
Abstract
Introduction:
Autoimmune thyroid disease is the most common autoimmune disorder. Evidence regarding causes of the high prevalence and incidence of thyroid autoimmunity in women, and especially women of reproductive age, is still inconclusive and previous studies have suggested genetic, environmental, and existential factors to play a role in its pathogenesis. In this study, we aimed to investigate the effect of parity and other reproductive factors on the incidence of thyroid autoimmunity within the framework of the Tehran Thyroid Study (TTS).
Materials and Methods:
This study was conducted within the framework of the TTS and 1999 nonpregnant euthyroid thyroid peroxidase antibody (TPOAb) negative women were followed up for an average of 8.3 years. A pooled logistic regression model was used to assess the association (odds ratio) between time-dependent covariates parity, menopause, and abortion, and incidence of TPOAb positivity.
Results:
The total incidence rate of TPOAb positivity was 8.65 [7.35–10.18] per 1000 person-years. We found no significant association between changes in the number of parity and risk of developing TPOAb using multiple pooled logistic models both as crude effect and after adjustment for age, body mass index, and smoking. Similarly, there was no association between changes of parity, menopause, and abortion status, and incidence of TPOAb positivity.
Conclusions:
Parity does not seem to have an independent role in triggering thyroid autoimmunity, but vast immunological and physiological changes during pregnancy may act as a precipitating factor in the context of other genetic and environmental modifiers.
Introduction
Autoimmune thyroid disease (AITD) is the most frequent pathology affecting the thyroid gland and the most common autoimmune disorder in humans (1). Many of the genetic, endogenous, and environmental factors involved in the pathogenesis of these complex highly organ-specific disorders have been elucidated through a large and still growing body of literature, but the exact trigger mechanisms are still unclear (2,3). The high prevalence and incidence of thyroid autoimmunity in women, and specially women of reproductive age, have highlighted pregnancy and related factors such as fetal microchimerism, sex hormones, and abnormalities of X chromosome inactivation as potential contributors to the pathogenesis of AITD (4).
AITD generally tend to improve during pregnancy followed by an exacerbation in the postpartum period, possibly due to vast immune response reprogramming needed for a successful pregnancy (5). Postpartum thyroiditis is also a common occurrence and can cause long-term hypothyroidism in a considerable proportion of affected women (6). Microchimerism of fetal cells that may have crossed the placenta during pregnancy has been documented in several maternal tissues, including the thyroid, and it has been shown to be more common in thyroid tissue of AITD patients than in that of healthy controls (7). It is postulated that the immune response against these semiallogenic cells triggers autoimmunity against bystander maternal tissue (8). Finally, pregnancy and menopause are accompanied by rapid physiological changes in estrogen levels; estrogen has been shown to have immunomodulatory properties (9) and can affect thyroid binding protein concentration and subsequently circulating levels of thyroid hormones (10).
AITDs are characterized by the presence of a variety of antithyroid antibodies (11). Studies have shown that thyroid peroxidase antibodies (TPOAbs) can be detected in a majority of disorders in the AITD spectrum and they are a reliable and sensitive marker of AITD (12). As such, TPOAbs have been widely used in the clinic and in AITD research.
Cross-sectional studies provide conflicting results regarding the association between TPOAb levels and parity. Some large cross-sectional studies reported lower rates of thyroid antibody positivity in nulliparous patients (13 –15), while others have failed to report any associations (16 –19). In this study, we aimed to investigate the association between changes in parity, abortion, and menopause status, and the incidence of positive seroconversion of TPOAbs in a longitudinal cohort selected from the Tehran Thyroid Study (TTS).
Materials and Methods
Study population
This study was organized within the framework of TTS, a prospective population-based cohort study aiming to evaluate the prevalence and natural course of thyroid diseases and their long-term consequences on metabolic and ischemic heart disease, as well as cardiovascular and all-cause mortality. TTS is a subdivision of Tehran Lipid and Glucose Study (TLGS) that is performed on the urban iodine sufficient population of district-13 of Tehran, the capital of Iran. TLGS is an ongoing integrated community-based cohort study with regular follow-ups at 3-year intervals, which was initiated in 1997 for the identification and prevention of noncommunicable disorders.
This study was conducted on TTS participants who were followed for 12 years through phases 1 to 4. During the first visit, the study was explained to subjects and demographic data were obtained followed by a clinical examination. Collection of demographic, clinical, and laboratory data was repeated every 3 years. Details of the study have been published elsewhere (20).
Data from 5783 individuals aged ≥20 years who were recruited within the framework of the TTS were assessed. In total, 3406 of the assessed individuals were women and were selected for this study. Women with wrong and/or missing data, pregnant women, and subjects with a history of thyroid surgery at baseline or any of the follow-ups, as well as subjects who were using medications including thyroid hormones, antithyroid drugs, and radioiodine at baseline were excluded. From the 2665 remaining subjects, 398 women had clinical or subclinical thyroid diseases, and 431 women were TPOAb positive. Subsequently, 1999 nonpregnant, TPOAb negative, and euthyroid women were included in the longitudinal analysis (Fig. 1).
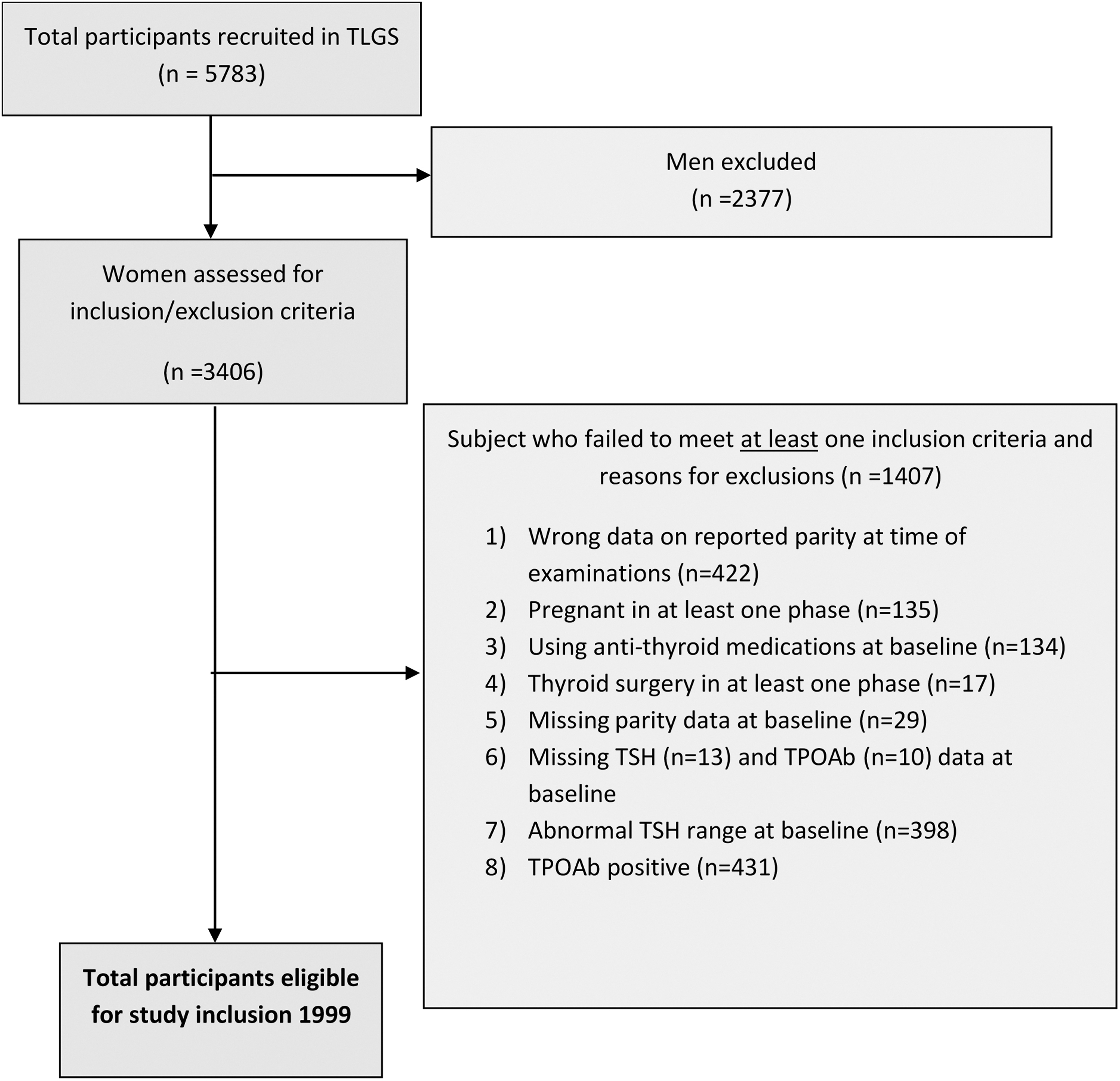
Flow diagram for participants included in the study. Number of participants included at each stage of the study process and reasons for participant exclusion (baseline = 1999, follow-up = 2011).
Laboratory analysis
Fasting blood samples were drawn from all participants between 7:00 and 9:00 AM into vacutainer tubes at each follow-up visit. Samples were centrifuged within 30–45 minutes of collection and separated sera were stored at −70°C for analysis.
Free thyroxine (fT4) and thyrotropin (TSH) were determined on −70°C stored serum samples by the electrochemiluminescence immunoassay (ECLIA) method, using Roche Diagnostics kits & Roche/Hitachi Cobas e-411 analyzer (GmbH, Mannheim, Germany). Lyophilized quality control material (Lyphochek Immunoassay plus Control; Bio-Rad Laboratories) was used to monitor accuracy of assay; intra- and interassay coefficients of variation (CVs) were 1.3% and 3.7% for fT4, and 1.5% and 4.5% for TSH determinations, respectively.
TPOAbs were measured by an immune-enzymometric assay (IEMA) using commercial kits (Monobind, Costa Mesa, CA) and the Sunrise ELISA reader (Tecan Co., Salzburg, Austria); intra- and interassay CVs were 3.9% and 4.7%, respectively. All laboratory measurements were performed in the same laboratory by a skilled laboratory technician.
The ethical committee of the Research Institute for Endocrine Sciences of Shahid Beheshti University of Medical Sciences approved the protocol for this study. Written informed consent was obtained from all subjects.
Definition of terms
Parity was defined as number of pregnancies that lasted >20 weeks, abortion was defined as pregnancies that lasted <20 weeks from gestation (21). Menopause was defined as cessation of menstrual cycles for >12 months.
Reference limits from previous studies of the TTS population were used for determining thyroid diseases and anti-TPO antibody positivity (22).
Anti-TPO antibody positivity was defined as anti-TPO antibody levels ≥35 IU/mL. Euthyroidism was defined as having 0.32 ≤ TSH ≤5.06 and fT4 within normal reference limits while not taking any thyroid medication or agent interfering with thyroid function.
Subclinical hypothyroidism, overt hypothyroidism, subclinical hyperthyroidism, and overt hyperthyroidism were defined as TSH >5.06 IU/mL and fT4 of 0.91 ± 1.55 ng/dL, TSH >5.06 IU/mL and fT4 < 0.91 ng/dL, TSH <0.32 mIU/L and fT4 of 0.91 ± 1.55 ng/dL, and TSH <0.32 IU/mL and fT4 > 1.55 ng/dL, respectively.
Statistical analysis
Baseline demographic and reproductive characteristics are presented as mean ± standard deviation and frequency (%) for continuous and noncontinuous variables, respectively. The relationship between baseline reproductive characteristics and TPOAb status (positive/negative) was assessed by applying multiple logistic regression models (adjusted for demographic variables). Friedman and Cochran tests were used for evaluating change of exposures during different phases of follow-up for continuous or categorical data, respectively.
Assuming that TPOAb positivity occurred in the mid-time between the visit in which the TPOAb positivity was diagnosed and the previous visit, the incidence rate of TPOAb positivity was calculated using the following formula:

For the censored or lost to follow-up subjects, the time to failure (development of TPOAb positivity) was the time between the first and last observation dates. Exposure value on the visit before TPOAb positivity was assumed for calculating change of exposure from the baseline.
A pooled logistic regression model was used to assess the association (odds ratio [OR]) between the time-dependent covariates parity, menopause, abortion, and TPOAb positivity. This model merges the observations of all intervals together into one pooled sample, assuming every interval as a minifollow-up study, and does a logistic regression on the pooled data set.
All analyses were performed using STATA (version 13; STATA, Inc., College Station, TX) and IBM SPSS (version 23; SPSS Inc., Chicago, IL). Two-tailed p-values <0.05 were considered significant.
Results
Table 1 gives the distribution of variables at baseline according to TPO antibody status. From a total of 2267 nonpregnant and euthyroid women at baseline, 268 (11.8%) subjects were TPOAb positive, 524 (23.1%) were parous, and 540 (23.8%) had a history of abortion. In total, 1746 women were premenopausal (77%). The mean age of participants at the beginning of study was 38.06 ± 13.1 years and 4.8% of them were smokers. Linear regression models disclosed that smoking and body mass index (BMI) were associated with TPOAb positivity (OR: 1.79, confidence interval [CI]: 1.08–2.296 and 1.03, CI: 1.002–1.06, respectively).
Presence of Thyroid Autoimmune Disease According to Demographic and Reproductive Characteristics at Baseline, Tehran Thyroid Study, 1999–2011 (Nonpregnant Euthyroid Women)
Those with TPOAb levels ≥35 IU/mL were regarded as TPOAb positive. Data are given as mean ± standard deviation and frequency (%) for continuous and noncontinuous variables, respectively.
Multiple logistic regression models (adjusted on demographic variables) were used to calculate p-value for each reproductive characteristics, separately, and also univariate logistic regression models for each demographic characteristics. Bold numbers represent data that are considered statistically significant.
BMI, body mass index; CI, confidence interval; OR, odds ratio; TPOAb, thyroid peroxidase antibody.
At baseline, 10.5% of nulliparous women and 12.2% of parous women were TPOAb positive. TPOAb positivity in those without any history of abortions, with at least 1 abortion and pre- and postmenopausal subjects were 12.4%, 11.7%, 11.7%, and 12.3%, respectively.
Multivariate adjusted models (adjusted for age, BMI, and smoking) at baseline in a group of nonpregnant euthyroid women showed that higher number of parity was significantly associated with lower risk of TPOAb positivity [OR: 0.9, CI: 0.82–0.997, p: 0.043]. Parous women, postmenopausal women, and those with a history of abortion had a lower risk of TPOAb positivity, but it did not reach statistical significance [OR: 0.92, CI: 0.63–1.34; OR: 0.76, CI: 0.48–1.18; OR: 0.8, CI: 0.58–1.16] (Table 1).
Among 1999 nonpregnant euthyroid TPOAb negative participants selected for follow-up, 450 women were menopausal, 1530 were parous, and 477 had a history of abortion. Throughout the duration of follow-up, there were a significant increase in the mean number of parity and menopausal subjects (Table 2).
Changes of Reproductive Characteristics of Healthy Participants (i.e., Euthyroidism and Thyroid Peroxidase Antibody Negative Participants at Baseline) During Follow-Up
Bold numbers represent data that are considered statistically significant.
Data are given as mean ± standard deviation and frequency (%) for continuous and noncontinuous variables, respectively; the percentages may not add up to 100% because of missingness at some visits.
Friedman test.
Cochran test.
A total of 144 new cases of TPOAb positivity were identified during a mean follow-up of 8.33 ± 2.39 years, showing a total incidence rate of 8.65 [CI: 7.35–10.18] per 1000 person-years. Table 3 gives incidence rates per 1000 person-years of TPOAb seroconversion in different groups of reproductive status.
Thyroid Autoimmunity Incidence Per 1000 Person-Years by Parity, Menopause, and Abortion at Baseline, Tehran Thyroid Study, 1999–2011
The incidence rate of TPOAb positivity among women with at least one abortion, nulliparous and premenopausal women at baseline, was higher than that of the total study population. The incidence rate ratio of seroconversion to TPO positivity in parous compared with nulliparous women was 0.87 [CI: 0.59–1.32]; this ratio was 0.64 [CI: 0.39–1.0] for postmenopausal women compared with premenopausal subjects, and 1.12 [CI: 0.73–1.69] for women with compared with those without a history of abortions.
We found no significant association between changes in the number of parity and risk of developing TPOAbs using multiple pooled logistic models both as crude effect [OR: 0.97, CI: 0.88–1.06, p: 0.5] and after adjustment for age, BMI, and smoking [OR: 1.05, CI: 0.91–1.22, p: 0.49]. Similarly, there was no association between changes in parity, menopause, and abortion status, and incidence of TPOAb positivity.
In longitudinal models, parity and abortion, when considered as categorical variables, were associated with higher but not significant incidence of seroconversion [OR: 1.30, CI: 0.75–2.25, p: 0.97; OR: 1.32, CI: 0.84–2.07, p: 0.341, respectively].
Postmenopausal state in both cross-sectional and longitudinal models was associated with lower risk of thyroid autoimmunity (Table 4).
Results Pooled Logistic Regression Model of the Development of Thyroid Peroxidase Antibody Positivity
Multiple pooled logistic regression models were used to calculate p-value for each reproductive characteristic, separately.
Crude.
Adjusted by age, smoking, and BMI at baseline.
Discussion
In this study, we provide longitudinal evidence on the association between changes in parity and other female reproductive factors and incidence of thyroid autoimmunity. We also identified an 8.65 per 1000 person-years rate of seroconversion to TPOAb positive state in nonpregnant euthyroid Iranian women comparable with the previous report of 9.35 per 1000 person-years in the extended population of the women enrolled in the TTS (23).
The results reveal no association between changes in parity over time and incidence of seroconversion to TPOAb positivity in Iranian women, which is in line with the results of previous cross-sectional studies (16 –18,24), as well as a 12-year longitudinal survey on 1746 Danish women who studied the relationship between changes in parity and TPOAb status after 12 years compared with baseline and found no significant association (19). In contrast, in the National Health and Nutrition Examination Survey (NHANES) and another large prospective study, parity increased the risk for TPOAb positivity (13,14). Nonetheless, the association diminished after adjusting for age, smoking, and other risk factors in both studies (13,14). Studies using higher cutoff values for TPOAb positivity (>200–1000 IU/mL) resulted in a significant association between parity and TPOAb positivity that persisted after adjustments (14,25).
Our study did not find a significant association between abortion and incidence of thyroid autoimmunity, a result consistent with findings of the mentioned Danish survey (19) and a number of cross-sectional studies (17,18). Another study from the Danish population reported an association between spontaneous abortions and development of autoimmune hypothyroidism (26). Finally, we did not identify any risk associated with menopausal state and thyroid autoimmunity, consistent with the results of the only similar investigation in the Danish longitudinal survey (19).
The apparent disagreements in results from different studies should be interpreted in light of the participant's demographic features, including age, race/ethnicity, and, importantly, iodine intake. Iodine prophylaxis has been shown to increase the prevalence of positivity for thyroid antibodies in population studies (27 –29).
Before this study, the study of 1746 Danish women was the only longitudinal survey investigating the association between female reproductive factors and thyroid disease. However, the mentioned study pooled the 12-year changes in exposures and outcomes, disregarding precedence of the change in reproductive status (exposure) to the incidence of TPOAb positivity (outcome.) To the best of our knowledge, this is the first study to address changes in parity and other reproductive factors in association with the incidence of thyroid autoimmunity as evidenced by TPOAb positive seroconversion. Considering the high response rate and the large study population in the TTS, we speculate that these results are highly representative, at least for the Iranian population. The use of an IEMA for the measurement of TPO-Ab provided adequate methodologic accuracy in this study (30). Nonetheless, we could not separately measure the effect of parity on one-year postpartum seroconversion, which is an important milestone for development of thyroid autoimmunity (31). We also used self-reported indices for parity, abortion, and menopause status, as well as current or recent thyroid drug use, and thyroid surgical history, the accuracy of which depends highly on the accuracy of the information provided by the subject and educational status.
Evidence regarding the causes of the high prevalence and incidence of thyroid autoimmunity in women, and specially women of reproductive age, is still inconclusive (32,33). The current understanding is that the pregnancy-related surge in sex hormones and the subsequent immunomodulation and fetal microchimerism are triggers of autoimmunity in the context of genetic predisposition (32,33). Indeed, fetal cells have been found in blood and thyroid tissue of patients with Hashimoto and Graves' disease up to 38 years after pregnancy (34). It is, however, still not clear whether the immune response against these cells triggers thyroid autoimmunity or whether they are just innocent bystanders, or whether they may even exert protective immune regulatory effects. If parity can be considered as a surrogate for the intensity of fetal cell exposure, considering that microchimerism is common in normal pregnancies (13,14,18), our results prove against a triggering effect for fetal microchimerism in the pathogenesis of thyroid autoimmunity.
Pregnancy and abortion are accompanied by physiological surges of sex hormones and a significant immunomodulatory reprogramming (35), followed by a rebound phase in the postpartum period, which is associated with aggravation and emergence of AITD and the characteristic postpartum thyroiditis (6,31). It should be noted that the mentioned postpartum alterations in immune response are generally considered as precipitating factors, but not causal, for autoimmunity (36), added to the fact that the short duration of postpartum immune and hormonal changes does not have a long-lasting effect on maintaining thyroid autoimmunity (37,38).
In conclusion, it appears that parity is not an independent risk factor for thyroid autoimmunity. However, given their complex nature, pregnancy-related immunological and physiological changes, in combination with a favorable genetic and environmental predilection, might be considered as precipitating factors for developing AITD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Tehran Thyroid Study grant. No other funding was received for this article.