
Abstract
Background:
Although clinical studies indicate that thermal ablation is effective in treating low-risk papillary thyroid microcarcinomas (PTMCs), the effectiveness of this treatment in patients with low-risk PTMC has not yet been systematically evaluated.
Methods:
Ovid-MEDLINE and EMBASE databases were searched for studies published through May 1, 2019, which report the efficacy of thermal ablation in patients with low-risk PTMCs. Data were extracted and methodological quality was assessed independently by two radiologists according to PRISMA guidelines.
Results:
This systematic review identified 503 low-risk PTMCs in 470 patients treated by thermal ablation from 9 studies. During follow-up, no patient experienced local tumor recurrence or distant metastasis, whereas two patients (0.4%) experienced lymph node (LN) metastasis. One patient (0.2%) developed a new PTMC, which was successfully treated by additional ablation. Five patients (1.1%) underwent delayed surgery after ablation, including the two patients with LN metastasis and three additional patients with unknown etiology.
Conclusions:
Thermal ablation is an excellent local tumor control method in patients with low-risk PTMCs. Strict inclusion criteria and technical expertise are required to obtain favorable results.
Introduction
The incidence of papillary thyroid carcinoma (PTC) patients requiring subsequent surgery have markedly increased over the past 20 years. These increases are due primarily to the incidental detection of small subclinical PTCs and/or early ultrasound (US) screening (1 –3). The indolent characteristics of PTCs have reduced the need for immediate surgery, as surgery has several important drawbacks, including vocal cord paralysis, hypoparathyroidism, and postsurgical complications (4). Active surveillance (AS) is considered the alternative first-line option for patients with low-risk papillary thyroid microcarcinoma (PTMC), as it reduces overtreatment and unnecessary surgery, while showing favorable results, in these patients (5 –7).
Some patients with low-risk PTMCs undergoing AS may be concerned or anxious about the presence of cancer. Clinical trials have, therefore, evaluated thermal ablation of low-risk PTMCs, using methods such as radiofrequency ablation (RFA), laser ablation (LA), or microwave ablation (MWA) (8 –16). Although these thermal ablation methods have achieved good results with a low incidence of complications, inclusion/exclusion criteria and the completeness of treatment have varied (17,18). Therefore, a systematic evaluation about thermal ablation for low-risk PTMC is timely. This study, therefore, systematically reviewed the inclusion/exclusion criteria; efficacy of treatment; and rates of tumor recurrence, lymph node (LN) metastasis, distant metastasis, delayed surgery, and complications in patients undergoing thermal ablation for low-risk PTMC.
Materials and Methods
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (19).
Literature search
The MEDLINE and EMBASE databases were searched systematically to identify primary studies of patients with PTMC who were managed by AS. Search terms included ([thyroid microcarcinoma] or [papillary thyroid microcarcinoma] or [papillary microcarcinoma] or [primary papillary thyroid carcinoma] and ablation). All relevant studies published through May 1, 2019, were included. The bibliographies of relevant articles were searched to identify other appropriate articles.
Inclusion criteria
Studies were included if they (1) involved patients with low-risk PTMCs satisfying at least one of the following criteria: (a) greatest tumor dimension ≤10 mm; (b) diagnosis by cytology or biopsy; and (c) absence of LN metastasis, distant metastasis, and gross extrathyroidal extension; (2) included evaluation of efficacy after thermal ablation; and (3) contained results of histopathological tests as reference standards. In this study, thermal ablation included MWA, LA, and RFA.
Exclusion criteria
Studies or subsets of studies were excluded if they (1) were case reports or case series; (2) were letters, editorials, conference abstracts, systematic reviews/meta-analyses, consensus statements, guidelines, or review articles; (3) did not focus on the efficacy of thermal ablation for low-risk PTMCs; (4) included patients with tumors >1 cm in size despite focusing on the efficacy of thermal ablation for PTC; (5) were articles with, or suspected of having, overlapping populations; or (6) were articles without reference standards based on histopathological tests.
The literature search and selection were independently performed by two radiologists, S.J.C. and J.H.B., with 5 and 25 years of experience, respectively, in thyroid imaging.
Data extraction
The following data were recorded using standardized forms according to PRISMA guidelines (19): (1) article characteristics, including institution, country of origin, authors, year of publication, duration of patient recruitment, number of patients, mean patient age, male-to-female ratio, and study design (prospective or retrospective); (2) details of the included tumors, including the total number of ablated tumors, the criteria for ablation (summary of inclusion and exclusion criteria), tumor multiplicity, and the methods of confirming tumor diagnosis; (3) the details of thermal ablation, including ablation methods and devices, power output, applicator, mean ablation time, techniques used [local anesthesia, hydrodissection (20), the moving shot technique (21,22), track-back coagulation], minimum extent of the margins over the tumor margins covering the ablation area, and methods to evaluate the completion of ablation; (4) the results of ablation and details of follow-up (FU), including mean FU duration, serial changes in the size of the index tumor (before and immediately after ablation and at last FU, including the maximum diameter and/or volume, with volume (V) calculated using the equation: V = a × b × c × 0.524, where a is the maximum length, and b and c are the other two perpendicular diameters), tumor disappearance rate (both complete tumor disappearance or the presence of residual scar-like changes), the volume reduction rate (VRR) during FU calculated as ([initial tumor volume − final tumor volume] × 100)/initial tumor volume), mean tumor size at last FU (maximum diameter and/or volume), VRR at last FU, local tumor recurrence (appearance of viable tumor at or around the ablated lesion), a new tumor separate from the target tumor, LN metastasis, distant metastasis, number and causes of surgery during FU after ablation, and complications associated with ablation.
Complications were evaluated using the reporting standards of the Society of Interventional Radiology (23). Major complications were defined as adverse events associated with substantial morbidity or disability, an increased level of care, hospital admission, or substantial prolongation of hospital stay. Minor complications were defined as all other complications, and side effects defined as untoward consequences that did not require therapy or medical treatment, as well as undesired consequences of the procedure according to previous studies (24,25). However, the occurrences after ablation, including transient voice changes, minimal or asymptomatic hematoma, bleeding, and parenchymal edema, and tolerable mild pain or discomfort not requiring medication were regarded as neither complications nor side effects. Early complications were defined as those occurring within 30 days after ablation, and delayed complications were those occurring after 30 days (26).
Quality assessment
Two reviewers independently extracted data and assessed quality using the risk of bias for nonrandomized studies (RoBANS) tool for nonrandomized controlled trials (27,28).
Results
Literature search
The article selection process is described in detail in Figure 1. The initial systematic literature search identified 367 articles. After removing 27 duplicates, screening of the remaining 340 titles and abstracts yielded 16 potentially eligible articles. Searching the bibliographies of these articles identified one additional article (10). The full texts reviews of the 17 provisionally eligible articles found that 3 articles did not assess the efficacy of thermal ablation for low-risk PTMCs (17,18,29), 2 were case reports or case series (30,31), 2 included populations that overlapped or were suspected of overlapping (32,33), and 1 was a review article (34): these 8 articles were excluded. Although two studies included PTCs with longest dimension >10 mm, these studies were included because raw data for low-risk PTMCs were accessible (8,10). Some of the data not included in one of the original articles were supplied by its first author (S.Y. Jeong) (8). Finally, nine studies were included for qualitative synthesis in the current systematic review.

Flow diagram of the study selection process.
Characteristics of the included studies
Table 1 gives the detailed characteristics of the 9 included studies, involving 503 tumors in 470 patients. Four studies evaluated patients who underwent MWA (11 –14), three evaluated patients who underwent RFA (8,10,16), and two evaluated patients who underwent LA (9,15). The sizes of the study populations ranged from 4 to 185 patients, with the patients having mean ages of 42.2–70.8 years. Eight studies included more women than men (9 –16), whereas one did not (8). Seven studies were retrospective in design (8 –13,15), whereas the other two were prospective (14,16). The criteria for ablation were generally similar across the studies; these included low-risk PTMCs diagnosed by cytology or biopsy, the absence of LN or distant metastasis, the absence of imaging-based gross extrathyroidal extension, and ineligibility for surgery. Three studies included some patients with multiple tumors (12,13,16), whereas the 6 other studies involved only patients with single tumors (8 –11,14,15), with the number of tumors in the 9 studies ranging from 4 to 206. In the 2 studies using LA, tumors were confirmed by cytology (or fine needle aspiration [FNA]) (9,15); in 2 studies using MWA and 2 using RFA, tumors were confirmed by either core needle biopsy (CNB) or FNA (8,10,12,13); and in the other 2 studies using MWA and 1 study using RFA, tumors were confirmed by CNB (11,14,16). The 2 studies using LA excluded tumors with coarse calcifications or isthmic location (9,15), whereas the 7 other studies did not consider calcification or isthmic location as criteria excluding ablation (8,10 –14,16). The other detailed criteria for ablation are described in Table 1.
Characteristics of the Included Studies
Results of RFA in patients with low-risk PTMCs.
CNB, core needle biopsy; FNA, fine needle aspiration; LA, laser ablation; LN, lymph node; MWA, microwave ablation; NA, not available; Pro., prospective; PTC, papillary thyroid carcinoma; PTMC, papillary thyroid microcarcinoma ≤10 mm in greatest dimension; Retro., retrospective; RFA, radiofrequency ablation; RT, radiation therapy; US, ultrasonography.
Characteristics of the ablation methods
The detailed characteristics of the ablation methods are reported in Table 2. The mean ablation times were variable without tendency according to the type of ablation ranging from 165.9 to 500 seconds. In 5 studies, 2% lidocaine was used for local anesthesia (8,10,11,14,15), whereas the other 4 studies used 1% lidocaine (9,12,13,16). Three of 185 patients were converted to general anesthesia, 2 because they could not bear the pain of the intervention, and 1 because of a vasovagal reflex (13). Hydrodissection was not used in 2 studies (8,10), but was used in the other 7 on a case-by-case basis (9,11 –16). Hydrodissection was performed with lidocaine (1–2% lidocaine diluted 1:8 in normal saline) in 4 studies (9,11,14,15) and with normal saline in 3 studies (12,13,16). The moving shot technique was performed in 6 studies (8,10 –13,16), but details were not available for the other 3 studies (9,14,15). Two studies used a track-back coagulation technique at the final stage of ablation to prevent track seeding (11,14). The minimum covering ablation margin extent over the tumor margin was 5 mm in 4 studies using MWA and 1 using RFA (8,11 –14) and 1–2 mm in 1 study using LA (9), but details were not available for the other 4 studies (15,16). Seven studies used both conventional US and contrast-enhanced ultrasonography (9,11 –16), whereas two used conventional US and Doppler US (8,10) as conformation methods for completion of ablation.
Characteristics of the Ablation Methods
Original data communicated by the first author (S.Y. Jeong) of the study.
CEUS, contrast-enhanced ultrasonography; NA, not available; Nd-YAG, Neodymium yttrium–aluminum–garnet.
Results of ablation
The mean FU duration after ablation ranged from 7.8 months to >53 months (Table 3). The mean size of the index tumor before and immediately after ablation and at last FU ranged from 4.3 to 7.5 mm (41–157 mm3), 11.8 to 14.1 mm (517.6–3099.4 mm3), and 0 to 4 mm (0–70 mm3), respectively. Disappearance rates ranged from 33.7% to 100%. Although disappearance rate was defined as complete tumor disappearance or the presence of residual scar-like changes, the latter was not evaluated in four studies (8,11 –13). The VRR conversion period from negative to positive ranged from 1 to 3 months in 1 study (14), from 3 to 6 months in 3 studies (9,15,16), and from 6 to 12 months in 3 other studies (11 –13); this factor was not available in 2 other studies (8,10). The VRR at last FU ranged from 47.8% to 100%. No local tumor recurrence or distant metastasis was observed during FU. One study reported a new tumor separate from the primary ablated tumor, but this tumor disappeared completely 18 months after additional ablation (13). Two patients from 2 studies using LA showed LN metastasis: 1 patient out of 37 (2.7%) at 24 months after ablation (9) and 1 of 64 patients (1.5%) at 30 months after ablation (15). Both of these patients (9,15), and three patients from one another (14%) study for causes that are not specified (14), underwent delayed surgery during FU. There were no major complications in any of the included studies, with five studies reporting no significant complications. The rate of minor complications per tumor in the other four studies were 3.4%, 4.3%, 5.4%, and 19%, respectively, with the most common complication being transient hoarseness (11/15, 73.3%).
Results of Ablation
Including complete disappearance and residual scar-like change.
One of 64 (1.5%, 30 months after ablation due to LN metastasis).
One of 37 (2.7%, 24 months after ablation due to LN metastasis).
Three of 21 (14% with unclear etiology).
Cx., complication; FU, follow-up; LA, laser ablation; NA, not available; VRR, volume reduction rate.
Assessment of the study quality
Assessment of the qualities of the included studies according to RoBANS criteria (Fig. 2) showed that all nine studies had a low risk of bias in the selective reporting, incomplete outcome data, outcome data, measurement of exposure, confounding variables, selection of participants, and participant comparability domains. However, eight of the studies showed an unclear risk of bias in the blinding of outcome assessment domain, as they did not clearly report patient/investigator blinding (8 –15).
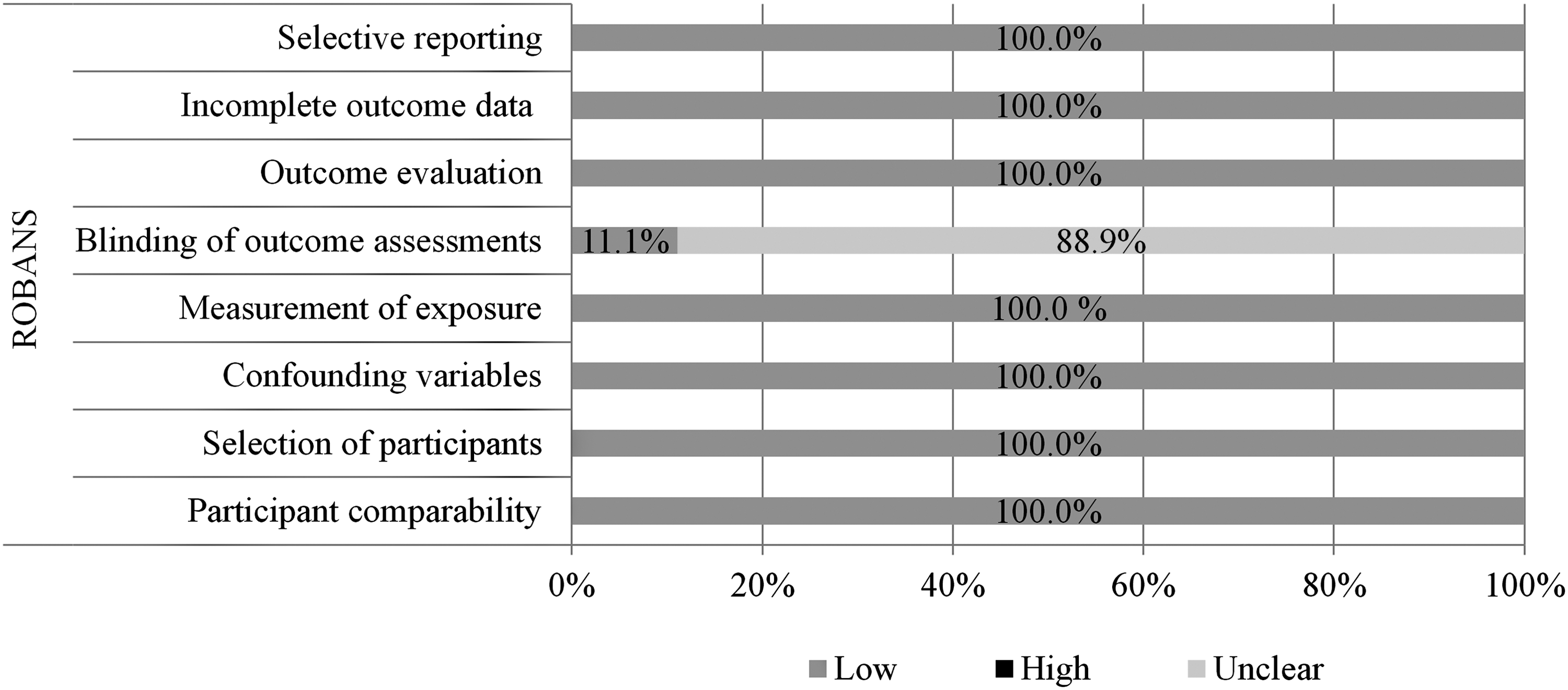
The quality assessment of the included studies according to the RoBANS. RoBANS, risk of bias for nonrandomized studies.
Discussion
This systematic review evaluated the efficacy and safety of thermal ablation of 503 low-risk PTMCs in 470 patients. None of these patients experienced local tumor recurrence or distant metastasis. However, two patients developed LN metastasis during FU. In addition, one patient developed a new cancer, which completely disappeared after additional ablation. Of the 470 patients, only 5 (1.1%) underwent delayed surgery after ablation, including the 2 patients with LN metastasis and 3 patients for reasons that were not specified. Therefore, this systematic review reveals that thermal ablation is a safe and effective local tumor control method for patients with low-risk PTMCs.
Incidental detection or US screening has resulted in marked increases in the incidence of PTC and the number of operations over the past 20 years (1 –3). Because immediate surgery has more disadvantages than advantages (4), AS has become the alternative first-line option for low-risk PTMCs and shows favorable results (5 –7). The 2015 ATA guidelines recommend AS for the first-line management of low-risk PTMCs (5). Based on this background, many trials have treated a small proportion of patients at high surgical risk and those who refuse to undergo surgery using thermal ablation techniques (8 –16). According to a recent systematic review and meta-analysis, AS shows acceptable size enlargement and LN metastasis during 5-year FU (pooled proportion of 5.3% and 1.6%, respectively). However, a large proportion (ranging from 8.7 to 32%) of patients underwent delayed surgery. Among them, a substantial proportion (ranging from 50 to 69%) of the reasons for delayed surgery were distinct from size enlargement or LN metastasis. We believe that anxiety is one of the main reasons for delayed surgery (35). In contrast, in this systematic review, we show that after thermal ablation, only two patients developed LN metastasis without local tumor recurrence or distant metastasis. Moreover only 1.1% of patients in this study underwent delayed surgery after thermal ablation, with none undergoing delayed surgery because of the patient's anxiety about tumor progression. By treating the primary tumor, thermal ablation may alleviate or eliminate patient anxiety.
A recent study showed results conflicting with those of this systematic review (18). That study described the results in 12 patients with PTCs who underwent thermal ablation followed by surgery. Postsurgical results were unsatisfactory, with residual tumor in 11 patients and multifocality in 9 patients. Nine patients had T1b stage tumors, and eight had LN metastases. In contrast, the current systematic review did not identify local tumor recurrences or distant metastasis in the small number of patients who underwent delayed surgery after ablation. This discrepancy may be due to differences in patient inclusion criteria, the extent of the ablation zone, and qualities of the treatment center. Acceptable inclusion criteria may be adopted from those used for AS. It can, for example, be based on the clinical framework for risk stratification in determining whether AS is appropriate for PTMC categorized patients as ideal, appropriate, or inappropriate for AS based on imaging findings, and the characteristics of the patient and/or medical team (36). Based on strict stratification, the patients classified as inappropriate for AS should not be considered for thermal ablation. However, patients with a fear of undergoing surgery can be considered for thermal ablation. Because the ablation procedure is totally operator dependent, the qualities of the operator and the treatment center are essential. The finding that most of the complications were minor, with transient hoarseness being the most frequent complication, indicates that the operator should be thoroughly trained in US-based anatomy, especially in the evaluation of the danger triangle, that is, the tracheoesophageal groove including the RLN, trachea, and esophagus (37). In addition, the operator needs to be fully competent with the technical aspects of thermal ablation, including the use of a small active tip, the moving shot technique, and hydrodissection, thereby maximizing the efficacy and minimizing complications associated with thermal ablation (38).
This study has several limitations. First, some of the included studies were case–control studies, which varied in cohort size and mean FU duration. Additional well-designed multicenter studies comparing ablation with surgery or observation, with long-term FU, in large-sized populations are needed to clarify the efficacy of thermal ablation for low-risk PTMCs. Second, the criteria for ablation in the included studies were not identical, despite all of these studies assessing patients with low-risk PTMCs. The definitions of disappearance also differed among studies, as four of the included studies did not define scar-like changes as disappearances (8,11 –13).
In conclusion, this systematic review shows that thermal ablation methods are safe and effective for local tumor control in patients with low-risk PTMCs, minimizing the delayed surgery rate. Strict inclusion criteria and technical proficiency are required to maximize favorable results.
Footnotes
Author Disclosure Statement
All authors declare no competing financial activities relating to this article. Financial activities not related to this article are J.H.B. is a patent holder for a unidirectional ablation electrode. J.H.B. has been a consultant to two radiofrequency companies, STARmed and RF Medical, since 2017.
Funding Information
No funding was received for this article.