
Abstract
Background:
Thyroid disease is prevalent in women of reproductive age, while infertility is common in women with thyroid dysfunction. In this study, we review the recent advances in the field of thyroid and fertility since the publication of the 2017 American Thyroid Association pregnancy guidelines.
Summary:
Recent studies have confirmed associations of thyrotropin (TSH) elevation and/or thyroid autoimmunity with infertility and low ovarian reserve in subsets of women, and have led to a better understanding of the pathogenesis linking thyroid autoimmunity with infertility. Even though the benefit of treating patients with TSH >4 mIU/L has been confirmed in a large retrospective cohort study, two large randomized controlled trials have failed to show benefit of thyroid hormone on obstetrical outcomes in euthyroid women with thyroid autoimmunity. New data have emerged regarding the potential gonadal toxicity of radioactive iodine (RAI), based on its impact on ovarian reserve and sperm chromosomal abnormalities.
Conclusions:
There is continued evidence supporting an important role of thyroid hormone in regulation of reproductive tissues at many levels. Recent randomized trials have failed to identify a benefit of thyroid hormone in euthyroid women with thyroid autoimmunity. Further research in the field is needed to more completely delineate the relevant pathways and identify women who may benefit from levothyroxine treatment. The impact of RAI on fertility also merits further investigation.
Introduction
Thyroid disease is quite prevalent in women of reproductive age. About 11% of women have thyroid autoimmunity, 2–3% have hypothyroidism, and 1–2% have hyperthyroidism (1). Thyroid cancer incidence has been rising in recent years, and thyroid cancer is the most common cancer in women between the ages of 20 and 39 years (2). Infertility is also quite common in women with Graves' and Hashimoto's disease, affecting ∼50% of patients (3).
The 2017 American Thyroid Association (ATA) pregnancy guidelines, based upon the data to date and a number of recent studies confirming adverse effects of subclinical hypothyroidism and thyroid peroxidase antibody (TPO Ab) positivity on obstetrical outcomes (4,5), as well as demonstrated benefit of levothyroxine in lowering adverse outcomes (6,7), recommend testing high-risk women with thyrotropin (TSH) in early pregnancy, followed by reflex measurements of anti-TPO Abs in women with TSH levels between 2.5 and 10 mIU/L (8). For antibody-positive women, the guidelines recommend treatment if the TSH is between the upper limit of the pregnancy-specific reference range and 10 mIU/L, and consideration of treatment for TSH levels between 2.5 mIU/L and the upper limit of the pregnancy-specific reference range. For anti-TPO Ab-negative women, the guidelines recommend to consider treatment for women with TSH levels between the upper limit of the pregnancy-specific reference range and 10 mIU/L, and no treatment if the TSH is between 2.5 mIU/L and the upper limit of the pregnancy-specific reference range (8). In women seeking pregnancy through assisted reproductive technologies, the guidelines recommend levothyroxine treatment of subclinical hypothyroidism, defined as a TSH >2.5 mIU/L in many studies, with a goal for the TSH of <2.5 mIU/L. For women who are euthyroid but have thyroid autoimmunity, in whom there is lack of evidence of clear benefit, the guidelines recommend to consider treatment, given the low-risk/potential benefit ratio (8). With respect to thyroid cancer, the guidelines recommend that women wait 6 months and men wait 120 days to conceive after radioactive iodine (RAI) treatment, because of the potential for suboptimal control of thyroid hormone levels after RAI administration, as well as the known effects of RAI to date on spermatogenesis (8).
For the purposes of this discussion, fertility is defined as the ability to produce live offspring; conception and miscarriage rates are key determinants. In this study, we review recent advances in the field of thyroid and fertility accumulated since the publication of the 2017 ATA pregnancy guidelines, and discuss new insights gleaned from these studies. Specifically, there have been important advances in the areas of hypothyroidism, thyroid autoimmunity, the relationship between thyroid function and reproductive physiology, and thyroid cancer treatment, in particular RAI treatment, with respect to fertility. We also summarize areas that merit further investigation.
Review
Hypothyroidism
Observational studies
Two studies have recently evaluated the effect of mild TSH elevation on pregnancy outcomes. The study by Tuncay et al., a retrospective cohort study of 302 women undergoing intrauterine insemination (IUI) for the first time, regardless of the cause for IUI, showed that the outcomes of miscarriage, clinical pregnancy, and live birth rates were not different in patients with TSH levels of 2.5–5 mIU/L compared with TSH 0.4–2.5 mIU/L (9). Antithyroid antibodies were not determined.
In a cross-sectional study of 239 women with infertility, women with unexplained infertility had slightly higher TSH levels compared with those whose partners had severe male factor infertility (1.95 vs. 1.66 mIU/L). Also, the percentage of women with TSH >2.5 was twice as high in the unexplained infertility group as the male infertility group (26.9% vs. 13.5%) (10). Nevertheless, whether such a small difference in TSH within the reference range significantly impacts outcomes is in question. In a cross-sectional analysis of a prospective Belgian cohort of 1321 euthyroid pregnant women without thyroid autoimmunity, a TSH ≥2.5 mIU/L (mean TSH 2.98 mIU/L) was not associated with adverse pregnancy outcomes compared with TSH levels <2.5 mIU/L (mean TSH 1.31 mIU/L) (11).
With respect to treatment, Maraka et al. (12) studied obstetrical outcomes in a large retrospective cohort of 5405 women in the United States with subclinical hypothyroidism, of whom 16% were treated with levothyroxine. The benefit of levothyroxine treatment in terms of lowering miscarriage risk was depending on pretreatment TSH. Subjects with a pretreatment TSH of 4.1–10 mIU/L had a reduction of 55% in miscarriage risk, whereas patients with a pretreatment TSH in the 2.5–4.0 mIU/L range did not benefit from a reduction in miscarriage rates (12). Of note, thyroid autoimmunity was not evaluated. This study confirmed prior findings of a large retrospective study in the United Kingdom showing reduction of miscarriage with levothyroxine in patients with TSH >4 mU/L, but not in those with a TSH of 2.5–4 mU/L (7). Levothyroxine treatment, however, was associated with higher rates of pre-eclampsia compared with controls (11).
In summary, recent small observational studies addressing the impact of TSH elevations in pregnancy have failed to conclusively show a relationship of TSH in the 2.5–5 mIU/L range with impaired fertility. A large retrospective cohort study, however, did show that levothyroxine treatment decreased miscarriage rates in patients with TSH levels between 4.1 and 10 mIU/L, but not in those with a TSH 2.5–4 mIU/L, confirming prior findings.
Thyroid autoimmunity
Observational studies
There have been a number of studies in the last couple of years evaluating the impact of thyroid autoimmunity on fertility and on ovarian reserve. Analysis of a retrospective cohort of 3143 women in Belgium undergoing their first IUI, regardless of reason, showed no association of anti-TPO Ab positivity with delivery, pregnancy, or miscarriage rates (13). However, in a prospective study of 1468 women, which was a secondary analysis of two multicenter randomized controlled trials (RCTs) in the United States including euthyroid infertile women mainly with unexplained infertility or polycystic ovarian syndrome, anti-TPO Ab positivity was associated with a doubling of miscarriage risk and an odds ratio for live birth of 0.58 [95% confidence interval (CI) 0.35–0.96] (14). TSH levels >2.5 mIU/L did not affect the rates of conception, clinical pregnancy, first trimester pregnancy loss, or live birth, compared with TSH levels <2.5 mIU/L.
Two studies have evaluated the association of thyroid autoimmunity with ovarian reserve, and the findings support the concept that thyroid autoimmunity is associated with low ovarian reserve in subsets of infertile women. The first is a cross-sectional study of 1044 women undergoing IUI/in vitro fertilization (IVF) in China. After they grouped women according to anti-Müllerian hormone (AMH) levels to low (<15% for age-adjusted range), normal (15–85%), and high (>85%) ovarian reserve categories, the investigators showed that in the whole group there was no association between thyroid function tests or thyroid antibody status and ovarian reserve (15). However, after excluding 111 women with known causes of low ovarian reserve (iatrogenic causes and karyotypic abnormalities), women with low ovarian reserve were found to have a significantly higher percentage of anti-TPO Ab positivity (22.7%) compared with those with normal (14%) or high ovarian reserve (10.3%) (p = 0.012) (15). Women with unexplained infertility, comprising 1/3 of the group, had the most statistically significant association, with 28.6% being anti-TPO Ab positive in the low ovarian reserve group, 15.7% in the normal ovarian reserve group, and 9.5% in the low ovarian reserve group (p = 0.02) (15). These findings are in contrast with a prior large cross-sectional study of a retrospective cohort of 4894 women in Belgium who did not show an association of hypothyroidism or thyroid autoimmunity with low ovarian reserve as defined by AMH levels (16).
A smaller prospective cohort study from the United States including 436 patients attending the Massachusetts General Hospital infertility clinic, using antral follicle count (AFC) as a surrogate marker of ovarian reserve, showed that in the whole study population there was no association with anti-TPO Ab positivity (17). However, in a subgroup analysis of women with diminished ovarian reserve and unexplained infertility, anti-TPO Ab positivity was associated with a decrease in AFC. The authors also showed that anti-TPO Ab positivity, as well as low free triiodothyronine (fT3) levels, were associated with a blunting of the inverse association between AFC and follicle-stimulating hormone (FSH), compared with the anti-TPO Ab-negative and high fT3 groups, respectively (17). Finally, analysis of an Italian retrospective cohort of 123 euthyroid women and their 513 embryos demonstrated that thyroid autoimmunity was associated with a decreased percentage of grade 1 (good quality) embryos during IVF and a higher percentage of grade 2 (fair quality) and grade 3 (poor quality) embryos, compared with subjects without thyroid autoimmunity (18).
Randomized controlled trials
The most exciting recent developments in the field of thyroid autoimmunity and fertility have been the results of two large RCTs. The Pregnancy Outcomes Study in Euthyroid Women With Thyroid Autoimmunity After Levothyroxine (POSTAL) evaluated the impact of levothyroxine treatment in euthyroid anti-TPO Ab-positive women on obstetrical outcomes in women undergoing IVF (19). The study randomized 600 women, after excluding women at high risk of miscarriage, such as women with a prior history of two or more miscarriages and women positive for antinuclear Abs, anticardiolipin Abs, or lupus anticoagulant. The primary outcome of miscarriage rates was similar in the intervention versus the control group (10.3% vs. 10.6%). Similarly, clinical pregnancy rates and live birth rates were not affected by levothyroxine treatment (19).
This study has a number of limitations that should be considered when interpreting the results. It was an open-label trial, single-center RCT, the ovarian hyperstimulation protocols were not uniform among patients, and the numbers were too small in important subgroup analyses. TSH levels and anti-TPO Ab titers were slightly higher in the intervention group compared with the control group, which would bias potentially the results toward the null hypothesis. No data were given regarding the percentage of patients achieving a TSH at goal; compliance was only assessed through phone calls. Rates of miscarriage were quite low, far lower than the 30% expected, when the authors made their power calculations. Therefore, it is unclear if the study had enough power to detect expected differences. Most importantly, the authors excluded the populations most likely to benefit, and therefore their findings are only potentially applicable to women at low risk of miscarriage. Nevertheless, this study was included in a recent meta-analysis, along with three prior much smaller RCTs studying the impact of levothyroxine on obstetrical outcomes in euthyroid patients with subclinical hypothyroidism or thyroid autoimmunity undergoing IVF (20). With the inclusion of this study, the meta-analysis concluded that levothyroxine treatment has no statistically significant impact on live births in women with subclinical hypothyroidism or thyroid autoimmunity undergoing IVF; however, it does decrease miscarriage rates by ∼50% (20).
The second RCT is the much anticipated Thyroid Antibodies and Levothyroxine (TABLET) trial, a multicenter study of 940 women in the United Kingdom, which evaluated the effect of levothyroxine on live births in euthyroid anti-TPO Ab-positive women with a history of infertility or miscarriage (21). Levothyroxine was started preconception and was continued throughout pregnancy. Treatment did not result in a significant change in live birth rates (relative risk [RR] = 0.97 [CI 0.83–1.14]) or any of the secondary outcomes, including miscarriage (21). This study was large, multicenter, and well designed, with initiation of thyroid hormone treatment preconception. A few limitations are noted. The thyroid hormone dose was fixed at 50 mcg daily and was not further adjusted upon confirmation of pregnancy, per guideline recommendations. In the control group, the TSH levels decreased over time during pregnancy, which is not the expected course of TSH in anti-TPO Ab-positive patients. Due to these factors, the TSH between the two groups was quite similar by 16 weeks (1.3 vs. 1.6 mIU/L). There was not antibody-negative control group. The patient population was a mix of infertile patients and those with history of miscarriage. Anti-TPO Ab testing was not performed at a central laboratory, but instead performed at local facilities, using 22 different assays, each with its own methodology and reference range for positivity. Finally, it is important to note that the trial agent was discontinued in patients who developed abnormal thyroid tests during the study (∼10% in each arm). Therefore, the negative results apply only to subjects who maintained normal function before and throughout pregnancy; no conclusions can be drawn for subjects who developed thyroid insufficiency.
Nevertheless, the results of the TABLET study are provoking. A prior small (N = 72) RCT of anti-TPO Ab-positive women undergoing assisted reproduction technologies had shown a decrease in miscarriage rates in levothyroxine-treated women, from 52% to 33%, which, however, did not meet statistical significance, likely due to the study being underpowered (22). Another RCT by Negro et al. has shown a significant decrease in miscarriage rates with levothyroxine treatment of euthyroid anti-TPO-positive patients, from 13.8% to 3.5% (6). The discrepancy between the TABLET study results and this RCT could be potentially explained by the following: (i) a lower dose of thyroid hormone used in the TABLET trial compared with the study by Negro et al. (6), who adjusted levothyroxine according to TSH levels, achieving TSH levels similar to the anti-TPO-negative controls during pregnancy; (ii) a nonuniform antibody cutoff and the use of many different assays in the TABLET trial, which may have resulted in including a population of women who are not truly antibody positive, as different assays have different diagnostic validities; and (iii) disparate patient populations [infertile or with a history of miscarriage in TABLET versus all-comers in the study by Negro et al. (6)].
In summary, the studies in the last few years have confirmed an association of thyroid autoimmunity with infertility and low ovarian in subsets of women, while two large RCTs of euthyroid women with anti-TPO positivity failed to show an effect of levothyroxine treatment in improving rates of miscarriage and live births.
Thyroid and reproductive physiology
Ovarian follicular development goes through multiple stages: primordial follicle, primary follicle, secondary follicle, preantral follicle, and antral follicle. The oocyte is surrounded by layers of granulosa cells that provide critical support for proper oocyte development. We have known for more than a decade, through both messenger RNA analysis and protein studies, that many different cells in the ovary, including cells of the epithelium, oocytes, and granulosa cells, express the TSH receptor, thyroid hormone receptor (TR)alpha1, TRalpha2, and TRbeta1, with expression of these proteins being differentially regulated at different stages of follicular development (23). Similarly, the endometrium expresses these proteins differentially throughout the various phases of the menstrual cycle (24). Thyroid hormone plays a critical role in implantation and early fetal development through actions on the placenta and endometrium (25), including regulation of the invasiveness of extravillous trophoblasts (26). A 2015 review by Vissenberg et al. clearly summarized the state of knowledge regarding the expression of thyroid-related proteins in reproductive tissues (27), and reviewed data showing expression of thyroid receptors, deiodinases, and thyroid hormone transporters in oocytes, endometrium, placenta, and fetal tissues. In addition, multiple effects of thyroid hormone were reviewed such as its synergistic action with FSH to promote granulosa cell proliferation, enhancement of the invasive potential of the extravillous trophoblast through effects on matrix metalloproteinase expression, and enhancement of endometrial receptivity during the window of implantation (27).
A recent animal model of chronic hypothyroidism studied its effects on the growing follicle population. After rats were made hypothyroid through a 16-week low iodine diet, there was a significant decrease in the number of growing follicles (28). An in vitro study using rat ovarian cells showed that high doses of triiodothyronine (T3) induced an increase in follicle volume of 40% after 7 days in culture, while T3 decreased rates of apoptosis of granulosa cells, when they were cultured in medium deprived of serum, similar to the effects seen with FSH (29).
While thyroid hormones have been shown to affect reproductive tissues, the thyroid is also regulated by reproductive hormones. The most notable example is human chorionic gonadotropin (hCG), which through its high homology with TSH cross-reacts with the TSH receptor, resulting in a linear association of hCG with free thyroxine (fT4) and, subsequently, in an inverse association of hCG with TSH levels during pregnancy (30). Korevaar et al. (31) recently showed that this relationship is altered in the presence of thyroid autoimmunity. Using samples from two large prospective Dutch cohorts, the authors described that the normal linear relationship of fT4 with hCG, seen in anti-TPO Ab-negative women, was significantly blunted in anti-TPO Ab-positive women (31). Similarly, the negative association of TSH with hCG was significantly attenuated in anti-TPO Ab-positive women. The authors went on to show that the subset of anti-TPO Ab-positive women who did not have an appropriate response to hCG had a 2.2- to 2.8-fold higher risk of preterm delivery, providing a possible explanation regarding the pathogenic link between thyroid autoimmunity and preterm delivery (31). Thyroglobulin antibodies also identify patients with thyroid autoimmunity and, in fact, isolated thyroglobulin antibodies are present in 5% of women (32). A recent study by Hou et al. (33) showed that thyroglobulin antibodies also interfere with the thyroidal response to hCG, and confirmed the findings by Korevaar et al. (31) established for anti-TPO-positive women.
Finally, a recent immunocytochemistry study by Monteleone et al. showed expression of TPO on cumulus granulosa cells isolated from retrieval of ovarian follicles in three women undergoing IVF (34). This is the first study showing expression of the enzyme itself on ovarian tissue. If these findings are replicated and confirmed, they suggest the possibility that TPO Abs could target their antigen directly at the level of the ovary, and perhaps provide a mechanistic explanation for the infertility in some women with thyroid autoimmunity.
Thyroid cancer treatment
The effects of prior thyroid cancer treatment on fertility have not been thoroughly investigated in the past. A large recent retrospective population-based observational study involving >2 million mother-offspring pairs in the Korean national database evaluating the risk of adverse obstetrical outcomes in women with a history of thyroid cancer (0.32% of the population), in a country where about half of the patients with thyroid cancer receive RAI, showed that women with a history of thyroid cancer were older, with a higher prevalence of prepregnancy diabetes mellitus and hypertension (35). After adjusting for these variables, no increase in stillbirths was found in women with a history of thyroid cancer. More detailed outcomes of interest with respect to fertility were not investigated, while women with a history of thyroid cancer were found to have overall similar pregnancy outcomes compared with control women, but be at higher risk of multiple gestations and postpartum hemorrhage (35).
Radioactive iodine
A prior meta-analysis has described that RAI treatment causes transient amenorrhea in up to 27% of women and slightly earlier menopause (36). Prior studies concluded that fertility and rates of pregnancy loss are not affected (36,37). In men, RAI had been associated with a transient increase in FSH and reduction in normokinetic sperm (38), but fertility in the long run has not been thought to be impacted unless cumulative doses of RAI exceed 400 mCi (39). Recent prospective studies, however, have provided some concerning data regarding adverse effects of RAI on the gonads.
Two prospective studies evaluated the impact of RAI on ovarian reserve by measuring serial levels of AMH, starting at baseline, and then at regular intervals, up to 1 year after RAI treatment. The first study, from Israel, evaluated 24 women, at a mean age of 34 years, after receiving a mean dose of 103 mCi after Thyrogen stimulation. The authors showed that AMH levels reached a nadir at 3 months after RAI, falling from 3.2 to 1.9 ng/mL, and then partially recovered, with levels at 12 months ∼30% lower than at baseline (40). Normally, AMH drops by 0.2 ng/mL per year as women age, so the observed decrease is quite significant. In subgroup analysis, the authors showed that women >35 years of age had a higher drop in AMH compared with women <35 years of age. Five women in their study had underlying Hashimoto's thyroiditis; these women were the most vulnerable, with a drop of AMH at 3 months of >70% (40). In contrast, five patients who were treated for Graves' disease with a mean activity of 13 mCi did not have a decrease in AMH (40). The second study, from Turkey, evaluated 33 women, at a mean age of 31 years, after receiving RAI after thyroid hormone withdrawal at a mean activity of 111 mCi (41). This study showed similar findings, with significant drop of AMH at 3 months, with only slight recovery by 12 months. Women over the age of 30 years had higher decreases in AMH than younger women (41).
Does this decrease in AMH translate into lower birth rates? Data from a North Carolina registry of 2360 women with thyroid cancer between the ages of 15 and 39 years were recently analyzed to assess the impact of RAI treatment on birth rates. Cumulative incidence of birth rates over a 14-year follow-up period was similar in the group that had received RAI and the group that had not. The authors did find that, at the extremes of the age spectrum of their population, birth rates were lower in the group exposed to RAI, but the data did not reach statistical significance (42). A prior, much larger California registry study of 18,850 women also failed to show an impact of RAI on birth rates in the whole population. However, in subgroup analysis, women in the 35–39 years age group were negatively affected and had 16.3 live births per 1000 women in the unexposed group versus 11.5 live births per 1000 women in the group exposed to RAI (p < 0.01) (43). Median time to live birth was 8.4 months longer in the group that received RAI (43).
Finally, one study has recently prospectively studied the impact of RAI in men. Twenty-four men, at a mean age of 36 years, were followed with serial measurements of FSH, inhibin B, and sperm analyses, after receiving an average of 100 mCi of RAI for thyroid cancer, in the setting of thyroid hormone withdrawal (44). FSH rose at 3 months and then partially recovered by 13 months after treatment, inhibin B fell at 3 months and then partially recovered by 13 months after treatment, while sperm count fell at 3 months but fully recovered by 13 months. The novel finding consists in the demonstration of frequent chromosomal sperm abnormalities, mainly aneuploidies. The rate of these increased from 3.2% to 4.8% at 3 months after RAI. By 13 months, the rate improved slightly to 3.7%, but this remained higher than the baseline rate (p = 0.01) (44).
These three new prospective studies shed new light into potential reproductive risks of RAI through effects on ovarian reserve and chromosomal abnormalities in sperm that warrant further investigation in larger cohorts.
Discussion
The developments in the area of thyroid and fertility since 2017 have important implications for the field. The ramifications of the two recent RCTs showing no impact of levothyroxine on obstetrical outcomes in euthyroid patients with thyroid autoimmunity, as well as the new data regarding the expression of TPO in the ovary and the impact of anti-TPO Abs on the thyroid's response to hCG, are significant. There are three hypotheses that have been proposed in the past regarding the association of thyroid autoimmunity with infertility in the setting of euthyroidism. The first is that thyroid autoimmunity is an epiphenomenon; that is, it is a marker of generalized autoimmunity and not a pathogenic factor by itself. An altered immune status with enhanced natural cytotoxicity has been recently described in women with thyroid autoimmunity (45). The second hypothesis is that thyroid antibodies are directly pathogenic to ovarian tissue. The third hypothesis is that thyroid autoimmunity causes a degree of relative hypothyroidism that adversely impacts reproductive tissues. Data from the recent studies lend support to some of the above possibilities.
The results of the past RCT by Negro et al. were supportive of the third hypothesis, given the significant impact that thyroid hormone had in that study in reducing both miscarriage and preterm delivery rates in euthyroid women with autoimmunity (6). The study by Korevaar et al. described above also shows that thyroid autoimmunity results in a blunting of the thyroid response to levothyroxine, which is associated with preterm delivery (31). This pathogenetic mechanism would provide a rationale for the effectiveness of thyroid hormone supplementation in ameliorating adverse obstetrical outcomes. On the contrary, the results of the POSTAL and TABLET RCTs, which showed no impact of thyroid hormone on adverse obstetrical outcomes in women with thyroid autoimmunity, are more consistent with the underlying pathophysiology mechanism being unrelated to levels of thyroid hormone, but rather related to a direct autoimmune phenomenon. The recent finding of TPO expression by mature granulosa cells, if confirmed, would provide support for a potential direct pathogenic effect of thyroid autoimmunity on the ovary. How does one reconcile all of the above findings?
One potential model of the pathogenesis involved in the link between thyroid autoimmunity and fertility is presented in Figure 1. Teleologically, we have evolved to maximize thyroid hormone exposure to reproductive tissues during pregnancy. HCG, through its high homology with TSH, may act to stimulate the thyroid to ensure adequate thyroid hormone supply during pregnancy. The ovary, the endometrium, the placenta, and the fetus all express thyroid hormone transporters, thyroid deiodinases, and thyroid hormone receptors that mediate actions of thyroid hormone at all levels of reproduction and development. It is possible that in the setting of thyroid autoimmunity, we have two mechanisms at play, depending on the severity of the autoimmune process. At early stages of autoimmunity, or potentially when anti-TPO Ab levels are low, it is possible that the main impact is through a hostile immune environment at the level of the ovary, with TPO as the direct antigen. If one intervenes at that stage with thyroid hormone (Fig. 1A), one would expect that there would be no impact on outcomes, as in early stages of thyroid autoimmunity, the thyroid hormone response would be intact. At that stage, strategies aimed to lower anti-TPO Ab titers, such as potentially treatment with selenium, steroids, or other immunomodulatory agents, might be effective instead. As thyroid autoimmunity progresses however, it could also result in an impaired thyroidal response to hCG stimulation, providing inadequate thyroid hormone support under conditions of extra demand such as pregnancy, and eventually result in subclinical hypothyroidism. In that situation (Fig. 1B), one would expect that treatment with thyroid hormone would be beneficial. If this model is correct, one would need to identify whether there are subsets of women with thyroid autoimmunity that are still in the euthyroid phase, which would benefit from levothyroxine treatment, such as potentially those with an impaired response to hCG stimulation.
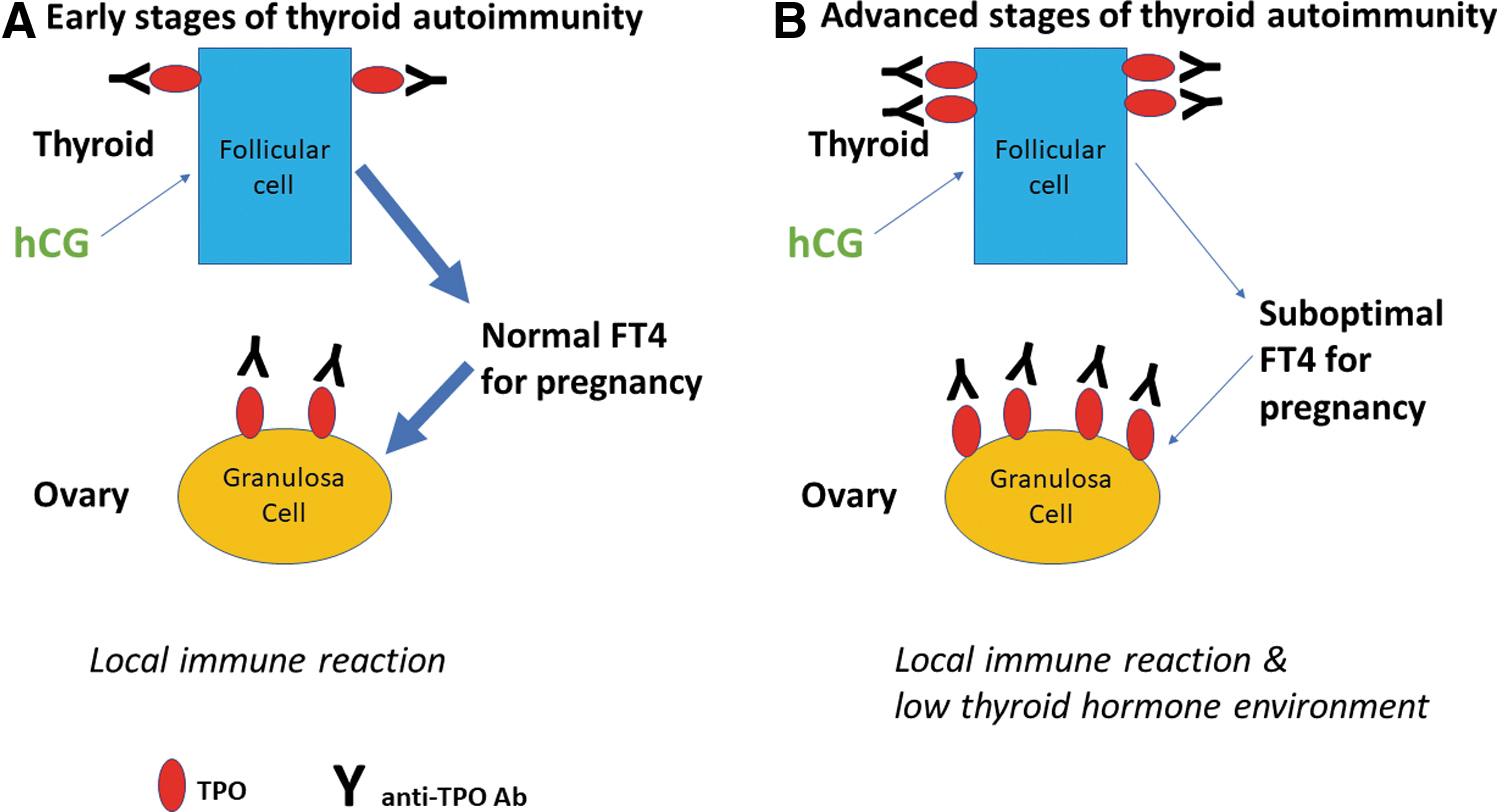
Proposed model of the link between thyroid autoimmunity and infertility.
It is possible that different mechanisms are at play in pregnancies conceived naturally versus those conceived through IVF. A recent meta-analysis of four case–control and cohort studies by Poppe et al. showed that thyroid autoimmunity did not impact miscarriage rates in patients undergoing intracytoplasmic sperm injection (46). Consistent with these data, another recent meta-analysis of 13 studies has shown that the benefit of levothyroxine in reducing miscarriages in euthyroid women with thyroid autoimmunity may only be present in women conceiving naturally, and not in those using assisted reproduction technologies (47). Specifically, in women with thyroid autoimmunity, levothyroxine supplementation reduced risk of pregnancy loss (RR = 0.61 [CI 0.39–0.96]) and preterm birth (RR = 0.49 [CI 0.30–0.79]) in naturally conceived pregnancies but not in pregnancies achieved by assisted reproduction (47).
Look to the future
There is still one large ongoing trial in the field of thyroid and fertility that we are eagerly awaiting results from. The T4-LIFE trial in the Netherlands is a large RCT investigating the effect of levothyroxine on live births in euthyroid anti-TPO Ab-positive women with a history of recurrent pregnancy loss. The results will provide an important contribution, as the study has targeted a population at high risk of miscarriage.
Multiple other areas are in need of further investigation. We still need to identify the subsets of euthyroid infertile women who may benefit from levothyroxine treatment. It is possible that only particular subgroups, such as women with unexplained infertility, or a history of multiple miscarriages, or women who do not mount a proper thyroidal response to hCG, may benefit from levothyroxine. The T4-LIFE study above will be addressing the multiple miscarriage group. It is also possible that there are different benefits of levothyroxine treatment in women conceiving naturally versus those conceiving through assisted reproduction. Further studies should try to confirm whether TPO is indeed a local antigen at the level of the ovarian follicle and, if it is, aim to develop strategies to lower anti-TPO Ab levels and study the impact of that intervention.
In the area of thyroid and reproductive physiology, we need to further investigate the role of thyroid hormone in oocyte maturation, implantation, and placentation. In the area of thyroid cancer, the association of prior thyroid cancer treatment with fertility outcomes needs to be further studied. We need to understand if the effects of RAI on ovarian reserve are fully reversible, dependent on administered activities of radioiodine, and a function of age. Subsets of women such as older women or women with underlying Hashimoto's appear to be more vulnerable to RAI effects. It is possible that high levels of TPO Abs render the ovary more susceptible to the toxicity of RAI. If these findings are confirmed, the mechanism needs to be investigated. Larger studies will provide a better understanding of the risks, which will allow us to more accurately counsel thyroid cancer patients seeking conception. We need to investigate whether there is a difference between recombinant TSH stimulation versus thyroid hormone withdrawal protocols in terms of impact on ovarian reserve. Finally, we need to more fully understand the impact of RAI on male fertility.
Summary
Recent studies since the 2017 guidelines have provided important insights into the complex interactions of thyroid diseases with fertility. They have shown that higher TSH and/or anti-TPO Abs are associated with infertility and decreased ovarian reserve in subsets of women, but not all women. They have confirmed that treatment of subclinical hypothyroidism with TSH >4 improves miscarriage rates, and that anti-TPO Abs are associated with increased risk of miscarriage in euthyroid infertile women. Two large RCTs of thyroid hormone in anti-TPO Ab-positive euthyroid patients have had negative outcomes, bringing into question the effectiveness of treatment in the studied populations. New insights have been provided regarding the pathways through which anti-TPO Abs affect fertility: both by affecting thyroidal stimulation from hCG and by being potentially directly pathogenic to granulosa cells. And finally, new prospective studies in both men and women are putting into question the reproductive safety of RAI treatment for thyroid cancer. This is an exciting time in the field of thyroid and fertility. There are still many unanswered questions that warrant further investigation. Future research needs to focus on identifying the subsets of infertile euthyroid women with thyroid autoimmunity that would benefit from thyroid hormone treatment, delineating more comprehensively the pathways of thyroid hormone action on reproductive tissues and investigating more thoroughly the impact of RAI on fertility.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.