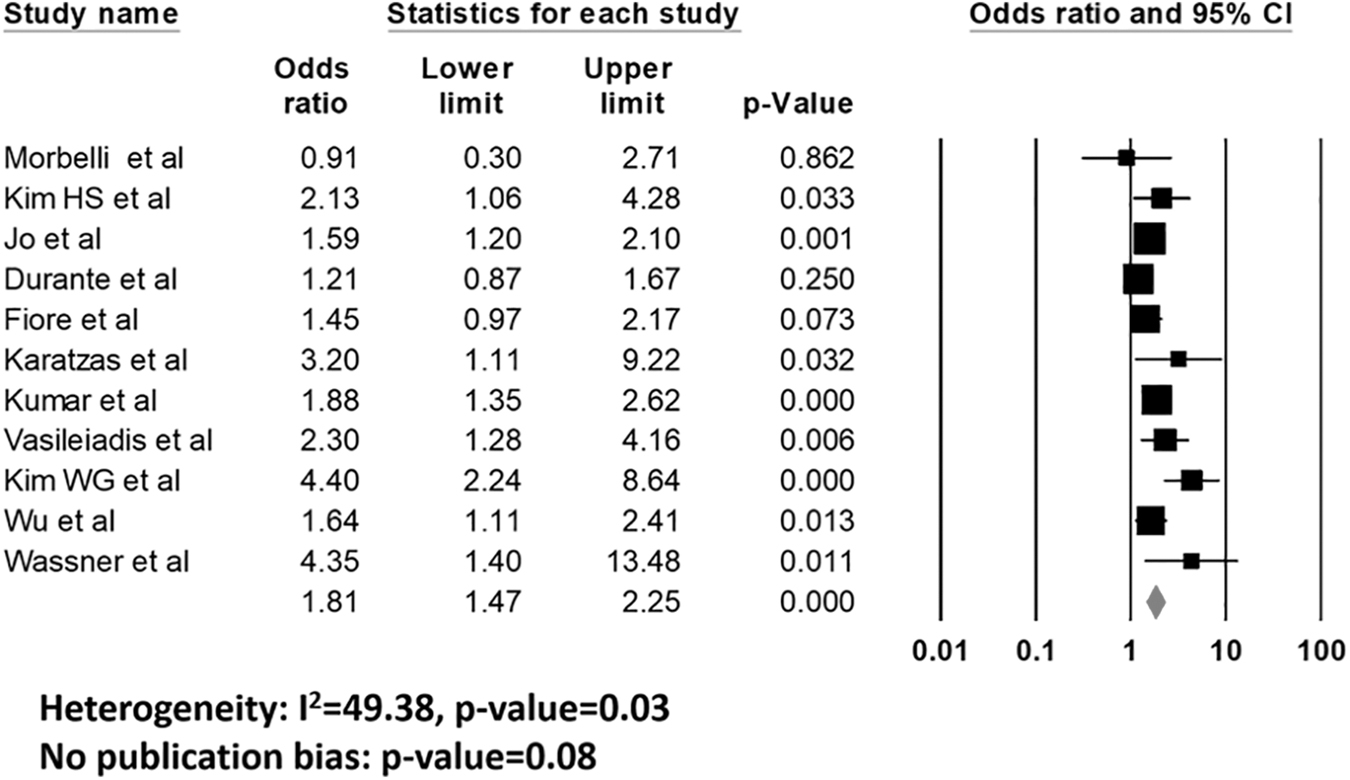
TgAb positivity and risk of lymph node metastasis. Forest plot illustrating individual (black square) and pooled (gray diamond) OR and CI.
TgAb positivity and cancer persistence/recurrence
Eighteen studies were included in our meta-analysis to examine the association between TgAb positivity and cancer persistence/recurrence in patients with DTC (5,12,13,15 –17,24 –35). As shown in Supplementary Figures S10 and S11, 27% of 1336 TgAb+ patients developed cancer persistence/recurrence, compared with 12% of 6343 TgAb− patients. This finding was concordant with the forest plot in Figure 5, in which TgAb+ patients were found to have a significantly higher risk of developing cancer persistence/recurrence than TgAb− patients (OR = 2.78 [CI 1.55–4.98], p = 0.001). There was no publication bias in Egger's regression model, p = 0.23 (Fig. 5). There was a high level of heterogeneity (Fig. 5).

TgAb positivity and risk of cancer persistence/recurrence. Forest plot illustrating individual (black square) and pooled (gray diamond) OR and CI.
TgAb positivity and cancer mortality
Two studies were included in our meta-analysis to examine the association between TgAb positivity and cancer mortality in patients with DTC (13,25). According to Supplementary Figures S12 and S13, 8% of 137 TgAb+ patients died from cancer, compared with 4% of 1284 TgAb− patients. However, the forest plot in Figure 6 did not show a significant difference in the risk of cancer mortality between TgAb+ and TgAb− patients (OR = 1.76 [CI 0.85–3.66], p = 0.13) (Fig. 6). There were an inadequate number of studies available for publication bias assessment. There was no evidence of heterogeneity.

TgAb positivity and risk of cancer mortality. Forest plot illustrating individual (black square) and pooled (gray diamond) OR and CI.
TgAb trend and cancer persistence/recurrence
Thirteen studies were included in our meta-analysis to examine the association between TgAb trend and cancer persistence/recurrence in patients with DTC (22,25,27,32,36 –44). According to Supplementary Figures S14 and S15, 45% of 299 patients with persistent/increasing TgAb levels developed cancer persistence/recurrence, compared with 8% of 1058 patients with decreasing TgAb levels. This finding was concordant with the forest plot in Figure 7, in which patients with persistent/increasing TgAb levels had a significantly higher risk of cancer persistence/recurrence than patients with decreasing TgAb levels (OR = 9.90 [CI 4.36–22.50], p < 0.001). There was evidence of publication bias, p = 0.03 (Fig. 7). We therefore used the fail-safe methods to estimate the number of potential missing studies needed to significantly change the conclusion of our findings. This analysis showed that, to nullify our estimated effect size, 234 studies with nonsignificant findings would be needed (45). In view of the fact that there have been no more than 34 studies published over the past 26 years, it is highly improbable that such a large number of similar studies would have gone unpublished or have been missed by our extensive search strategy. There was a moderate level of heterogeneity.

TgAb trend and risk of cancer persistence/recurrence. Forest plot illustrating individual (black square) and pooled (gray diamond) OR and CI. The Matrone et al. (44) study was not found in the forest plot as none of the DTC patients developed cancer persistence/recurrence in both the TgAb trend groups.
TgAb trend and cancer mortality
Three studies were included in our meta-analysis to examine the association between TgAb trend and cancer mortality in patients with DTC (25,37,39). According to Supplementary Figures S16 and S17, 17% of 52 patients with persistent/increasing TgAb levels died from cancer, compared with 1% of 252 patients with decreasing TgAb levels. This finding was concordant with the forest plot in Figure 8, in which patients with persistent/increasing TgAb levels were at significantly higher risk of cancer mortality than patients with decreasing TgAb levels (OR = 15.18 [CI 2.99–77.00], p = 0.001). There was no evidence of publication bias shown in Egger's regression model, p = 0.34 (Fig. 8). There was no heterogeneity (Fig. 8).

TgAb trend and risk of cancer mortality. Forest plot illustrating individual (black square) and pooled (gray diamond) OR and CI.
Discussion
TgAb status and DTC prognosis
Although our study shows that TgAb+ patients showed poorer results for all surgical parameters in absolute numbers, only the risk of lymph node metastasis was significantly (approximately two times) higher in TgAb+ patients. Our study also shows that those patients who were TgAb+ were almost three times more likely to have a cancer persistence/recurrence. Dynamic prognostic factors such as TgAb trends have been shown in some studies to be superior to static prognostic factors in terms of monitoring disease progression (46). Therefore, our meta-analysis also included studies that evaluated TgAb trends and their influence on DTC prognosis. We noted that patients with persistent/increasing antibody levels were at ∼10 and 15 times higher risk of cancer persistence/recurrence and cancer mortality, respectively. This finding may be explained by the increasing Tg antigenic stimulus via increasing Tg levels, stimulating an immune response in terms of TgAb expression from plasma cells (2). Therefore, decreasing antibody levels after thyroidectomy ± radioiodine therapy are expected, whereas positivity or persistent or increasing antibody levels may suggest cancer persistence/recurrence.
Several studies also assessed the prognostic values of the degree of change in TgAb levels (e.g., decrease by ≤50% or ≥50%) (5,15,25,27,36,39,41,42). Hence, additional analyses were conducted in this group of studies. We found that patients with decreasing TgAb levels of ≤50% were at significantly higher risk of cancer persistence/recurrence than patients with decreasing TgAb levels of ≥50% (OR = 4.32 [CI 2.14–8.73], p < 0.001) (Supplementary Fig. S18). Although there was no significant difference in the risk of cancer persistence/recurrence between patients with increasing TgAb levels of ≤50% and ≥50% (OR = 0.58 [CI 0.11–2.98], p = 0.51), there were only two studies with small sample sizes included in the analysis (Supplementary Fig. S19). These findings would be important because further stratifying patients according to the degree of change in TgAb levels may facilitate triage and guide management of patients with DTC.
Autoimmune thyroid disease and DTC
Because TgAbs highly correlate with lymphocytic thyroiditis, one possible reason for the controversy regarding the prognostic significance of TgAb is the failure to differentiate between diffuse infiltration by lymphocytes (a hallmark of Hashimoto's thyroiditis) and peritumoral lymphocytic infiltration (a hallmark of the immune response against tumors), which could influence DTC prognosis differently (47 –49). A role for the above mechanisms is further suggested by a study by Latrofa et al. (50) reporting different epitope specificities for TgAbs in patients with PTC with or without autoimmune thyroid disease (ATD). On the basis of these previous findings, we decided to perform an additional analysis assessing TgAb status and DTC prognosis in studies that accounted for ATD. With adjustment for ATD, we found that TgAb+ patients with ATD have larger tumor sizes (Supplementary Table S4) and higher risks of extrathyroidal extension, tumor multifocality, lymph node metastasis, and cancer persistence/recurrence compared with TgAb+ patients without ATD (Supplementary Figs. S20, S21, S22, S23). This result is consistent with findings from previous studies suggesting that patients with DTC with Hashimoto's thyroiditis are at higher risk of developing bilateral and multifocal tumors (20,47,51 –53), lymph node metastasis (20,22), and they tend to have higher cancer stages (53). The lymph node metastasis risk in TgAb+ patients with DTC might be explained by TgAbs being markers of ATD, and patients with DTC with ATD having poorer prognosis. Another possible reason for the lymph node metastasis risk in TgAb+ patients with DTC may be due to node sampling, because ATD results in more enlarged lymph nodes (54); these enlarged lymph nodes would be more likely to be dissected and hence more likely to result in detection of neoplastic cells.
Strengths and limitations
Follow-up period
Previous studies have reported that a transient increase in TgAb levels during the early post-treatment period might be due to an immune response secondary to the release of antigenic Tg from thyroidal tissue after surgery ± radioiodine therapy (55,56). Because all the retrospective studies in our meta-analysis had an adequate follow-up period of ≥1 year to evaluate long-term outcomes (e.g., cancer persistence/recurrence or mortality), the results reported here are more likely to have some prognostic significance and it is less likely that the observed trends are solely due to iatrogenic trauma to the thyroidal tissue.
Sample sizes
Data regarding TgAb trends and DTC prognosis generally have smaller sample sizes than the rest of the data. The inclusion of 12 studies assessing TgAb trends and cancer persistence/recurrence (Fig. 7) provided 2715 patients to assess, which is excellent and provided reasonable statistical power to detect small differences. Furthermore, a meta-analysis assessing TgAb trends and cancer mortality included three studies with a combined sample size of 457 patients with DTC (Fig. 8). These studies provided consistent data with no heterogeneity and were able to detect large statistically significant effect sizes (Figs. 7 and 8) (57).
Heterogeneity
Most of our data have moderate to high levels of heterogeneity for the following possible reasons: (i) variability in TgAb measurement kit sensitivities, specificities, and cutoff values for TgAb positivity; (ii) multiple assays used in the same study period; (iii) variability in outcome assessment criteria; and (iv) populations of different geographical locations. Some data relating TgAb status and cancer mortality (Figs. 6 and 8) did not display any evidence of heterogeneity, thus further emphasizing the influence of the outcome assessment criteria on result heterogeneity, because there is no variability when assessing cancer deaths. To address the heterogeneity, we performed additional meta-analyses, which excluded studies that used older agglutination (22) and multiple assays (17,26,29,32,37,41,42) in the same study period. Despite the above changes, we did not detect major changes in the heterogeneity and risks of extrathyroidal extension (postexclusion: I 2 = 78.11, OR = 1.17 vs. initial: I 2 = 72.29, OR = 1.17), tumor multifocality (postexclusion: I 2 = 70.08, OR = 1.84 vs. initial: I 2 = 68.33, OR = 1.46), lymph node metastasis (postexclusion: I 2 = 45.69, OR = 1.97 vs. initial: I 2 = 49.38, OR = 1.81), cancer persistence/recurrence in patients with TgAb positivity (postexclusion: I 2 = 90.73, OR = 3.33 vs. initial: I 2 = 89.16, OR = 2.78), and cancer persistence/recurrence in TgAb trend (postexclusion: I 2 = 52.93, OR = 4.60 vs. initial: I 2 = 52.42, OR = 7.41) (Supplementary Figs. S24, S25, S26, S27, S28).
Publication bias
Publication bias from the TgAb trend and cancer persistence/recurrence data may have been due to an outlier estimate from the study by Trimboli et al. (25), in which the OR for cancer persistence/recurrence in patients with persistent/increasing TgAb levels was much higher (OR = 240.00 [CI 23.34–2468.03]) than in other studies (Fig. 7). After excluding the study by Trimboli et al. (25) from our meta-analysis (Supplementary Fig. S29), we found that the publication bias was eliminated and that patients with persistent/increasing TgAb levels were still at higher risk of cancer persistence/recurrence, although the pooled OR decreased from 9.90 to 7.41. We verified and found no errors in the data extraction and analysis of the study by Trimboli et al. (25).
Other assessments
Most of the studies included in our meta-analyses were retrospective in nature; retrospective studies are considered inferior to prospective studies in terms of their level of evidence. Furthermore, the calculated OR values from individual studies were derived from univariate analyses, and 23 of the total 34 eligible studies did not adjust for age and/or sex, thus potentially suggesting the presence of other confounding factors that might influence DTC prognosis.
Conclusions
Overall, DTC has a good prognosis, but the prognosis may be more limited in the presence of recurrent and distant metastasis. Our analysis indicates that TgAb dynamics may be used as a prognostic tool in TgAb+ patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Figure S9
Supplementary Figure S10
Supplementary Figure S11
Supplementary Figure S12
Supplementary Figure S13
Supplementary Figure S14
Supplementary Figure S15
Supplementary Figure S16
Supplementary Figure S17
Supplementary Figure S18
Supplementary Figure S19
Supplementary Figure S20
Supplementary Figure S21
Supplementary Figure S22
Supplementary Figure S23
Supplementary Figure S24
Supplementary Figure S25
Supplementary Figure S26
Supplementary Figure S27
Supplementary Figure S28
Supplementary Figure S29
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4