
Abstract
Background:
Although thyrotropin (TSH) receptors are found in many nonthyroid tissues, we know little about the direct action of TSH on these receptors. Patients after total thyroidectomy for differentiated thyroid cancer (DTC) provide an interesting model for studying this issue. The administration of exogenous TSH in patients with an established thyroid state on levothyroxine (LT4) treatment allows us to study the effect of elevated TSH concentrations independent of thyroid status on the function of various organs, including the kidneys. The aim of this study was to assess the effects of the administration of recombinant human TSH (rhTSH) on renal perfusion and glomerular filtration in this group of patients.
Methods:
The study included 24 patients after total thyroidectomy due to DTC, without concomitant diseases, receiving only LT4 who qualified for radioiodine treatment (RIT). For two consecutive days, the patients received rhTSH and subsequently the RIT. Clinical and biochemical evaluation of thyroid and renal function was carried out before and 24 hours after the second dose of rhTSH and before the RIT. On the sixth day of hospitalization, the patients' glomerular filtration rate was re-evaluated. Kidney perfusion was assessed using color Doppler ultrasound imaging before and 24 hours after the second dose of rhTSH and before the RIT.
Results:
The administration of rhTSH to patients after total thyroidectomy due to DTC caused significant deterioration of renal perfusion after the second dose of rhTSH before the RIT, which was followed by a significant reduction in glomerular filtration. Furthermore, rhTSH did not significantly affect the hemodynamic parameters that could worsen renal function.
Conclusions:
This study indicates that TSH alone, independent of thyroid hormone concentrations, can influence renal perfusion and renal function.
Introduction
Thyroid dysfunction affects the function of many organs, including the kidneys. Hypothyroidism reduces reabsorption of sodium and calcium in renal tubules and decreases free water clearance; it also reduces renal plasma flow (RPF), renal blood flow (RBF), and glomerular filtration rate (GFR) (1 –6). As a result, prolonged hypothyroidism can lead to impaired renal function and be associated with the development of chronic kidney disease (CKD) (7). However, hyperthyroidism increases tubular reabsorption of sodium and calcium, increases free water clearance, RPF, and RBF, and elevates GFR (8 –10).
Several large cross-sectional studies in various populations have demonstrated a relationship between elevated thyrotropin (TSH) concentrations and decreased GFR and/or a higher prevalence of CKD (11 –17). These observations apply to both subclinical and overt hypothyroidism, as well as to situations with variation in TSH within the reference range. It has also been shown that levothyroxine (LT4) treatment of hypothyroidism improves renal function or attenuates declines in GFR (18 –20).
However, no specific causal link between hypothyroidism and CKD development has been found. For example, Chen et al. did not find any common genetic markers of hypothyroidism and CKD (21). Moreover, in one recent study of more than 70,000 patients, a higher incidence of CKD in hypothyroidism was not proven, suggesting that the relationship found in observational studies may result from a higher prevalence of elevated TSH in patients with underlying impaired renal function (22). As a consequence, questions on the relationship of hypothyroidism and elevated TSH to renal function remain open.
While the above observations refer to the influence of altered free thyroid hormone concentrations on the kidneys, they serve to raise questions about a possible independent direct effect of TSH alone on peripheral tissues, including the kidneys. Such effects would be mediated by TSH receptors (TSH-Rs) that have been found not only on thyroid cell membranes but also on adipocytes, fibroblasts, osteoclasts, leukocytes, monocytes, and interestingly, myocytes of the heart, endothelial cells, and smooth muscle cells of vessels (including the glomerular arteriole) (23 –28). Little is known about the functional role of these receptors outside their role in the thyroid gland.
Ippolito et al. demonstrated that recombinant human TSH (rhTSH) could improve coronary flow during cold pressure tests (CPT) in patients after thyroidectomy due to differentiated thyroid cancer (DTC), thereby improving coronary reserve, perhaps in a vascular endothelium-dependent mechanism (29). Some studies have reported a significant relationship between TSH and changes in GFR, independent of alterations in free thyroid hormone concentrations (30 –32). Higher TSH values have also been shown, even within the reference range, to relate to an increased resistance of the afferent glomerular arteriole and thus with decreased RPF, RBF, and GFR (33). However, evidence of a direct effect of TSH on renal function has not yet been shown.
Patients after total thyroidectomy for DTC represent an interesting model in which to observe a direct impact of TSH on peripheral tissues. The administration of exogenous rhTSH in thyroidectomized patients with an established thyroid state during LT4 treatment allows us to assess the direct influence of elevated TSH concentration on the function of peripheral organs, including the kidneys.
Thus, the aim of this study was to assess renal perfusion and GFR, before and after administration of exogenous TSH, in patients after total thyroidectomy for DTC without concomitant cardiovascular, metabolic, or kidney diseases.
Patients and Methods
Study population
Twenty-four consecutive patients (5 males, 19 females; age 35.6 ± 9.1 years) after total thyroidectomy for DTC admitted to the Endocrinology and Radioisotope Therapy Department of the Military Institute of Medicine were included in the study. The study was approved by the Bioethics Committee of the Military Institute of Medicine. All patients received information about the study and subsequently provided their informed consent to participate. All patients had a history of DTC with low or intermediate risk of recurrence, according to the American Thyroid Association (ATA) guidelines (34). All patients received LT4 treatment in doses dependent on their DTC risk, according to the ATA guidelines. Rigorous selection was carried out to exclude any factors affecting blood flow, renal perfusion, and glomerular filtration.
The exclusion criteria were age <18 and >55 years, obesity, or any history of smoking (now or in the past), arterial hypertension, CKD, diabetes, arrhythmias, myocardial infarction, ischemic heart disease, heart failure, stroke, urinary tract infection, hypercholesterolemia, hypertriglyceridemia, liver disease, vegetarian diet, infections, insulin resistance, pregnancy, and taking medicines other than LT4. Obesity was defined as a body mass index (BMI) >30 kg/m2 and hypertension as systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg. CKD was excluded based on history, serum creatinine (Cr) concentration, estimated GFR based on the Modification of Diet in Renal Disease Study Group (MDRD) formula, and urinary albumine to creatinine ratio (UACR) (35).
Heart and coronary diseases were excluded based on history, electrocardiogram, and N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) concentration; stroke, based on history; and urinary tract infections, based on clinical symptoms and urinalysis. Hypercholesterolemia was defined as total cholesterol >200 mg/dL and/or low-density lipoprotein (LDL)-cholesterol >130 mg/dL and hypertriglyceridemia as triglycerides >165 mg/dL. Liver disease was excluded based on history, transaminase, and albumin concentrations, and infections were excluded based on history, physical examination, and measurement of highly sensitive C-reactive protein (CRP-hs) concentration. Insulin resistance was assessed as homeostasis model assessment index, according to the homeostasis model of insulin resistance: insulinemia (mIU/L) × glycemia (mg/dL)/405 (36).
Study protocol
One to three months after their thyroidectomies, the participants were admitted to the Endocrinology and Radioisotope Therapy Department for radioisotope treatment with radioiodine (RAI). Patients received intramuscular rhTSH at a dose of 0.9 mg to assess the stimulated concentrations of thyroglobulin (Tg) for two consecutive days (the first and second day of hospitalization).
At admission, the following parameters were measured: TSH, free thyroxine (fT4), free triiodothyronine (fT3), Tg, antithyroglobulin antibodies (TgAb), as well as all the necessary parameters and tests for exclusion from the study, including Cr, CRP-hs, NT-pro-BNP, glucose, insulin, albumin, transaminase, total cholesterol, LDL-cholesterol, triglycerides, urinalysis, and albumin and Cr concentration in the urine. BMI was calculated from patient's weight and height. TSH, fT3, fT4, and Cr concentrations were measured again 24 hours after the second dose of rhTSH (on the third day). Stimulated Tg was determined on the fifth day, and Cr was measured again at discharge on the sixth day of hospitalization. Estimated GFR was based on the MDRD formula (35). LT4 treatment was continued at an unchanged dose during hospitalization.
Ultrasound examinations of the kidneys were performed at admission, before administration of the first rhTSH dose (on the first day), and 24 hours after the second dose of rhTSH (on the third day). Blood pressure and heart rate (HR) were measured directly before each ultrasound examination. All patients received RAI 24 hours after the second rhTSH dose, on the third day of hospitalization after second blood sampling and second ultrasound examination with a mean activity of 95.6 ± 14.23 mCi (3.53 ± 0.52 GBq) and within a range of 78.7–129.5 mCi (2.91–4.79 GBq).
Biochemical assessment of thyroid function
Fasting blood for serum TSH determination was collected from the forearm veins between 7:30 and 8:30 a.m., after an overnight rest. TSH concentrations were measured using the electrochemiluminescence immunoassay (ECLIA) method (Cobas e601 analyzer; Roche), with a sensitivity of ≥0.014 μIU/mL and a reference range of 0.4–4.2 μIU/mL. fT4 and fT3 concentrations were also measured using the ECLIA method, with a sensitivity of ≥0.3 and ≥0.4 pmol/L, respectively, and a reference range of 12–22 and 3.2–6.9 pmol/L, respectively. The Tg and TgAb concentrations were measured using the ECLIA, with a sensitivity of ≥0.04 ng/mL and ≥10 IU/mL, respectively, and a reference range of 1–77 ng/mL and 0–115 IU/mL, respectively.
Ultrasound examination
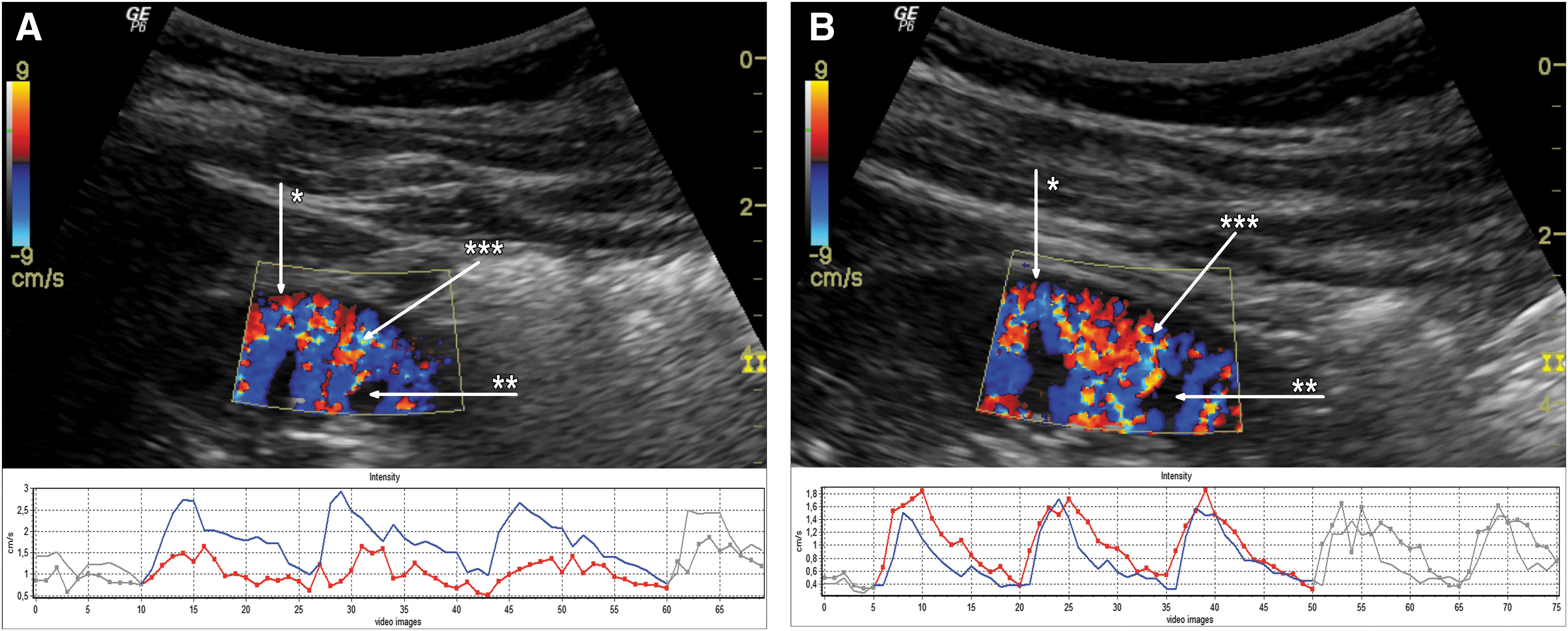
Ultrasound color Doppler imaging (Logiq P6; GE Healthcare, Seoul, Korea)—with a curved array probe of 2–5 MHz—of renal cortex perfusion was performed in the middle segment of the right kidneys, in a manner previously described (37 –39). Video clips 3–5 seconds long were recorded in DICOM (Digital Imaging and Communications in Medicine) format with color Doppler perfusion and were evaluated using external software (PixelFlux; Chameleon Software, Leipzig, Germany). Renal cortical perfusion (RCP) as a mean value of arterial and venous flow intensity was estimated (40). Only measurements performed in the same renal cortical segment and with the same color Doppler frequency, gain, and velocity scale, and subsequently verified by an independent investigator were considered for comparative analysis (Fig. 1A, B).
Blood pressure measurement
An Omron 705IT (Omron Corporation, Kyoto, Japan) was used for blood pressure estimation. Measurements were performed on the left arm, just before each of the ultrasound examinations.
Hemodynamic parameters
The mean arterial pressure (MAP) was calculated according to the formula:
where DBP is diastolic blood pressure and SBP is systolic blood pressure.
The pulse pressure (PP) was calculated as the difference between the SBP and DBP:
The rate pressure product (RPP) was calculated as the product of SBP and HR:
Statistical analysis
To examine the possible effect of the thyroid state on RCP changes due to the TSH injection, patients were divided into Group 1 (n = 18) with a baseline TSH concentration <0.4 μIU/mL (patients with suppressive doses of LT4) and Group 2 (n = 6) with a baseline TSH of 0.4–4.0 μIU/mL (patients with supplementary doses of LT4).
Correlations between variables were analyzed using Pearson's or Spearman's test, depending on the type of data distribution. Differences between dependent variables were analyzed with the use of the appropriate parametric t-test or the nonparametric Wilcoxon test. Differences between groups were analyzed with the t-test or the Mann–Whitney U test. Stepwise multivariable linear regression analysis was used to identify factors independently associated with the change in RCP.
Results
Results are presented as means with standard deviation. Baseline clinical, demographic, and anthropometric characteristics of the examined population are presented in Tables 1 and 2. As a result of the exclusion criteria, no patient was obese, and no one had an infection, hyperglycemia, hyperinsulinemia or insulin resistance, hypercholesterolemia, or hypertriglyceridemia. Baseline serum TSH, fT4, and fT3 concentrations were all within the reference ranges.
Baseline Characteristics of the Study Population
Reference values used by local laboratory unit.
ALT, alanine transaminase; AST, aspartate transaminase; BMI, body mass index; CRP, C-reactive protein; HOMA-IR, homeostasis model assessment of insulin resistance; LDL, low-density lipoprotein; M, men; NT-pro-BNP, N-terminal pro-B-type natriuretic peptide; SD, standard deviation; TgAb, antithyroglobulin antibody; UACR, urinary albumin to creatinine ratio; W, women.
Comparison of the Results Before (Day 1) and After Thyrotropin Injection (Day 3)
DBP, diastolic blood pressure; fT3, free triiodothyronine hormone; fT4, free thyroxine hormone; HR, heart rate; MAP, mean arterial blood pressure; PP, pulse pressure; RCP, renal cortical perfusion; RPP, rate pressure product; SBP, systolic blood pressure; TSH, thyrotropin.
A comparison of results achieved before and 24 hours after the second rhTSH injection are shown in Tables 2 and 3. Intramuscular injection of rhTSH resulted in a significant decrease in RCP (0.798 ± 0.309 vs. 0.643 ± 0.259 cm/s; p < 0.001) accompanied by a marginally significant increase in Cr concentration (0.76 ± 0.12 vs. 0.78 ± 0.13 mg/dL; p = 0.066) and a decrease in GFR (100.8 ± 13.5 vs. 97.3 ± 13.7 mL/minute/1.73 m2; p = 0.096). In the extended observation of renal function at 96 hours after the second rhTSH injection, GFR was significantly reduced (100.8 ± 13.5 vs. 93.7 ± 12.1 mL/minute/1.73 m2; p < 0.001).
Comparison of the Renal Function Before (Day 1) and After Thyrotropin Injection (Day 3 and Day 6)
GFR, estimated glomerular filtration rate based on the Modification of Diet in Renal Disease Study Group formula; Group 1, patients with baseline TSH <0.4 μIU/mL; Group 2, patients with baseline TSH between 0.4 and 4.0 μIU/mL.
Administered activities of RAI did not correlate with GFR both from the third day (before RAI administration) (r = 0.164; p = 0.443) and the sixth day (three days after RAI administration) (r = 0.040; p = 0.858) and also with the decrease of GFR between third and sixth days (r = −0.328; p = 0.127). Quantifications of ultrasound color Doppler-coded perfusion of the renal cortex before and after TSH administration in a single patient are shown in Figure 1A and B. Quantifications of RCP for the entire investigated population before and after rhTSH administration are shown in Figure 2.
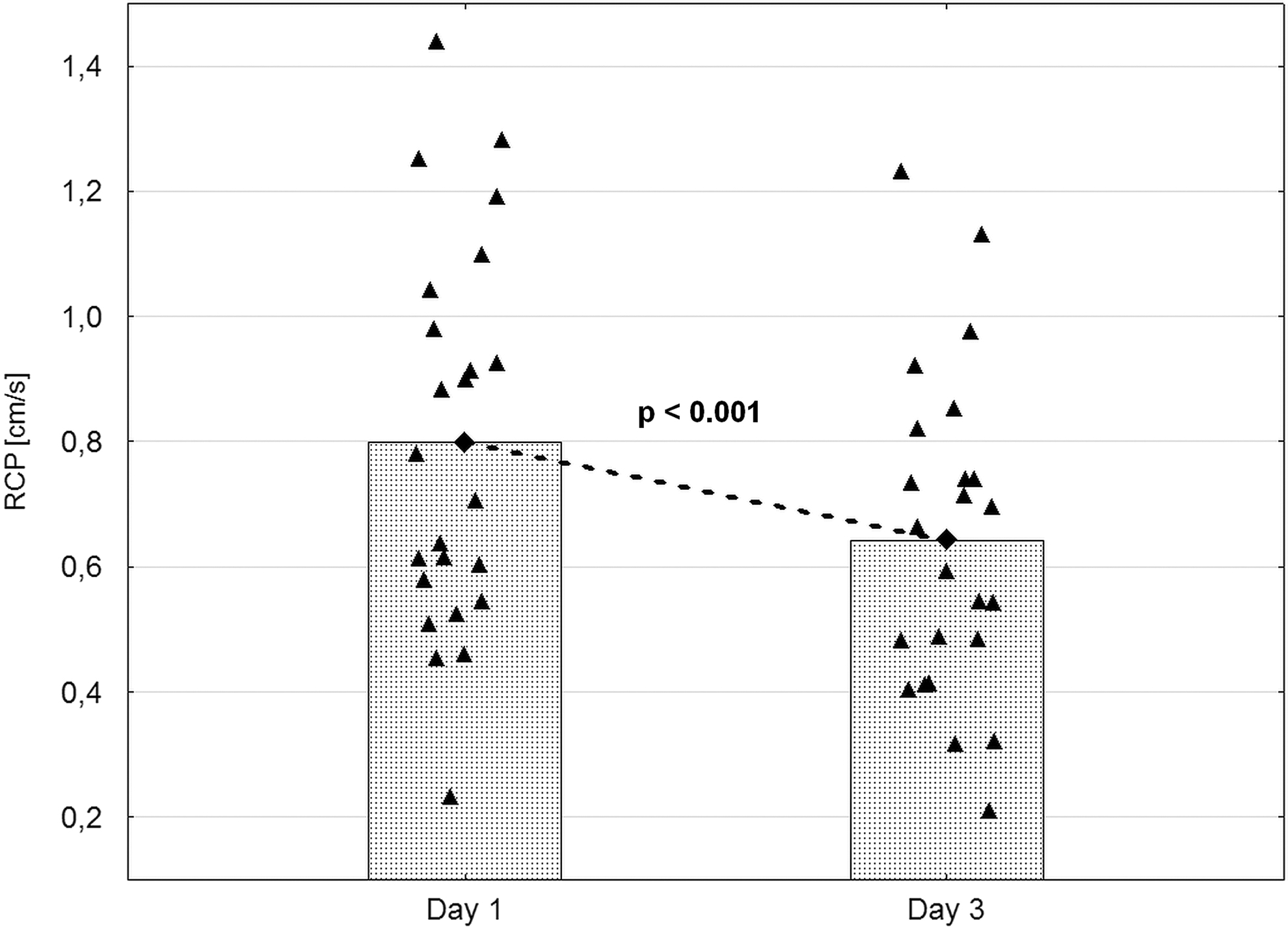
RCP before and after recombinant human TSH administration. ▴, single patient RCP; ♦ and columns, mean RCP; Day 1, before TSH injection; Day 3, 24 hours after the second TSH injection and before the radioiodine administration. RCP, renal cortical perfusion.
Twenty-four hours after the second rhTSH injection, PP, HR, and RPP were significantly higher (45.7 ± 10.8 vs. 51.4 ± 12.5 mmHg, p = 0.019; 70.3 ± 10.1 vs. 75.4 ± 11.6 beats per minute, p = 0.001; 8584.7 ± 1980.8 vs. 9373.6 ± 2149.8 mmHg/minute, p = 0.006, respectively). However, SBP, DBP, and MAP did not change. In the thyroid profiles after rhTSH injection, the expected increase in TSH concentration was observed, but also slight (within the reference range) decreases in fT4 (insignificant) (20.86 ± 2.48 vs. 19.70 ± 3.74 pmol/L, p = 0.083) and fT3 (significant) concentrations (5.04 ± 0.80 vs. 4.62 ± 0.77 pmol/L, p = 0.001).
A comparison subgroup analysis between patients with suppressive LT4 treatment (Group 1) and those with supplementary LT4 treatment (Group 2) revealed no significant differences between groups in the change in SBP, PP, HR, RPP, RCP, or GFR after TSH injection (Table 4), although DBP (−2.3 ± 8.8 vs. −5.2 ± 2.7 mmHg, p = 0.034) and MAP (−0.1 ± 8.5 vs. −4.4 ± 2.7 mmHg, p = 0.039) were slightly decreased in Group 2. Baseline concentrations of fT4 and fT3 also did not differ between these subgroups.
Comparison of Hemodynamic and Renal Changes Between Subgroups Differed in Baseline Thyrotropin Concentration
Δ, difference between day 1 and day 3 values (before and after recombinant human TSH injection).
An analysis of correlations performed for the entire investigated population showed a significant positive correlation only between the change in RCP and the change in GFR (r = 0.522; p = 0.004). Moreover, in the multivariable regression analysis considering significant changes in systemic hemodynamic parameters (HR, PP, and RPP), none of the parameters independently influenced the change in RCP. However, the change in renal function alone was independently and positively associated with the change in RCP (r = 0.564; R 2 = 0.318, p = 0.005).
Discussion
To the best of our knowledge, this may be the first study assessing the influence of TSH alone on renal function. With strict selection criteria, we excluded patients with factors that could affect blood flow, renal perfusion, and glomerular filtration. In patients after total thyroidectomy after rhTSH injection, we observed a significant deterioration in renal perfusion, which was followed by a significant reduction in glomerular filtration. Moreover, rhTSH had no effect on hemodynamic parameters, such as SBP, DBP, or MAP. Based on these results, it would appear that kidney function abnormalities may result from the direct action of TSH on the kidneys and not indirectly from hemodynamic changes.
A slight increase in PP, HR, or myocardial work (RPP) should improve blood flow, renal perfusion, and GFR, but not cause deterioration of renal function, as observed in our study. Similarly, discrete fT3 changes within the reference range do not significantly affect perfusion and renal function. This was confirmed by the regression analysis, in which GFR was the only factor independently associated with renal perfusion changes. In addition, any effect of “thyroid status” on renal dysfunction was ruled out by comparing subjects subgrouped by having either suppressed or normal TSH levels. The two groups did not differ significantly in regard to free thyroid hormone concentrations, hemodynamic changes, or in changes in renal parameters after rhTSH administration.
There has been a relative dearth of research on an exclusive influence of TSH on renal function in the literature. However, with evidence of TSH-Rs in different cells and tissues outside the thyroid gland, the functional role of these receptors remains to be determined (23 –28). Tsuda et al. showed in 26 patients with normal renal function that higher TSH concentrations, even within the reference range, were associated with lower RBF, RPF, and GFR and with higher resistance of the glomerular afferent (Ra) but not the efferent arteriole (Re) (33). Moreover, the positive relationship of TSH with Ra was independent of age and blood pressure, and free thyroid hormones did not significantly correlate with changes in renal parameters. Rather, TSH levels in those patients reflected functional thyroid status and depended on the concentration of free thyroid hormones, even within the reference range.
On the basis of their observations, it is therefore difficult to unambiguously infer an impact of TSH alone on glomerular hemodynamics. In contrast, the positive relationship of TSH with Ra is of great importance because it indicates a potential mechanism linking disorders of thyroid function and the kidneys. The present results are consistent with those of Tsuda et al. (33). In our different study model with patients after total thyroidectomy with an established thyroid state on LT4, exogenous TSH appears to adversely affect renal perfusion and glomerular filtration, perhaps through TSH-Rs located in the smooth muscle cells of glomerular afferent arteriole or other parts of renal glomeruli.
In similar studies, Duranton et al. observed reduced GFR after 4–12 weeks in thyroidectomized patients due to DTC, after injecting two doses of rhTSH (30). But their observations are difficult to interpret because this longer term renal function assessment was compared with GFR calculated 1 day after the second rhTSH dose and baseline GFR before rhTSH administration was not determined. As a consequence, the study results of Duranton et al. do not clarify how renal function might change shortly after rhTSH injection, compared with baseline renal function before rhTSH injection, although a clear and significant decrease in GFR was recorded in the long-term evaluation.
In our work, we evaluated GFR both before and twice after rhTSH administration—24 and 96 hours after the second rhTSH dose—observing a gradual decline in glomerular filtration. Nonetheless, the study by Duranton et al. complements our observations with a long-term GFR assessment and confirms a significant reduction in GFR after 4–12 weeks. In addition, our study suggests a potential mechanism for GFR decrease, that is, a significant reduction in renal cortex perfusion before GFR decline.
Similarly, Lee et al. measured potential alterations in serum Cr concentration by a study design protocol that differed from ours insofar as examining three time points and after a longer period. Their study times were at least 1 month before radioiodine treatment (RIT), on the day of RIT, and 3–6 months after RIT and found no differences in Cr concentration at the times examined (31). Thus, they could not evaluate the influence of rhTSH alone on Cr in the short-term period, as they did not measure Cr concentration just before rhTSH administration. Nevertheless, the results of Lee et al. are complementary to those of our study. They found no change in Cr concentration after rhTSH over a longer interval period (3–6 months), while we observed decreases of GFR in a short time frame evaluation (5 days).
Consequently, it is conceivable that the changes of GFR may be of transitory nature. Furthermore, in our study in patients with normal renal function, although significant, the changes were within the reference range. However, there is currently no better treatment regimen in these patients than rhTSH administration. Hormone withdrawal involves generating a hypothyroid state, which results in a more pronounced decrease of GFR and slower clearance of RAI. Thus, from the clinical point of view, we would conclude that there would be no need to avoid rhTSH in patients with normal renal function or stable CKD. However, whether these findings should prompt concern or consideration in patients with higher stages of CKD (G4, G5) or acute kidney injury remains to be determined.
In another study, Ippolito et al. demonstrated that rhTSH can improve coronary flow not at rest, but only after a CPT, presumably via a vascular endothelium-dependent mechanism, that is, a direct effect of TSH on vascular smooth muscle cells or endothelial cells of the coronary circulation (29). Interestingly, the authors did not observe a significant impact of rhTSH on hemodynamic parameters such as SBP, DBP, MAP, and HR, although myocardial work (RPP) significantly increased.
The data presented here are in general agreement with the observations of Ippolito et al. We also observed a significant increase in RPP after rhTSH administration but also a slight, but significant, increase in PP and HR, which could have influenced the RPP increase. However, even assuming that TSH may have an independent effect on various parts of the cardiovascular system and influence its hemodynamic parameters, the increase in RPP should result in a higher RBF and possibly an improvement in GFR, but our observations indicate the opposite. We found reduced renal perfusion after rhTSH administration and, consequently, deterioration of glomerular filtration on a subsequent evaluation.
Thus, the effect of injected TSH proved to be stronger on parameters of renal perfusion and glomerular hemodynamics than on any conceivably slight hemodynamic alterations in the cardiovascular system. These observations allow us to speculate that TSH, through its receptors in the smooth muscle cells of small renal vessels, reduces renal cortex blood flow and worsens glomerular filtration. In contrast to its possibly beneficial effect on coronary vessels, TSH may act in the opposite direction in the kidneys, perhaps by narrowing small renal vessels and thereby reducing perfusion and worsening renal function.
A limitation of our study is the relatively small number of patients. Similar- or even smaller-sized cohorts reported in the literature are likely to reflect the difficulty inherent in recruiting young nonobese patients after total thyroidectomy for DTC without concomitant diseases and medications (41). However, our rigorous inclusion criteria may override the relatively small sample size and the limitation that could derive from it.
It was pointed out that the extended third evaluation of GFR was performed three days after RIT and that some slight influence of RAI on glomerular filtration cannot be ruled out. RAI, like iodide, is freely filtered in the renal glomeruli and can be exchanged, for example, in the distal convoluted tubules via pendrin and probably via chloride channels and exchangers in different parts of the nephron (42 –46). But, there are still no data from clinical studies that relate to acute, delayed, or chronic influences of RAI on renal function. We also have no evidence of any significant renal RAI uptake during routinely performed nuclear medicine imaging.
In our study, the administered activities of RAI did not correlate with GFR both from the third day (before RAI administration) and the sixth day (three days after RAI administration) and also with the decrease of GFR between the third and sixth days. Finally, we observed a significant decrease in RCP after rhTSH but before RIT, with an independent and positive association exclusively of GFR with RCP in the regression analysis, which may indicate that altered RCP is responsible for the GFR impairment seen with extended evaluation.
A major strength of the present study is the use of an ideal model, which was developed after a rigorous selection process of patients without concomitant cardiovascular, kidney, liver and metabolic diseases, and medications, to show a possible direct impact of TSH on a normally functioning cardiovascular system and kidneys. Subjects were stratified in respect to whether they received supplemental or suppressive LT4 doses, and no differences were found in free thyroid hormone concentrations or significant hemodynamic parameters that could affect blood flow and renal perfusion (PP, HR, and RPP) between these two groups. Most importantly, there were no differences in RCP and GFR between the groups.
The importance of the presented study is the demonstration that TSH can directly and independently influence renal perfusion and function, without indirect action through free thyroid hormones. These effects are likely to be mediated through TSH-Rs localized in the smooth muscle cells of the small renal vessels, including glomerular arterioles, in the endothelial cells, glomerular mesangium, or renal tubular cells (47,48). Precise delineation of the mechanism(s) involved will require further research.
In conclusion, this study may have shown for the first time that TSH can directly and independently, without the contribution of free thyroid hormones, influence the perfusion and function of the kidneys. Furthermore, rhTSH did not significantly affect the hemodynamic parameters that could worsen renal perfusion and function.
Conceivably therefore, renal dysfunction in these patients may result from the direct action of TSH via the TSH-Rs localized in small renal vessels and different segments of renal glomeruli, independent of thyroid hormone concentrations and not indirectly via alterations in hemodynamics.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.