
Abstract
Background:
The clinical course of Graves' disease (GD) in women who switched from methimazole (MMI) to potassium iodide (KI) during the first trimester of pregnancy has never been reported in detail.
Objective:
To investigate the characteristics of GD patients whose thyroid hormone levels increase after substituting KI for MMI.
Patients:
Two hundred forty women with GD who had been treated with MMI and switched from MMI to inorganic iodide to control hyperthyroidism during the first trimester between January 1, 2005, and March 31, 2018.
Results:
In 133 (55.4%) of the GD patients, medication was completely tapered during pregnancy, and the other 107 (44.6%) GD patients were taking medication at delivery: 57 were taking KI alone and 50 were taking an antithyroid drug with or without KI. It was difficult to control the maternal thyrotoxicosis of 22 of the 107 patients with KI alone, and a higher dose of MMI compared with the dose at the time of conception was required (worsened group). Multivariate analysis revealed that the TRAb value at the time of switch from MMI to KI was the only factor that predicted continuation of the thyroid suppression medication, but none of the parameters was a predictor of the worsened group.
Conclusions:
It must be kept in mind that a certain proportion of GD patients escape from the antithyroid effect of iodide and that careful follow-up is necessary after switching a pregnant patient's medication to KI.
Introduction
Graves' disease (GD) is common in young women of childbearing age. GD patients who desire a future pregnancy should be treated with medical therapy, radioactive iodine therapy, or surgery, and pregnancy should be postponed until a stable euthyroid state is achieved. Maintaining a stable euthyroid state during pregnancy is important for both maternal health and fetal development. If medical therapy with an antithyroid drug (ATD) is required for the treatment of hyperthyroidism during the first trimester, propylthiouracil (PTU) is recommended as the first-line drug because of the possible associations of methimazole (MMI) with specific more serious congenital anomalies (choanal atresia, aplasia cutis, and esophageal atresia) than the face and neck anomalies and urinary system anomalies associated with PTU (1 –6).
We have been substituting potassium iodide (KI) for MMI to control hyperthyroidism during the first trimester in GD patients treated with MMI who cannot tolerate PTU because of adverse effects. We have reported finding that substituting KI for MMI in the first trimester of pregnancy decreased the incidence of major congenital anomalies (1.53%) in comparison with treatment with MMI alone (4.14%), and that there were no significant differences between the two groups in birth weight and gestational age at delivery (7).
Thyroid hormone levels were well controlled in most of the GD patients who were switched from MMI to KI, but in some patients it was difficult to control the maternal thyrotoxicosis after the switch to KI, and it became necessary to restart MMI and increase the dosage of MMI after the second trimester of pregnancy.
The aim of this study was to investigate the characteristics of GD patients whose thyroid hormone level increases after the switch from MMI to KI.
Subjects and Methods
We reviewed the cases of women with GD who had attended the outpatient clinic of Ito Hospital (Tokyo, Japan) and gave birth between January 1, 2005, and March 31, 2018. The 240 women with GD who were switched from MMI to inorganic iodide (≦38 mg) to control hyperthyroidism during the first trimester were retrospectively reviewed. Among the 240 women in this study population, there were 224 women who overlapped with the previous study population (7).The diagnosis of GD was based on clinical findings: the presence of a goiter and/or ophthalmopathy, elevated serum-free triiodothyronine (fT3) and free thyroxine (fT4) levels, a suppressed serum thyrotropin (TSH) level, and a positive TSH receptor antibody test. In some patients, radioactive iodine uptake was measured as a diagnostic test before pregnancy. The thyroid hormone status of each woman was evaluated during the first trimester of pregnancy by reviewing their fT3, fT4, and TSH levels measured before the switch from MMI to KI. Their thyroid hormone levels were measured again two to four weeks after the switch to iodine. KI was prescribed as an inorganic iodine dose of 10–30 mg per day in the form of a solution (10 mg of iodide per drop of the infusion) or in the form of KI tablets (38 mg of iodide per tablet). When the fT4 level after the substitution was within the reference range, the KI dose was tapered, and when the fT4 level was above the upper reference range, the KI dose was increased during the first trimester. When a patient being treated with KI was still hyperthyroid during the second trimester, an ATD was added to KI, or an ATD was substituted for KI.
Laboratory methods
TSH, fT3, and fT4 levels were measured by electrochemiluminescence immunoassays (ECLusys TSH, ECLusys fT3, and ECLusys fT4, respectively; Roche Diagnostics, Basel, Switzerland). The manufacturer's reference limits were TSH 0.2–4.5 mIU/L, fT3 2.2–4.3 pg/mL, and fT4 0.8–1.6 ng/dL. Based on the results of a previous study conducted on a large population, the reference intervals for maternal TSH and fT4 during the first trimester of pregnancy were 0.01–3.35 mIU/L and 0.77–1.91 ng/dL; their reference levels during the second trimester were 0.01–3.83 mIU/L and 0.86–2.44 ng/dL; and their reference levels during the third trimester were 0.01–3.67 mIU/L and 0.44–1.61 ng/dL. The reference ranges for umbilical cord serum TSH values and fT4 values were 0.09–18.0 mUI/L and 1.04–1.62 ng/dL, respectively (unpublished data). TRAb values were determined with an electrochemiluminescence immunoassay kit (ECLusys TRAb; Roche Diagnostics; reference value <2.0 IU/L).
Statistical analysis
Statistical analysis was performed with JMP software v14.0 (SAS Institute, Inc., Cary, NC). Differences between the discontinued group and the continued group and between the nonworsened group and worsened group were analyzed by the Wilcoxon test. p-Values <0.05 were considered significant. Multiple regression analyses were performed to identify possible predictors of the continued group and the worsened group. Receiver operating characteristic (ROC) curve analysis was performed to assess the optimal cutoff TRAb levels of GD mothers at the time of switch from MMI to KI for predicting the continued group.
Results
The median age of the 240 GD patients at the time of delivery was 33 years (range 20–44 years). The switch from MMI to KI was made at the first visit after conception. Most of the patients in the iodide group (228/240, 95%) were switched from MMI to KI within the first 10 weeks of gestation, and the median number of weeks of gestation at the time of switch to KI was 6 weeks (range 4–12 weeks). The initial dose of KI was 20 mg (range 5–38 mg). Patients with higher fT4 levels at the time of the switch tended to receive higher doses of KI (Fig. 1).
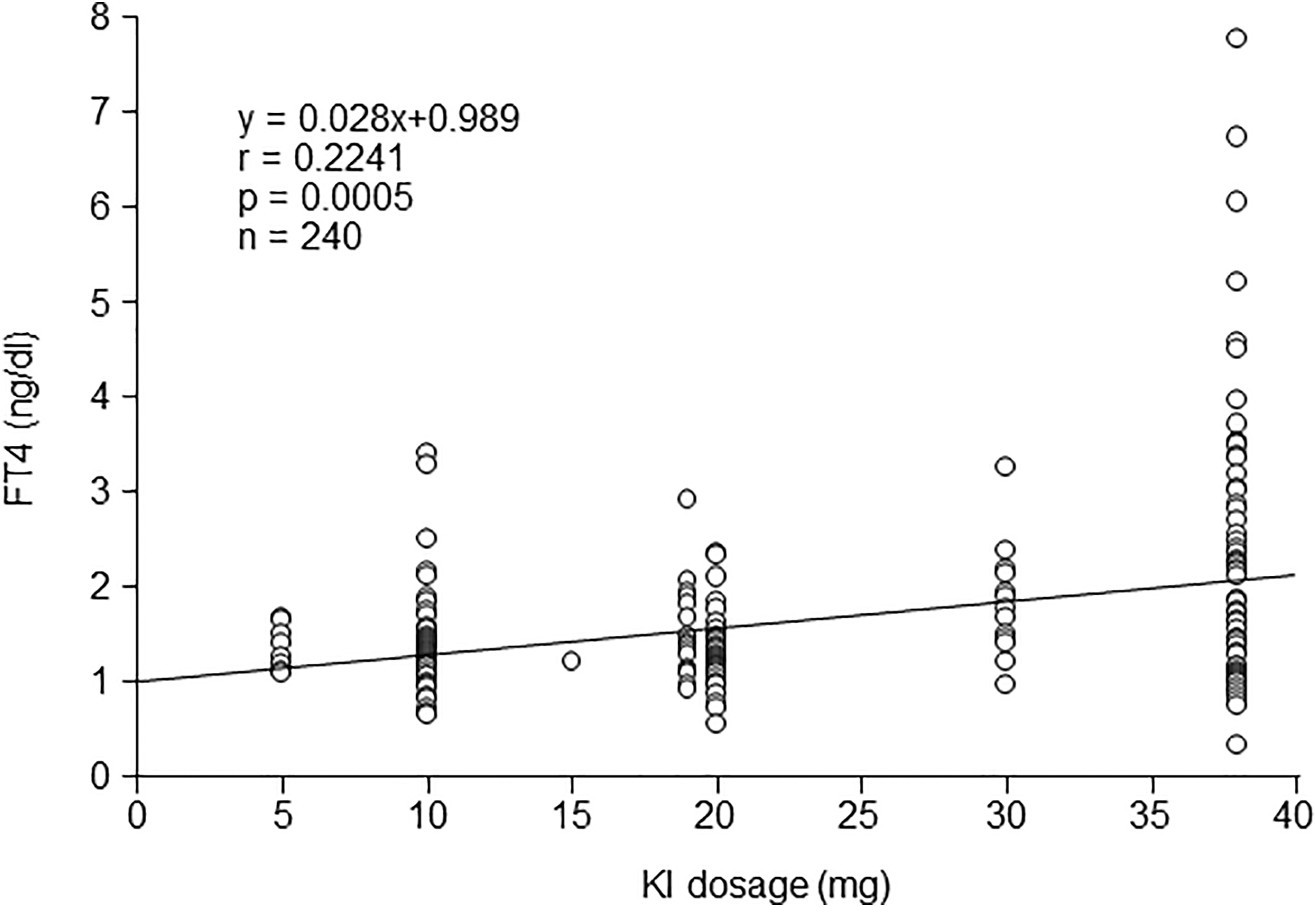
fT4 level at the time of switch from MMI to KI, and the initial KI dosage in each patient. MMI, methimazole; KI, potassium iodide.
In 133 GD patients (55.4%), medication was completely tapered during pregnancy: 129 of them were free of medication at delivery, and the other 4 patients were on thyroid replacement therapy with levothyroxine to maintain euthyroidism with a TSH level <2.5 μIU/L. The rest of the 107 GD patients (44.6%) were taking medication at delivery to control GD.
The characteristics of the group of GD patients in whom it was possible to discontinue KI or ATD at delivery (discontinued group) and group of patients who continued thyroid suppressive therapy (continued group) are given in Table 1, and a flowchart of the study population is shown in Figure 2. The MMI dose before the switch, KI dose at the time of switch, and TRAb titer at the time of switch were significantly higher in the continued group than in the discontinued group. The maternal TSH level at the time of switch during the first trimester and the mean gestational age of the newborns at delivery were significantly lower in the continued group than in the discontinued group. There were no significant differences between the two groups in maternal age, time of switch from MMI to KI during the first trimester, maternal fT4 level at the time of switch, and mean birth weight of the newborns.
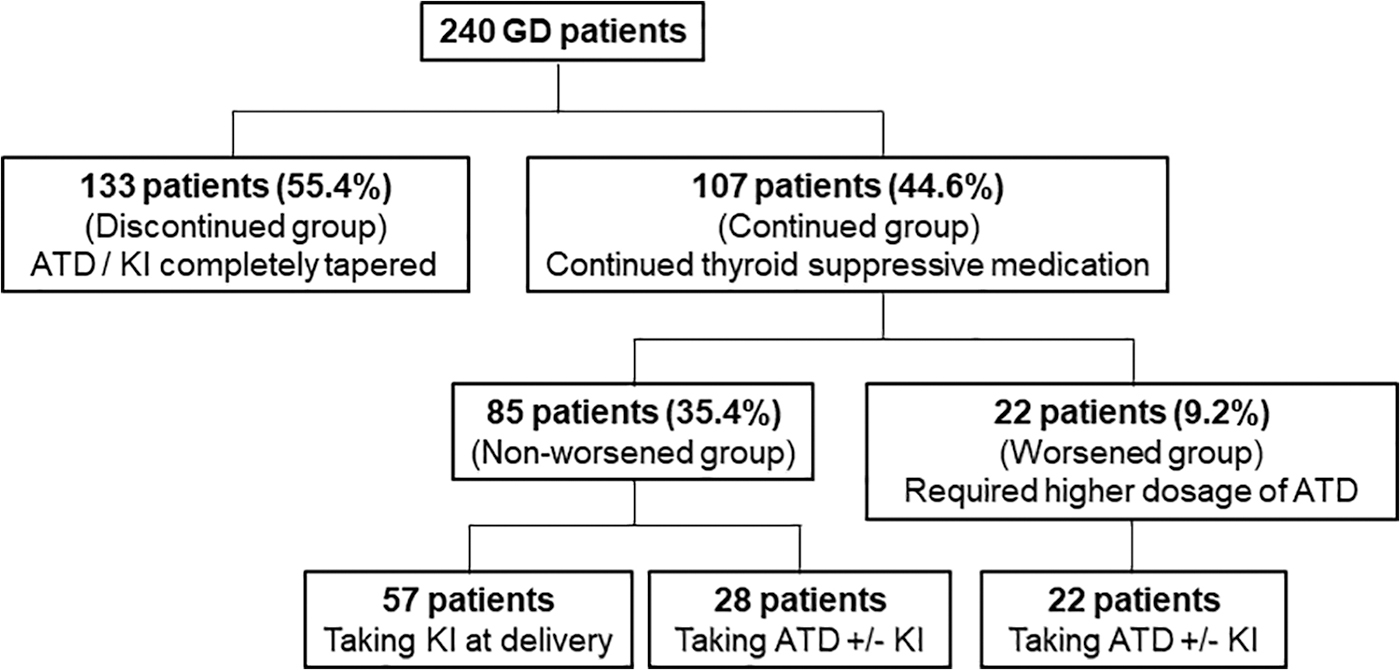
A flowchart of the study population. Medication was completely tapered during pregnancy in 133 of the 240 patients in the study population. The other 107 patients required medication until delivery, and 22 of them required a higher dose of MMI than their MMI dose at the time of conception (worsened group).
Comparison Between the Maternal and Neonatal Characteristics of the Discontinued Group and the Continued Group
10–90 percentile.
NS, not significant.
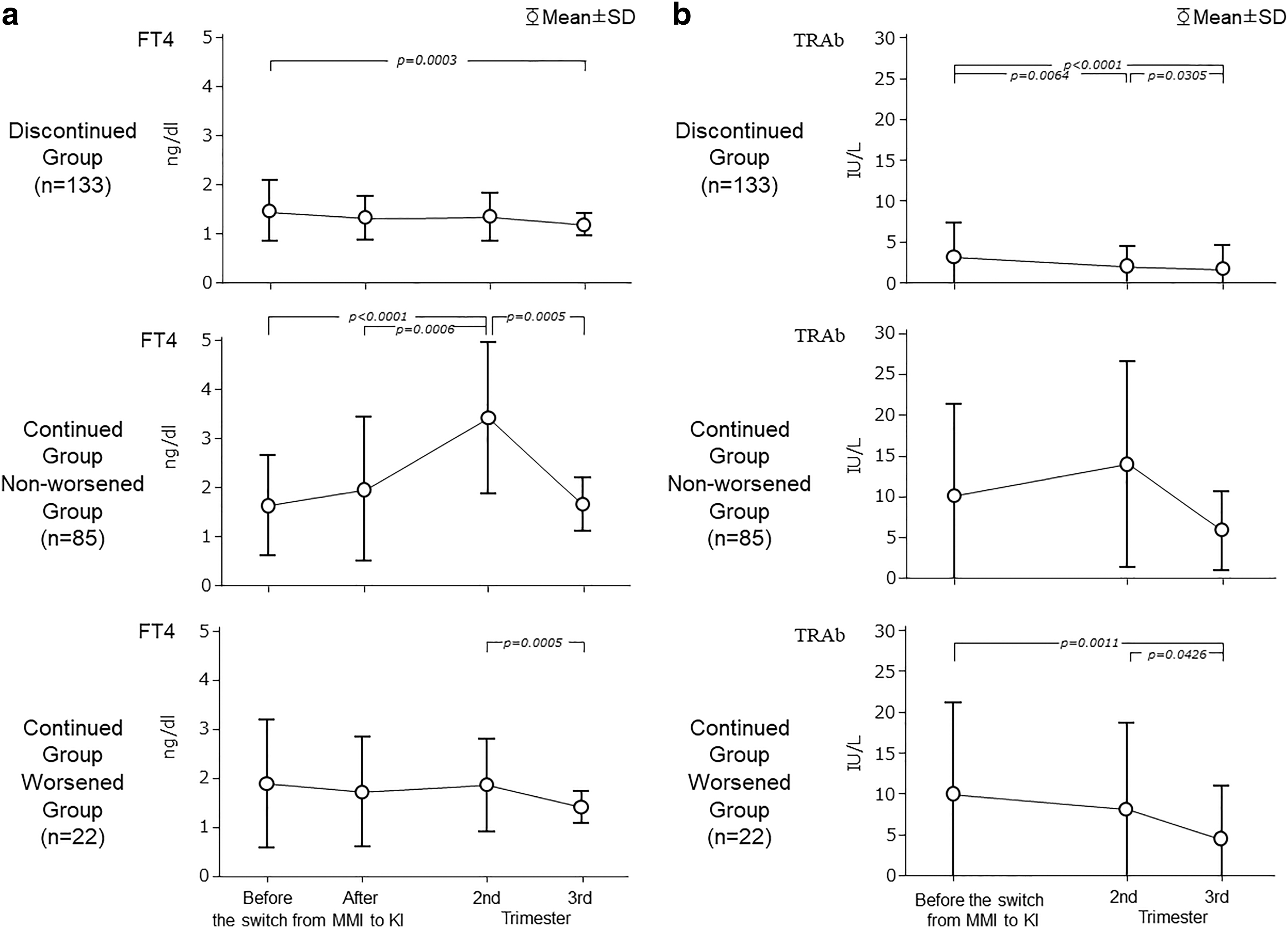
Figure 3a and b shows the fT4 levels and TRAb values before and after the switch from MMI to KI, highest fT4 levels and TRAb values during the second trimester of pregnancy, and during the third trimester of pregnancy in the discontinued group and the continued group.
(
Multivariate analysis revealed that the TRAb value at the time of switch from MMI to KI was the only predictor of continuation of the thyroid suppression medication. The ROC curve analysis showed that the cutoff TRAb value for predicting continuation of the medication was 6.8 IU/L. A maternal TRAb value >6.8 IU/L at the time of switch predicted continuation of medication with 44% sensitivity and 63.5% specificity. The area under the ROC curve was 0.742 (Fig. 4).

The receiver operating characteristic analysis showed that the cutoff TRAb value for predicting continuation of the medication was 6.8 IU/L. A maternal TRAb value >6.8 IU/L at the time of switch predicted continuation of the medication with 44% sensitivity and 63.5% specificity.
In 22 patients (9.2%), it was difficult to control the maternal thyrotoxicosis with KI alone after the switch during the first trimester, and a higher dosage of MMI than the initial dose at the time of conception was confirmed and was required in the third trimester (worsened group). A flowchart of the group of patients is shown in Figure 2, and the characteristics of the worsened group are given in Table 2. GD patients who required ATD or KI until delivery but did not require a higher dosage of MMI compared with the initial dose before the switch to KI were categorized as the “nonworsened group.” Of the 85 patients in the nonworsened group, 57 patients were taking KI alone, and 28 patients were taking an ATD with or without KI. All 22 patients in the worsened group were taking an ATD with or without KI. There were no significant differences between the nonworsened group and the worsened group in any of the variables investigated (Table 2). fT4 level and TRAb value before and after the switch from MMI to KI, highest fT4 level, and TRAb value during the second trimester of pregnancy and during the third trimester of pregnancy among the worsened group are shown in Figure 2. We performed a multivariate analysis including maternal age, time of switch from MMI to KI during the first trimester, MMI dose before the switch, KI dose at the time of switch, and maternal fT4 level, TSH level, and TRAb titer at the time of switch, but none of these parameters was a predictor of the worsened group. Thyroid size was measured in only 8 of the 22 patients, and median thyroid size was 40 mL (range 25–140 mL).
Comparison Between the Maternal and Neonatal Characteristics of the Worsened Group and the Nonworsened Group
Discussion
Recommendations for the management of GD with ATDs during pregnancy have been debated because of the risk of malformation of newborns associated with ATD use during the first trimester of pregnancy (1 –5). The latest guidelines of the American Thyroid Association for the management of GD patients choosing ATD treatment recommend that ATDs be avoided during the first trimester of pregnancy, but they state that when ATD treatment is necessary, PTU is preferable, because the malformations associated with PTU are less severe than those associated with MMI (2). Switching earlier might reduce the risk of birth defects, and it is recommended that women on ATDs attempting to conceive have a weekly pregnancy test and confirm a potential pregnancy as soon as possible (2). We previously reported finding that switching from MMI to KI during the first trimester of pregnancy did not completely prevent MMI embryopathy, but that the incidence of major anomalies was lower in the group of patients switched to KI (1.53%) during the first trimester than in the group treated with MMI throughout during the first trimester (4.14%) (7). Treatment of GD with KI is widely accepted by Japanese thyroid specialists, and its efficacy has been reported (8 –12). Treatment with KI during pregnancy has usually been considered contraindicated, because iodine is known to cross the placenta readily and possibly has an inhibitory effect on fetal thyroid hormone synthesis. Although several cases of neonatal hypothyroidism caused by excessive maternal iodine intake have been reported, none of the mothers had GD (13,14). According to several reports from Japan, iodine treatment of maternal hyperthyroidism due to GD did not cause neonatal hypothyroidism (7,8,15).
In our study, 55.4% of the GD patients who switched from MMI to KI went into remission during pregnancy, but 44.6% of the GD patients required an ATD or KI until delivery to control thyrotoxicosis. Multivariate analysis revealed that the TRAb values at the time of switch from MMI to KI were the only factor that predicted continuation of the thyroid suppression medication until delivery. A maternal TRAb value >6.8 IU/L at the time of switch was a predictor of continuation of the medication until delivery, but it was not an excellent predictor, because the area under the ROC curve was only 0.742.
It is well known that the antithyroid effect of iodide as monotherapy is incomplete and unsustained in some patients and their hyperthyroidism recurs, a phenomenon referred to as “escape” from control of thyrotoxicosis (12,16). The mechanism of the escape is still unclear. The inhibitory effects of excess iodide on thyroid hormone secretion is known as the Wolff–Chaikoff effect, and its inhibitory effect has been shown to be transient, and attributable to a decrease in iodide transport induced by decreased Na/I− symporter activity (17). There have been no reports on whether a similar phenomenon occurs in hyperthyroid subjects. None of the initial parameters predicted the response to KI. This finding is consistent with a previous study of GD patients that reported finding that none of the parameters assessed, including thyroid size and initial thyroid hormone levels, predicted the patients' response to KI therapy (10). Thyroid volume was not studied in every subject in our own study, but 22 of the patients had a relatively small goiter.
This study has the limitation of being a retrospective study, meaning that there was the potential for introducing biases because of having been conducted at a single institution. Further limitations include that the KI dose at the time of substitution differed from patient to patient, and that the KI treatment protocol varied in terms of continuation throughout pregnancy, addition of an ATD to KI, or switch to an ATD after the first trimester of pregnancy. Since iodine intake in Japan is high, this result cannot be automatically simply generalized to populations exposed to mild–moderate iodine deficiency. However, the impact of the findings in this study is that switching from MMI to KI during the first trimester of pregnancy is a way to prevent congenital anomalies due to ATD use, and there are still few reports of studies on iodide treatment in pregnant women (7,8).
In summary, although 55.4% of the GD patients who switched from MMI to KI during the first trimester went into remission during their pregnancy, the other 44.6% of the GD patients required medication until delivery. In 9.1% of the GD patients, it was difficult to control the maternal thyrotoxicosis with KI alone after the switch, but none of the parameters was a predictor of the worsened group. It must be kept in mind that a certain proportion of GD patients escape from the antithyroid effect of iodide, and thus careful follow-up is necessary after switching a pregnant patient's medication to KI.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest in this study.
Funding Information
This research did not received any specific grant from sponsors or funders.