
Abstract
Background:
The diagnostic role of ultrasonography (US)-guided core needle biopsy (CNB) as a first-line diagnostic method for thyroid nodules remains controversial. This study was performed to determine the diagnostic efficacy and safety of CNB as a first-line diagnostic method for thyroid nodules.
Methods:
From February 2016 to January 2018, CNB was prospectively performed by an experienced radiologist in all consecutive patients with thyroid nodules indicated for fine-needle aspiration (FNA). Three patients refused this protocol. Finally, 212 consecutive patients with 248 thyroid nodules were enrolled in this prospective study. Combined CNB/FNA was selectively performed in 43 patients. The diagnostic efficacy of CNB was evaluated by the rate of inconclusive results (nondiagnostic or indeterminate results), and its feasibility was estimated by calculating the successful biopsy rate and by measuring the procedure time from the time of the initial skin puncture to the last withdrawal of the biopsy needle from the skin. The safety of the procedure was evaluated by the major and minor complication rates. A US evaluation was performed before and after manual self-compression to assess for hemorrhage at the biopsy site, and delayed complications were assessed 5–7 days after the biopsy. Any hemorrhage that did not require hospitalization was classified as a minor complication.
Results:
CNB was performed once (n = 125, 50.4%), twice (n = 122, 49.2%), or three times (n = 1, 0.4%) per nodule. The diagnostic results of CNB were as follows: nondiagnostic (0.8%), benign (63.3%), indeterminate (10.1%), follicular neoplasm (3.2%), suspected malignancy (2.4%), and malignancy (20.1%); the rate of inconclusive results was 10.9%. The successful biopsy rate of CNB was 100%, and the median procedure time was 102 seconds (interquartile range 51–181 seconds). There were no major or delayed complications. There were 6 cases (2.8%) of minor complications, which included 2 cases (0.9%) with symptomatic hematomas and 4 cases (1.9%) with asymptomatic small hematomas.
Conclusion:
The findings confirm that CNB is effective in reducing the rate of inconclusive results and it is safe. CNB may be used as an alternative first-line diagnostic method for thyroid nodules by an experienced operator.
Introduction
Ultrasonography (US)-
Recently, several studies assessed the potential role of CNB as a first-line diagnostic tool in the management of thyroid nodules (15 –19). However, these studies included a specific patient population and the diagnostic role of CNB as a first-line diagnostic method for thyroid nodules remains controversial. The safety of CNB still remains a concern, even though it is considered to be safe, well tolerated, and associated with a low incidence of complications when performed by an expert (1,6). A recent large single-center study (20) and a systematic review and meta-analysis (21) validated the low rate of major and minor complications and no procedure-related death. However, most of the previous studies on the safety of CNB are retrospective studies and further validation by a prospective study is necessary. This prospective study was performed to determine the diagnostic efficacy and safety of CNB as a first-line diagnostic method in patients with thyroid nodules indicated for FNA.
Materials and Methods
Study design and study population
The primary endpoints of the study were the diagnostic efficacy of CNB, estimated by the rate of inconclusive results, and the safety of the CNB procedure, estimated by the complication rate. The secondary endpoints were the feasibility and procedural efficacy of CNB. The inclusion criterion for entering the study was patients who had thyroid nodules indicated for FNA according to the recommendations of the Korean Society of Thyroid Radiology (KSThR) (22). The FNA criteria based on the Korean Thyroid Imaging Reporting and Data System (TIRADS) were as follows: (i) high- or intermediate-suspicion (TIRADS 5 or 4) nodules ≥1 cm; (ii) low-suspicion (TIRADS 3) nodules ≥1.5 cm; (iii) benign nodules (TIRADS 2) ≥2 cm selectively for spongiform nodule and for diagnosis before ablation therapy; (iv) high-suspicion subcentimeter nodules (>0.5 cm) selectively for decision of active surveillance or surgery (22); and (v) nodules of any size when there was suspected gross extrathyroidal tumor extension, suspicious metastatic lymph node, and diagnosed distant metastasis from thyroid cancer. Patients who refused the study protocol were excluded. Coagulation screening was not routinely performed. In patients receiving antiplatelet or anticoagulation therapy, CNB was performed after discontinuing these medications for 1 week.
From February 2016 to January 2018, 215 consecutive patients with a total of 251 thyroid nodules with an indication for FNA were enrolled in this study at a single institution (the Human Medical Imaging and Intervention Center). Among these, three patients refused to participate in the study. Finally, we prospectively enrolled 212 patients (171 women, 41 men; mean age 48.8 ± 13.0 years; range, 12–79 years) with a total of 248 nodules with an indication for FNA. The median size (maximal diameter) of the thyroid nodules was 13 mm (interquartile range [IQR] 9–20 mm). There were 70 micronodules (<1 cm) and 178 macronodules (≥1 cm). CNB was performed for the micronodules: (i) nodules (>5 mm) with a highly suspicious US pattern before decision for active surveillance or surgery (n = 65); (ii) nodules with AUS/FLUS results on previous FNA (n = 3); (iii) nodules with discordant US and previous FNA results (n = 1); and (iv) for operation extent decision (lobectomy or total thyroidectomy) in a patient with a proven thyroid cancer in the contralateral biopsy (n = 1). The Institutional Review Board approved the protocol for this prospective study. An informed consent for the US examination, biopsy procedure, and study protocol was obtained from all patients before each examination and biopsy procedure.
US-guided CNB procedure
CNB procedures were performed under high-resolution, color-Doppler US guidance, by using a 10–12-MHz linear transducer (AplioXG; Toshiba, Otawarashi, Japan) by one experienced thyroid radiologist (D.G.N.) with 20 years of experience in thyroid US imaging and intervention. CNB was performed by using a disposable 18-gauge, single- or double-action spring-activated needle (∼1 or 2 cm excursion; TSK Acecut or Stericut; Create Medic, Yokohama, Japan), as previously described (7,23). In all cases, 1% lidocaine was administered for local anesthesia. The CNB needle notch was positioned to cut a portion of the normal parenchyma (about 2–3 mm in length) at the nodule margin in suspected follicular lesions based on US features. Strict vessel mapping along the approach route was performed by using color-Doppler US during the procedure to avoid vascular injury (6). During the procedures using a double-action CNB needle, the modified technique of introducing a pre-fired stylet needle into the thyroid tissue was allowed. The number of CNB biopsies was one or two in most cases. An additional, second CNB was selectively performed in the nodules with an suboptimal specimen by visual assessment, concern of mistargeted specimen, large (>3 cm) size or heterogeneous components, heavy calcification, or those suspected for a mainly fibrous component. For predominantly cystic nodules, CNB was performed in the solid part or at the wall, usually after near-complete aspiration of the cystic content. The obtained tissue was immediately fixed in formalin after a visual assessment of the CNB specimen (6). In the nodules where combined CNB/FNA were conducted, FNA was performed by using the combined method of capillary and aspiration technique and at least two samplings were performed for each nodule (24). In most cases, CNB was performed after FNA. Combined CNB/FNA was selectively performed for the nodules with a prior AUS/FLUS FNA cytology result, worrisome suboptimal CNB specimen, heavy calcifications, and a prior US-FNA discordant result, or for nodules that were candidates for radiofrequency ablation therapy. The combined CNB/FNA diagnostic results were classified by combination of the CNB and FNA results (19). We immediately compressed the biopsy site after the withdrawal of the CNB needle, and the patients were observed during the manual self-compression of the biopsy site for 20–30 minutes after the procedure.
Cytology and histology analyses
All FNA cytology specimens were interpreted according to the six categories of the Bethesda System for Reporting Thyroid Cytopathology (BSRTC) (25). The CNB histology diagnoses were made according to the diagnostic categories of thyroid CNB from the Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group (26,27). This pathology reporting system of CNB is also based on the six categories in the BSRTC, and the category III for CNB is an “indeterminate lesion,” which corresponds to “atypia of undetermined significance” or “follicular lesion of undetermined significance” in the BSRTC (26).
Analysis of the diagnostic efficacy and feasibility
The diagnostic efficacy of CNB was evaluated by the rate of inconclusive results (nondiagnostic or indeterminate results). The feasibility of CNB was estimated by calculating the successful biopsy rate of the biopsy procedure and by measuring the procedure time. The procedure time of CNB was measured from the initial skin puncture to the time of withdrawal of the biopsy needle from the skin after cutting the tissue sample. When CNB sampling was performed more than once, the procedure time was measured from the time of the initial skin puncture to the last withdrawal of the biopsy needle from the skin. The procedure time of CNB was measured in 157 consecutive nodules from July 2016 to January 2018. The number of biopsy samples, type and excursion length of the biopsy needle, and the combined application of an FNA procedure were prospectively recorded in each thyroid nodule.
Analysis of complications
The safety of the CNB procedure was assessed by major and minor complication rates. The types of complications, time of detection, time to recovery, management of the complications, and the presence of permanent consequences were also evaluated (20). The major and minor complications were defined based on the quality improvement guidelines from the Society of Interventional Radiology (28 –30). A major complication was defined as an event that caused an unintended increase in the level of care, hospitalization for therapy, sequelae, or morbidity (28,29). All other complications without any sequelae or need for nominal treatment were considered as minor (29). A large hemorrhage that had the potential of requiring hospital admission for treatment was considered as a major complication. Any symptomatic hemorrhage that could be managed with simple manual compression and did not require hospitalization was considered as a minor complication. Minor complications also included any asymptomatic small hemorrhage detected on US that did not require additional manual compression other than routine neck compression after biopsy. Hemorrhages were divided into two types, perithyroidal and parenchymal hemorrhages according to the site of hemorrhage. All complications were assessed, and US evaluation was routinely performed to assess for hemorrhage immediately after the CNB and after the manual self-compression of the biopsy site. Delayed complications were assessed 5–7 days after CNB, and the presence of any delayed complications was investigated when the patients revisited our outpatient clinic or referring hospitals; otherwise, it was checked by phone.
Statistical analysis
Continuous variables are presented by using the median (IQR) or the mean ± standard deviation (SD), according to parametric or nonparametric distribution, respectively. Categorical variables are reported as frequencies and percentages for each category. The McNemar test was used to compare the inconclusive results of CNB according to the nodule size and to compare the inconclusive results between CNB and selectively combined CNB/FNA in all nodules. The McNemar test was also used to compare the inconclusive results between CNB and combined CNB/FNA in nodules that underwent both CNB and FNA. The Mann
Results
Demographic data
CNB alone was performed in 205 nodules (82.7%), and combined CNB/FNA was performed in 43 nodules (17.3%) (Table 1). The mean number of CNB samples was 1.5 ± 0.5. CNB was performed once (n = 125, 50.4%), twice (n = 122, 49.2%), or thrice (n = 1, 0.4%). A double-action needle was used in 209 nodules (84.3%), and a single-action needle was used in 39 nodules (15.7%) for CNB. The length of the biopsy excursion was 1 or 1.1 cm (n = 187, 75.4%), 1.6 cm (n = 53, 21.4%), or 2 cm (n = 8, 3.2%).
Diagnostic Results of Core Needle Biopsy and Selectively Combined Core Needle Biopsy/Fine-Needle Aspiration in 248 Nodules
FNA was additionally performed in 43 nodules.
AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance; CNB, core needle biopsy; FN/SFN, follicular neoplasm or suspicious for follicular neoplasm; FNA, fine-needle aspiration.
The reasons for the additional biopsy performed in 123 nodules were as follows: (i) nodules with suboptimal specimens via visual assessment of the sampled tissue (n = 35, 28.5%); (ii) small nodules with concern of mistargeted specimen (n = 33, 26.8%); (iii) large nodules (>3 cm), or those containing heterogeneous components (n = 28, 22.8%); (iv) nodules suspected to contain predominant fibrosis (n = 19, 15.4%); and (v) nodules with heavy macrocalcifications (n = 8, 6.5%). The reasons for the additional FNA performed in 43 nodules were as follows: (i) a prior AUS/FLUS FNA cytology result (n = 19, 44.2%), worrisome suboptimal CNB specimen (n = 7, 16.3%), heavy calcifications (n = 5, 11.6%), a prior US-FNA discordant result (n = 2, 4.7%), or for nodules that were candidates for radiofrequency ablation therapy (n = 10, 23.3%).
Diagnostic efficacy of CNB
The diagnostic results of CNB and the selectively combined CNB/FNA are shown in Table 1. Inconclusive results (nondiagnostic [0.8%] and indeterminate [10.1%]) were found in 10.9% (24/248) of all nodules by CNB results. There was no significant difference in the inconclusive CNB results between nodules <1 cm and those ≥1 cm (14.3% vs. 9.6%, respectively; p = 0.364). The histology findings of the two nodules with nondiagnostic CNB results were paucicellular fibrotic nodules (stromal sclerosis with microcalcification and scanty atrophic follicles in a fibrous stroma). The inconclusive results (nondiagnostic [0.4%] and indeterminate [9.3%]) were found in 9.7% (24/248) of all nodules by selectively combined CNB/FNA diagnostic results. There was no significant difference in the rate of inconclusive results between CNB and the selectively combined CNB/FNA (10.9% vs. 9.7%, respectively; p = 0.250).
Inconclusive results of the nodules that were evaluated with combined CNB/FNA
In 43 nodules, FNA was selectively performed in addition to CNB. Inconclusive results were found in 8 (18.6%), 24 (55.8%), and 5 (11.6%) of all nodules by CNB, FNA, and combined CNB/FNA, respectively. Nondiagnostic results were noted in 1 (2.3%), 14 (32.6%), and 0 (0%) by CNB, FNA, and combined CNB/FNA, respectively. Indeterminate or AUS/FLUS results were found in 7 (16.3%), 10 (23.3%), and 5 (11.6%) by CNB, FNA, and combined CNB/FNA, respectively. The combined CNB/FNA results showed a slightly lower rate of inconclusive results; however, the difference was statistically insignificant (p = 0.250).
Feasibility and procedural efficacy of CNB
The successful biopsy rate of CNB was 100%. The median CNB procedure time per nodule was 102 seconds (IQR 51–181 seconds) (Table 2). The CNB procedure time was less than 5 minutes in 148 (94.3%) of the 157 nodules. When the CNB procedure time was compared according to the nodule size (micronodules <1 cm vs. macronodules ≥1 cm), there was no significant difference in the procedure time between the micronodules and macronodules for one biopsy procedure (median 58 seconds [IQR 38–74 seconds] and median 52.5 seconds [IQR 31–82 seconds], respectively; p = 0.611). In contrast, a significantly longer time was needed for two-times biopsies in micronodules (n = 30, median 240 seconds; [IQR 178–279 seconds]) than in macronodules (n = 46, median 147 seconds [IQR 118–224 seconds]) (p = 0.001). Among the 70 nodules <1 cm, the size of the nodules was significantly smaller in those biopsied more than once (n = 43, median 7 mm [IQR 5–8 mm]) than in those biopsied only once (n = 27, median 7 mm [IQR 6–9 mm]) (p = 0.030).
Procedure Time for Core Needle Biopsy
The procedure time for CNB was measured from the initial skin puncture time to the time of biopsy needle withdrawal from the skin after cutting the tissue sample.
IQR, interquartile range.
Complications of CNB
There were no major complications or procedure-related sequelae noted (Table 3). There were 6 cases (2.8%, 6/212) of minor complications in this study, which were 2 (0.9%) symptomatic hematomas and 4 (1.9%) asymptomatic small hematomas (Table 3). There was no large hematoma requiring additional treatment with hospital admission. Of the two symptomatic hematomas, one was a perithyroidal hematoma causing mild neck pain (Fig. 1) and the other comprised small perithyroidal and parenchymal hematomas accompanied by mild neck discomfort. All symptomatic and asymptomatic hematomas were detected by US evaluation immediately after the CNB. In two patients with symptomatic hematomas, the amount of the hematomas was stable and decreased, and the symptoms improved after manual compression of the neck. In four patients with asymptomatic small perithyroidal hematomas, the US evaluation after the routine neck compression showed a decrease in the size of the hematomas in all cases (Fig. 2). No delayed complications were observed in this study. Mild neck pain or discomfort was observed in 8 patients (3.8%, 8/212), lasting several days after the CNB, which completely resolved without any medications within 7 days.
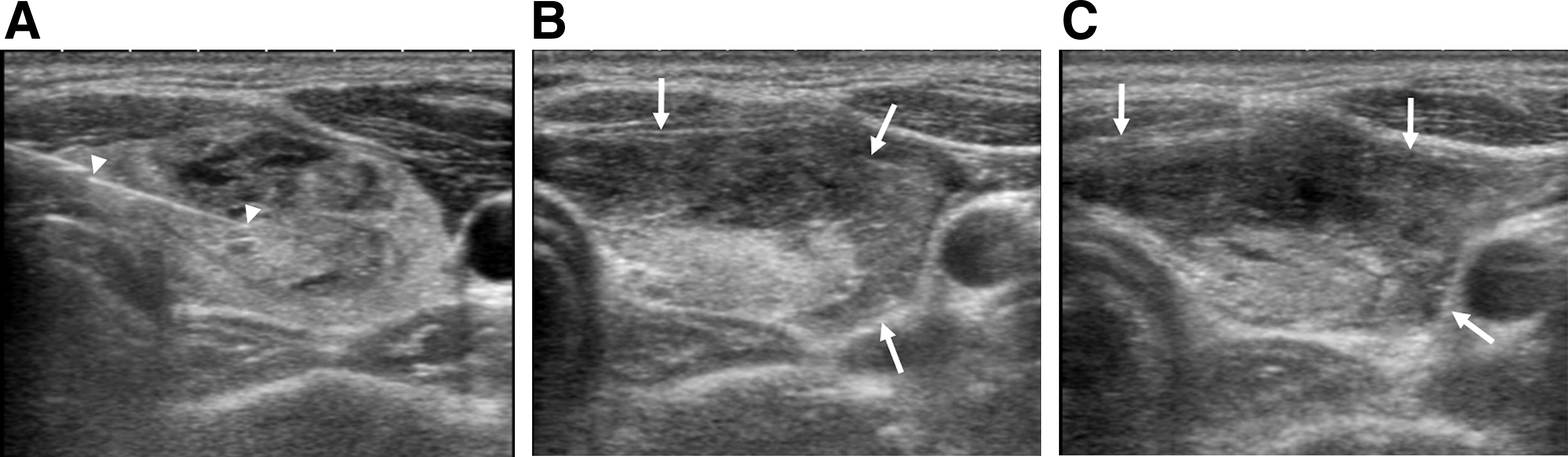
A 12-year-old female with symptomatic perithyroidal hematoma after CNB. (
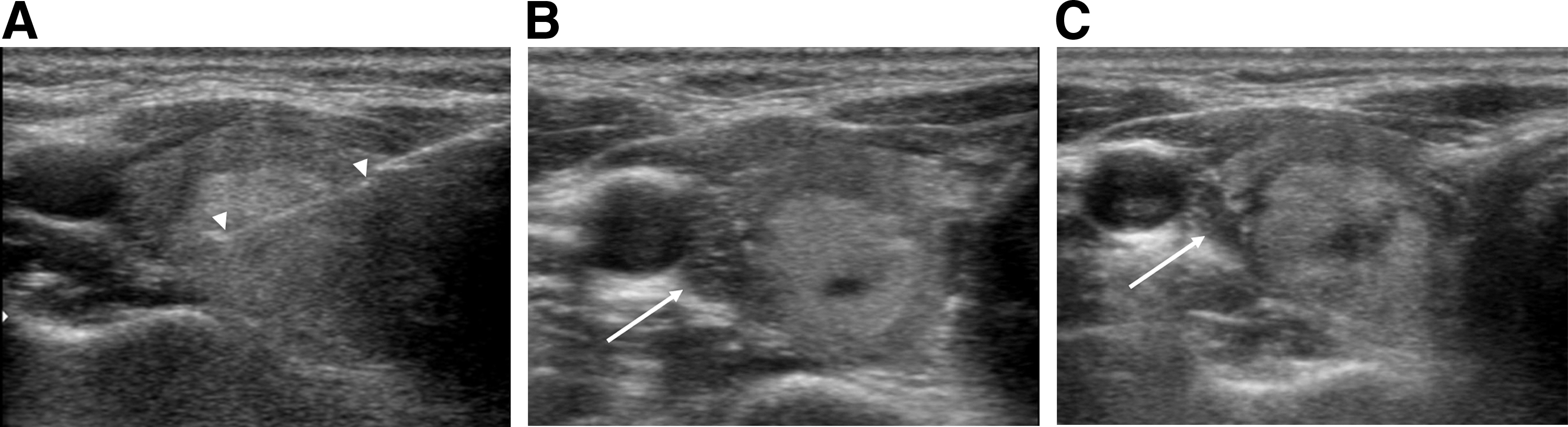
A 26-year-old female with asymptomatic small perithyroidal hematoma after CNB. (
Complications of Core Needle Biopsy in 212 Patients
Additional manual compression was performed by the operator before manual self-compression.
Discussion
Our study results demonstrate that the rate of nondiagnostic results was minimized (0.8%) and the rate of inconclusive results was low (10.9%) when using CNB. There were no major complications and there was a low minor complication rate (2.8%). Our study confirms and validates the high diagnostic efficacy and safety of CNB as a first-line diagnostic tool in thyroid nodules by experienced operators.
The rate of inconclusive results of CNB in this study was more than 10% lower than that of FNA (22.4%) estimated by a meta-analysis (5), which suggests that CNB could prevent or reduce unnecessary repeated biopsies or diagnostic surgery in more than 10% of thyroid nodules that underwent FNA. The results of this study are comparable with the results of a retrospective study (19) that evaluated the diagnostic efficacy of FNA, CNB, and combined FNA/CNB for the first-line diagnosis of thyroid nodules at our institution. In this study, CNB showed a significantly lower rate (10.2%) of inconclusive results compared with FNA (23.7%). In this study, the lower rate of inconclusive results by CNB may be mainly due to the minimized rate of nondiagnostic results (0.8%) of CNB as compared with that of FNA (12.9%) (5), because the rate of indeterminate results (10.1%) was similar to the rate of AUS/FLUS results (9.6%) in FNA (5).
The low rate of nondiagnostic results (1.3–5.2%) of CNB has been consistently reported by previous retrospective studies of CNB as a first-line biopsy tool (17 –19). It can be explained by the large tissue samples acquired by CNB, which can reduce the risk of nondiagnostic results by FNA in thyroid nodules with intrinsic paucicellular characteristics and severe fibrosis, heavy calcifications, or a predominantly cystic composition (31 –34). CNB can substantially lower the rate of nondiagnostic results compared with FNA in nodules with fibrosis or heavy calcifications (14,34 –36), and it has not been affected by the US characteristics of vascularity and cystic components in previous studies (16,17). The two nodules with nondiagnostic CNB results in this study were histologically paucicellular fibrotic nodules, which may be the main cause for the nondiagnostic CNB results since nodules with fibrosis, sclerosis, or calcification may induce a low cellularity in CNB specimens (6). Therefore, some technical issues should be considered to minimize the nondiagnostic results of CNB as a first-line diagnostic tool. The area of fibrosis is usually characterized by marked hypoechogenicity on US (34,37) along with firmness and difficulty in needle penetration. Therefore, at least two samples of CNB are necessary for nodules suspected to contain fibrosis or calcification, and the use of a CNB device with a strong spring power will be useful for penetration of heavily calcified nodules and for preventing the fragmentation of the tissue core. Although CNB may reduce the rate of repeated indeterminate results and is more effective compared with repeated FNA in nodules with prior AUS/FLUS FNA results (7,9,38), it showed a similar rate of indeterminate results compared with FNA in this study on the first-line use of CNB. Previous retrospective studies (17 –19) reported a wide spectrum (4.6–16.5%) of indeterminate CNB results in the first-line use of CNB, which was not significantly lower than the rate of AUS/FLUS FNA results (18,19). Possible causes for the wide spectrum of indeterminate CNB results might be the non-standardized pathology criteria of CNB for the diagnosis of indeterminate nodules, and the potential variability of interpretation of CNB histology among pathologists.
Our study shows that the selectively combined CNB/FNA did not significantly reduce the rate of inconclusive results compared with CNB alone in all nodules and in the subgroup of nodules that underwent both CNB and FNA. A previous retrospective study (19) also has suggested that that diagnosis by combined CNB/FNA has a low added diagnostic benefit over CNB alone for first-line diagnostic use in thyroid nodules. Therefore, combined CNB/FNA for the first-line diagnosis of thyroid nodules may not provide an added benefit over CNB alone. Regarding the feasibility and procedural efficacy of CNB, the successful biopsy rate of CNB was satisfactory and the CNB procedure time from the skin puncture to the withdrawal of biopsy needle for one sampling may be comparable with the procedure time for one FNA sampling.
The reported complication rates of CNB range from 0% to 4.1% (6,21), which is acceptable compared with that of FNA (0.074–8.5%) (18,39 –41). Most of the reported complications of CNB are minor complications, and the major complication rate (0.06%) is much lower than the minor complication rate (1.08%) (21). The overall minor complication rate (2.8%) of our study was slightly higher and the symptomatic minor complication rate (0.9%) was similar compared with the reported complication rate (0.81%) of a retrospective study on a large series of CNB (20), which may be explained by the difference of a study design. In our study, any small asymptomatic hematomas could be detected with a prospective evaluation and the asymptomatic small hematomas may be clinically insignificant because those were resolved after routine manual self-compression and did not require additional management.
Arteriovenous fistulae, hematomas requiring hospital admission, a pseudoaneurysm, permanent voice changes, and a permanent dysphonia have been reported as rare major complications of CNB (21,42,43). Vascular injury, including a fatal hematoma, pseudoaneurysm, and carotid injury, as well as dysphonia were also reported with US-guided FNA (40,41,44,45). Several major factors should be considered to minimize the complication rate of CNB. First, complete US guidance is mandatory during the biopsy procedure. Most of the rare serious complications may have resulted from the failure of real-time tracing of the tip of the biopsy needle. Second, strict vessel mapping of the access route from the thyroid capsule to the target nodule using color-Doppler US is essential to prevent hemorrhage, the most common complication of thyroid biopsy. In the case of hypervascular nodules, the visualized perinodular or intranodular arteries should be avoided along the anticipated route of the biopsy needle, and a biopsy needle should be introduced into the center of the target nodule along an avascular window at the margin of a hypervascular nodule. It is generally safer to use a single-action needle rather than a double-action needle for a hypervascular nodule, and it may be helpful to advance the stylet into the nodule, avoiding vessels after pre-firing the stylet outside the nodule if the double-action biopsy needle type is acceptable for advancing the pre-fired stylet. Third, a single-action needle is generally safer than a double-action needle for less experienced operators. Many of the rare major complications were reported in studies using a double-action needle (20,43). Because the exact location of the stylet after the initial stylet firing cannot be perfectly anticipated, it might be more liable to adjacent vessel or tissue damage. In contrast, the stylet and specimen notch can be adjusted to avoid vessel or tissue injury by manually advancing the stylet needle with a single-action needle. Recent retrospective studies (18,19) reported that CNB showed a higher sensitivity and similar specificity for the diagnosis of thyroid malignancy compared with FNA in initially detected thyroid nodules. Considering the lower rate of inconclusive results with CNB and the comparable feasibility, procedural efficacy, and safety compared with FNA, our study results suggest that CNB may provide more benefit to the patients and could be used as a first-line biopsy tool by experienced operators evaluating thyroid nodules. However, CNB has two main limitations in its widespread use as the first-line diagnostic tool for thyroid nodules in comparison with FNA. First, CNB requires more skills compared with FNA. Second, standardized histological diagnostic criteria for CNB have not been established, which may cause potential variability in the interpretation of CNB histology among pathologists. Our study suggests that CNB has a complementary role as a first-line tool for the initial diagnosis of thyroid nodules, indicating that FNA and CNB are not mutually exclusive in the initial diagnosis of thyroid nodules. CNB can be considered as the alternative first-line tool to FNA when performed by an experienced operator, especially for nodules with US features of suspected severe fibrosis, heavy calcifications, and a predominantly cystic composition, which increase the risk for nondiagnostic results with FNA (31 –34), and for nodules of suspected uncommon tumors, such as lymphoma, medullary carcinoma, anaplastic cancer, and metastasis (46 –49).
Our study has several limitations. First, the diagnostic results of CNB might be different according to the pathologists' experience and the institution, because standardized diagnostic histology criteria of CNB for thyroid nodules have not been established. Further investigations are needed to standardize the diagnostic histology criteria of CNB. Second, in this study, CNB was performed by a single experienced radiologist; therefore, our study results may not be generalized to less experienced operators. Third, the level of pain associated with the CNB procedure and its tolerability were not assessed in this study. Previous studies (50,51) reported that there was no significant difference in the pain level, tolerability, or satisfaction score between FNA and CNB. Further investigations may be required for pain and tolerability of the CNB procedure for its wide application in the clinical practice.
In conclusion, in this prospective study, CNB was effective for reducing the inconclusive results and safe as a first-line diagnostic tool in thyroid nodules. CNB may be used as an alternative to FNA for thyroid nodules if performed by experienced operators.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.