
Abstract
Background:
Radioiodine therapy (131I) forms a principal cornerstone in the management of differentiated thyroid cancer. Radioiodine-refractory differentiated thyroid cancer (RAIR-DTC) presents a challenge in detection of structural disease in patients with evidence of biochemical disease and in treatment of the disease using alternate therapies. The present study was conducted to compare the diagnostic accuracy (in terms of sensitivity and specificity) of 68Ga-DOTA-RGD2 positron emission tomography (PET)/computed tomography (CT) as a neoangiogenesis imaging modality with 18F-FDG PET/CT, the current standard in diagnostic algorithm of RAIR-DTC, and to evaluate the radiotracer avidity on 68Ga-DOTA-RGD2 PET/CT for potential theranostics.
Methods:
Forty-four RAIR-DTC patients with negative post-therapy 131I scan were prospectively enrolled. Serum thyroglobulin (sTg) and anti-thyroglobulin (ATg) measurements were performed with levothyroxine withdrawal (thyrotropin-stimulated state), and 18F-FDG PET/CT and 68Ga-DOTA-RGD2 PET/CT studies were performed within 1 week of each other. Follow-up was performed with histopathology/sTg/ATg/conventional imaging. The findings of 18F-FDG PET/CT and 68Ga-DOTA-RGD2 PET/CT were compared with the reference standard to obtain sensitivity, specificity, and overall accuracy. Degree of radiotracer uptake on 68Ga-DOTA-RGD2 PET/CT was described as tumor to background (T/B) and tumor to liver (T/L) ratios of standardized uptake value.
Results:
68Ga-DOTA-RGD2 PET/CT detected a total of 123 lesions, with an overall sensitivity, specificity, and accuracy of 82.3%, 100%, and 86.4%, respectively. 18F-FDG PET/CT detected a total of 144 lesions, with an overall sensitivity, specificity, and accuracy of 82.3%, 50%, and 75%, respectively. Most commonly identified disease sites were nodal metastases (82.9%), followed by thyroid bed lesions (10.5%). 82.1% of patients positive on 68Ga-DOTA-RGD2 PET/CT showed lesional radiotracer uptake higher than the liver (grade IV and grade V).
Conclusions:
68Ga-DOTA-RGD2 PET/CT showed a similar sensitivity to, but higher specificity and overall accuracy than 18F-FDG PET/CT in detection of lesions in RAIR-DTC patients. This novel application of the angiogenesis imaging modality can prove useful in RAIR-DTC, especially in patients with negative/suspicious 18F-FDG PET/CT. Furthermore, since the majority of patients (82.1%) positive on 68Ga-DOTA-RGD2 PET/CT showed radiotracer avidity toward the higher end of the spectrum (grade IV and grade V), novel 177Lu-based theranostics can be a potential treatment for these patients.
Introduction
Radioiodine-refractory differentiated thyroid cancer (RAIR-DTC) includes biochemical evidence of disease with—negative diagnostic 123I or low-dose 131I whole-body scan; negative post-therapy 131I whole-body scan; 131I uptake only in some, but not all tumor, foci or disease progression despite tumor uptake of 131I (1). The two primary challenges associated with RAIR-DTC are as follows: (i) detection of structural disease in patients with evidence of biochemical disease and (ii) treatment of the disease using therapeutic modalities, other than 131I. The workup toward the former includes biochemical confirmation of the presence of disease in the form of stimulated serum thyroglobulin (sTg) levels ≥10 ng/mL, or suppressed sTg ≥1 ng/mL with negative serum anti-thyroglobulin antibodies (sATg), or serial rising sATg levels, as per the American Thyroid Association (ATA) guidelines (2).
Imaging modalities such as ultrasound (US), high-resolution computed tomography (HRCT) of the chest, magnetic resonance imaging, and positron emission tomography (PET) were utilized for the detection of structural disease. Metastatic involvement is most commonly observed in the neck lymph nodes with distant involvement occurring in the lungs and bone. Failure of conventional imaging to identify disease prompts the use of 18F-FDG PET/computed tomography (CT) as next step in the diagnostic algorithm. The sensitivity of 18F-FDG PET/CT in the detection of structural disease in RAIR-DTC has been reported in the range of 11–100% (3 –9). There is a subgroup of patients who have a negative 18F-FDG PET/CT as well, which further complicates the management plan.
The next challenge is choosing an appropriate treatment for RAIR-DTC, especially in patients with surgically unresectable disease. The currently available options are limited, lack standardization with very insignificant clinical benefits, or are fraught with significant adverse effects leading to poor compliance (10). The treatment options include external beam radiation therapy, chemotherapeutic drugs such as cisplatin, doxorubicin, and taxanes, re-differentiation agents such as retinoic acid, histone deacetylase inhibitors, and tyrosine kinase inhibitors (TKI) such as lenvatinib and sorafenib (10 –15).
The tripeptide sequence of arginine–glycine–aspartate (RGD) is the integrin binding domain, which is part of several extracellular matrix (ECM) proteins. Integrins are heterodimer, transmembrane glycoprotein cell adhesion molecules that are involved in cell–cell and cell–ECM interaction (16). The RGD tripeptide sequence has high affinity and specificity toward the integrin αvβ3, which is overexpressed on the tumor vasculature and is thus an excellent angiogenesis biomarker (17). As the tumor vasculature and several tumor cells express αvβ3 integrin, the angiogenic markers such as RGD peptide are better suited for their detection. Since the mechanism of radiotracer localization is different in 18F-FDG PET/CT and 68Ga-DOTA-RGD2 PET/CT, the latter may have diagnostic utility in patients with thyroglobulin elevation with negative 131I scintigraphy (TENIS).
The benefit of 68Ga-DOTA-RGD2 PET/CT in patients with RAIR-DTC, similar to the management dilemma, can be twofold. Apart from the detection of structural disease, especially in patients who are negative on 18F-FDG PET/CT, the second potential benefit is that patients with lesions showing 68Ga-DOTA-RGD2 uptake are potential candidates for RGD-peptide-based therapeutic options. These options include, but are not limited to 177Lu-labeled RGD, various chemotherapeutic drugs such as paclitaxel and doxorubicin coupled with RGD peptide (18 –21).
Thus, in the absence of current literature evaluating the uptake pattern of 68Ga-DOTA-RGD2 in RAIR-DTC, this prospective study was performed to (i) compare the diagnostic accuracy of 68Ga-DOTA-RGD2 PET/CT with 18F-FDG PET/CT in patients with RAIR-DTC and (ii) assess the tumor radiotracer avidity to assess eligibility toward RGD-peptide-targeted therapies.
Materials and Methods
This prospective study included 44 consecutive patients with RAIR-DTC being managed in the Nuclear Medicine outpatient department of the institute between July 2016 and August 2018, considering the following inclusion and exclusion criteria. The study was duly approved by the Institutional Ethics Committee (INT/IEC/2017/873). Written informed consent was obtained from all the patients before their enrolment in the study.
Inclusion criteria
Patients with histopathologic diagnosis of DTC (papillary and follicular thyroid carcinoma) on post-surgery and after 131I therapy follow-up.
Thyrotropin (TSH)-stimulated sTg >10 ng/mL with negative sATg (<15 IU/mL).
Detectable sATg (>15 IU/mL) with serial rising levels.
Negative 131I post-therapy whole-body scintigraphy.
Exclusion criteria
Patients diagnosed with medullary or anaplastic thyroid carcinoma.
Pregnant/lactating women.
The demographic parameters of all the study participants including surgical summary and histopathology reports were recorded. The tumor–node–metastasis disease staging as per the American Joint Committee on Cancer (TNM-AJCC) and initial risk stratification was performed as per the ATA guidelines (2,22). sTg, sATg, and sTSH (TSH stimulation) values were recorded at the time of the study and at follow-up (six monthly interval). All the values were estimated by the standardized quantitative electrochemiluminescence immunoassay (ECLIA) method. All sTg and sATg values were obtained under TSH stimulation (sTSH >30 μIU/mL) by the thyroid hormone withdrawal method.
All study participants having prior negative 131I post-therapy whole-body imaging with elevated sTg or serial rising sATg underwent 18F-FDG PET/CT as a part of the routine diagnostic workup, using 18F-FDG as an intravenous bolus injection, at an activity of 5 MBq/kg body weight.
PET/CT acquisition was performed from vertex to mid-thigh at 50–70 minutes after injection of 18F-FDG, using dedicated full-ring PET/CT scanner with noncontrast CT (130 keV, 90 mA mean, section width 3 mm).
68Ga-DOTA-RGD2 PET/CT was performed within 2 weeks of 18F-FDG PET/CT. One microgram of the RGD2 peptide was used per 37 MBq of the 68Ga eluate (2–5 μg per patient dose) for synthesis of the radiopharmaceutical. 68Ga-DOTA-RGD2 was injected as an intravenous bolus injection at a dose of 2 MBq/kg body weight (maximum 200 MBq). PET/CT acquisition was performed from vertex to mid-thigh at 45–60 minutes after injection of 68Ga-DOTA-RGD2, using dedicated full-ring PET/CT scanner with noncontrast CT (120 keV, 40 mA mean).
Both PET/CT studies were performed under TSH-stimulated state using thyroid hormone withdrawal.
Image analysis and interpretation
Data obtained from the 18F-FDG PET/CT and 68Ga-DOTA-RGD2 PET/CT studies were reconstructed using an iterative reconstruction OSEM (Ordered Subset Expectation Maximization) algorithm along with attenuation correction.
All the PET/CT studies were independently reviewed by two certified nuclear medicine physicians who were blinded to the clinical and other diagnostic parameters of the study participants.
The uptake of 18F-FDG and 68Ga-DOTA-RGD2 was also assessed by drawing a circular region of interest over the entire lesion/lesions and was expressed as the maximum standardized uptake value (SUVFDG and SUVRGD). The assessment of both set of images included characterization of the primary lesion, number of locoregional and distant lesions, tracer avidity of the lesions, as well as semi-quantitative SUV measurement for the intensity of tracer uptake. SUV calculation was also performed for the mediastinal blood-pool tracer activity (at the arch of aorta; regarded as background tracer activity), liver, and splenic tracer uptake. Abnormal nonphysiological uptake of the radiotracer, higher than the mediastinal blood pool, consistent with the disease process was taken as a positive finding in both the PET/CT studies.
Disease foci were divided into the following regions: thyroid bed (remnant/recurrent), nodal disease (cervical, mediastinal), and lung and skeletal lesions. The number of lesions at each site was also noted, except in the lung where more than five lesions were labeled as multiple. Lung nodules were not included in the total lesion count on both PET/CT studies.
In the absence of any previous system for grading radiotracer uptake on 68Ga-DOTA-RGD2 PET/CT, we devised a 5-point visual grading system to provide an estimate for the degree of radiotracer avidity, inspired from the Krenning score (23).
Grade I—Uptake just higher than the background tracer activity.
Grade II—Uptake higher than the background but less than the liver tracer activity.
Grade III—Uptake similar to the liver tracer activity.
Grade IV—Uptake higher than the liver activity but less than the splenic activity.
Grade V—Uptake higher than the splenic activity.
Patients were assigned a grade based on the lesion with the maximum radiotracer avidity. All the four sites (thyroid bed, nodal, lungs, and skeletal) were also assigned grades based on the representative lesion with maximum avidity at each site.
Surgical resectability of the lesions detected on PET/CT was also assessed during the follow-up by surgical specialists to provide the standard of care treatment wherever feasible.
Reference standard
Study candidates were followed-up with histopathologic analysis of the suspicious lesions wherever feasible, clinical examination, conventional imaging such as US, HRCT chest, and sTg and sATg values. Since histopathologic analysis could not be performed in all the patients, due to inaccessible lesions, patient's unwillingness to undergo histopathologic sampling, or other technical reasons, we formulated a reference standard against which both the PET/CT findings were compared.
The following points were considered in the criteria for positive disease: Histopathology of the suspicious lesion on PET/CT positive for metastatic DTC. Serial rise in TSH-stimulated sTg values without any intervention. Stable TSH-stimulated sTg with absolute value >10 ng/mL. Rise in TSH-stimulated sTg values in response to therapy with re-differentiation agents. Fall in TSH-stimulated sTg values in response to therapy with TKI, local radiation therapy. Serial rising sATg levels on follow-up (>15 U/mL). Clinical examination, conventional imaging (US, HRCT chest) suggestive of the presence of disease.
The following points were considered in the criteria for negative disease:
Spontaneous fall in TSH-stimulated sTg values without any treatment, with an absolute value <10 ng/mL at follow-up.
Spontaneously declining sATg values on follow-up.
Clinical examination, conventional imaging (US, HRCT chest) negative for the presence of disease.
Based on the reference standard, both the PET/CT findings were categorized as true positive (TP), true negative (TN), false positive (FP), and false negative (FN).
Statistical analysis
Statistical analysis was carried out using Prism version 8 (GraphPad Software, Inc., San Diego, CA). Continuous variables were described in terms of mean and standard deviation or in terms of median and range in case of outliers. Categorical variables were expressed in terms of numbers and percentages. Diagnostic performance of both the PET/CT studies was described in terms of sensitivity, specificity, positive predictive value, negative predictive value, and accuracy. Comparison of diagnostic accuracy of both modalities was performed using the McNemar test. Correlation between paired continuous variables was determined using Pearson's r test (Gaussian distribution) or Spearman's rho (non-Gaussian distribution). Inter-rater reliability between the two PET/CT studies was assessed using Cohen's kappa (κ) statistics. p-Value <0.05 was considered statistically significant.
Results
Patient characteristics
A total of 44 consecutive patients, as per the eligibility criteria, were included in the study, 32 with elevated stimulated sTg and negative sATg and 12 with serial rising sATg. All the patients had a negative 131I post-therapy whole-body scans. Summary of the patient characteristics, including age, sex, disease, treatment details, and biochemical parameters are presented in Table 1. Flow of the participants in this study is shown in Figure 1. None of the patients experienced any adverse effects related to the diagnostic tests during the study.
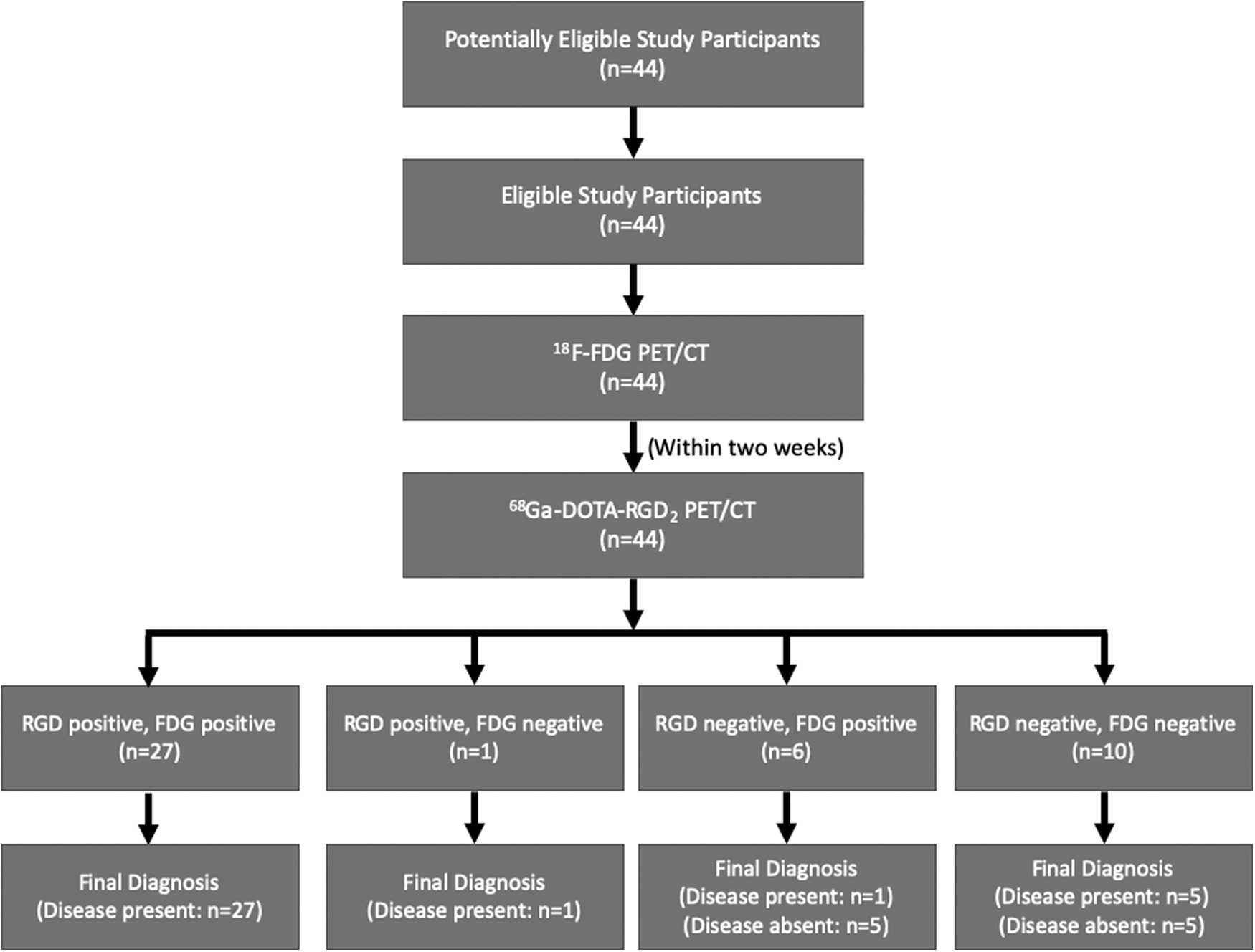
Flow of the participants during the study.
Demographic and Clinical Characteristics
Index values—at the time of imaging.
AJCC, American Joint Committee on Cancer; ATA, American Thyroid Association; FTC, follicular thyroid cancer; MND, modified neck dissection; PTC, papillary thyroid cancer; sATg, serum anti-thyroglobulin antibodies; SD, standard deviation; sTg, serum thyroglobulin; sTSH, TSH stimulation; TENIS, thyroglobulin elevation with negative 131I scintigraphy; TT, total thyroidectomy.
Reference standard
All the 44 patients were followed-up for a mean duration of 16.8 ± 3.8 months (range: 10–22 months). As per the reference standard, 34/44 (77.3%) patients were regarded as positive for disease. Histopathology of the suspicious lesions on PET/CT was available in 18/44 (40.9%) patients and was positive for metastatic thyroid carcinoma in 17/18 patients. Of the 32 patients with elevated sTg, four showed rising sTg values on follow-up, seven had stable sTg, one had rising sTg in response to thalidomide, and one had declining sTg in response to sorafenib treatment. Of the other 12 patients with elevated sATg, four had serial rising sATg on follow-up. Neck US showed evidence of structural disease in 6/44 (13.6%) patients with elevated sTg or rising sATg that was subsequently confirmed on histopathology.
Ten of the 44 (22.7%) patients were regarded as negative for disease. In the elevated sTg group, all five patients had a spontaneously declining sTg with the absolute value at follow-up <10 ng/mL. Neck US was negative in all the five candidates, and they were asymptomatic at last follow-up. In the elevated sATg group, 5/12 patients had serial declining sATg on follow-up with negative neck US, while one patient had additional confirmation with a negative histopathology from cervical lymph node biopsy.
Lesion-based analysis
Apart from physiological radiotracer distribution in the choroid plexus, liver, spleen, small intestine, kidneys, and urinary bladder, 68Ga-DOTA-RGD2 PET/CT detected a total of 123 lesions in 28 patients, excluding lung nodules which were not counted. Thirteen of the 123 lesions were thyroid bed lesions (10.6%), 102/123 (82.9%) were nodal lesions, including cervical and mediastinal lymph nodes, and 8/123 (6.5%) were skeletal lesions. Mean SUVmax values of the mediastinal blood pool, liver, and spleen were 1.1 ± 0.4, 2.5 ± 0.9, and 7.0 ± 2.5, respectively. SUVRGD had a strong positive correlation with sTg values (r = 0.74) which was highly statistically significant (p < 0.0001).
18F-FDG PET/CT detected a total of 144 lesions in 33 patients, excluding lung nodules which were not counted. Twelve of the 144 (8.3%) lesions were thyroid bed lesions, 124/144 (86.1%) were nodal lesions, and remaining 8/144 (5.5%) were skeletal lesions. The mean mediastinal blood pool SUVmax was 2.1 ± 0.7. SUVFDG had a moderate positive correlation with sTg values (r = 0.68), which was highly statistically significant (p < 0.0001).
Lesion sites, radiotracer avidity, and concordance between the two modalities are represented in Table 2. Lesion detection at the thyroid bed by 68Ga-DOTA-RGD2 PET/CT and 18F-FDG PET/CT showed strong inter-rater agreement (κ = 0.93) while that at the nodal region showed fair agreement (κ = 0.31).
Sites of Lesion Detection, Radiotracer Avidity, and Concordance/Discordance on 68Ga-DOTA-RGD2 Positron Emission Tomography/Computed Tomography and 18F-FDG PET/CT
SUVRGD and SUVFDG are expressed in mean ± SD (range).
CT, computed tomography; PET, positron emission tomography; RGD, arginine–glycine–aspartate.
Overall diagnostic performance
68Ga-DOTA-RGD2 PET/CT was positive for disease in 28/44 (63.6%) patients and negative in 16/44 (36.4%) patients. All the 28 patients were TP, 10/16 were TN, and 6/16 were FN. There were no FP on 68Ga-DOTA-RGD2 PET/CT. The overall sensitivity and specificity of 68Ga-DOTA-RGD2 PET/CT was 82.3% and 100%, respectively. 18F-FDG PET/CT was positive for disease in 33/44 (75%) patients and negative in 11/44 (25%) patients. Twenty-eight of the 33 patients were TP, 5/33 were FP, 5/11 were TN, and 6/11 were FN. The overall sensitivity and specificity of 18F-FDG PET/CT was 82.3% and 50%, respectively. A comparison of diagnostic performance of the two imaging modalities is presented in Table 3. Overall diagnostic performance of 68Ga-DOTA-RGD2 PET/CT and 18F-FDG PET/CT showed substantial agreement (κ = 0.63) with no statistically significant difference on the McNemar test (two-tailed p = 0.62).
Overall Diagnostic Performance of 68Ga-DOTA-RGD2 PET/CT and 18F-FDG PET/CT
CI, confidence interval.
Elevated sTg group
68Ga-DOTA-RGD2 PET/CT was positive for disease in 23/32 (23/23 TP) patients and negative in 9/32 (5/9 TN, 4/9 FN) patients. 18F-FDG PET/CT was positive for disease in 25/32 (23/25 TP, 2/25 FP) patients and negative in 7/32 (3/7 TN, 4/7 FN) patients.
The diagnostic performance of both PET/CT studies at various sTg levels is presented in Table 4.
Diagnostic Performance of 68Ga-DOTA-RGD2 PET/CT and 18F-FDG PET/CT in Patients with Elevated Serum Thyroglobulin and Negative Serum Anti-Thyroglobulin Antibodies, in Relation to Serum Thyroglobulin Values
sTg values (under TSH stimulation) are expressed in ng/mL. Since none of the patients with sTg >30 ng/mL were negative for disease as per the reference standard, the specificity values of both PET/CT modalities cannot be calculated at sTg >30 ng/mL.
Values in parentheses represent number of patients in each strata.
TSH, thyrotropin.
Rising sATg group
68Ga-DOTA-RGD2 PET/CT was positive for disease in 5/12 (5/5 TP) patients and negative in 7/12 (5/7 TN, 2/7 FN) patients. 18F-FDG PET/CT was positive for disease in 8/12 (5/8 TP, 3/8 FP) patients and negative in 4/12 (2/4 TN, 2/4 FN) patients.
68Ga-DOTA-RGD2 PET/CT—radiotracer uptake grading, distribution of lesions
68Ga-DOTA-RGD2 PET/CT showed the highest tumor to blood pool and tumor to liver (T/L) uptake ratio in the skeletal lesions, with a mean of 14.9 ± 9.1 (range: 6.3–24.4) and 5.2 ± 2.7 (range: 2.1–7.1), respectively. The detailed radiotracer avidity of lesions at various sites is presented in Table 5.
Radiotracer Uptake at Various Sites, Tumor to Blood-Pool and Tumor to Liver Standardized Uptake Value Ratios on 68Ga-DOTA-RGD2 PET/CT
SUVmax, T/B ratio, and T/L ratio are expressed in mean ± SD (range).
T/B ratio, tumor to blood-pool SUV ratio; T/L ratio, tumor to liver SUV ratio; SUV, standardized uptake value.
The radiotracer uptake on 68Ga-DOTA-RGD2 PET/CT was graded according to a 5-point visual scale as shown in Figure 2. Seventeen of 28 (60.7%) patients with a positive 68Ga-DOTA-RGD2 PET/CT were categorized in grade IV, showing lesional radiotracer uptake higher than that of the liver. Six of 28 (21.4%) patients were categorized as grade V, showing lesional radiotracer uptake higher than that of the spleen. Apart from a single thyroid bed site, grade I radiotracer uptake was not noted elsewhere among all the patients with a positive 68Ga-DOTA-RGD2 PET/CT. Detailed grading on a per patient basis and per site basis is presented in Table 6, and representative scans in Figure 2.
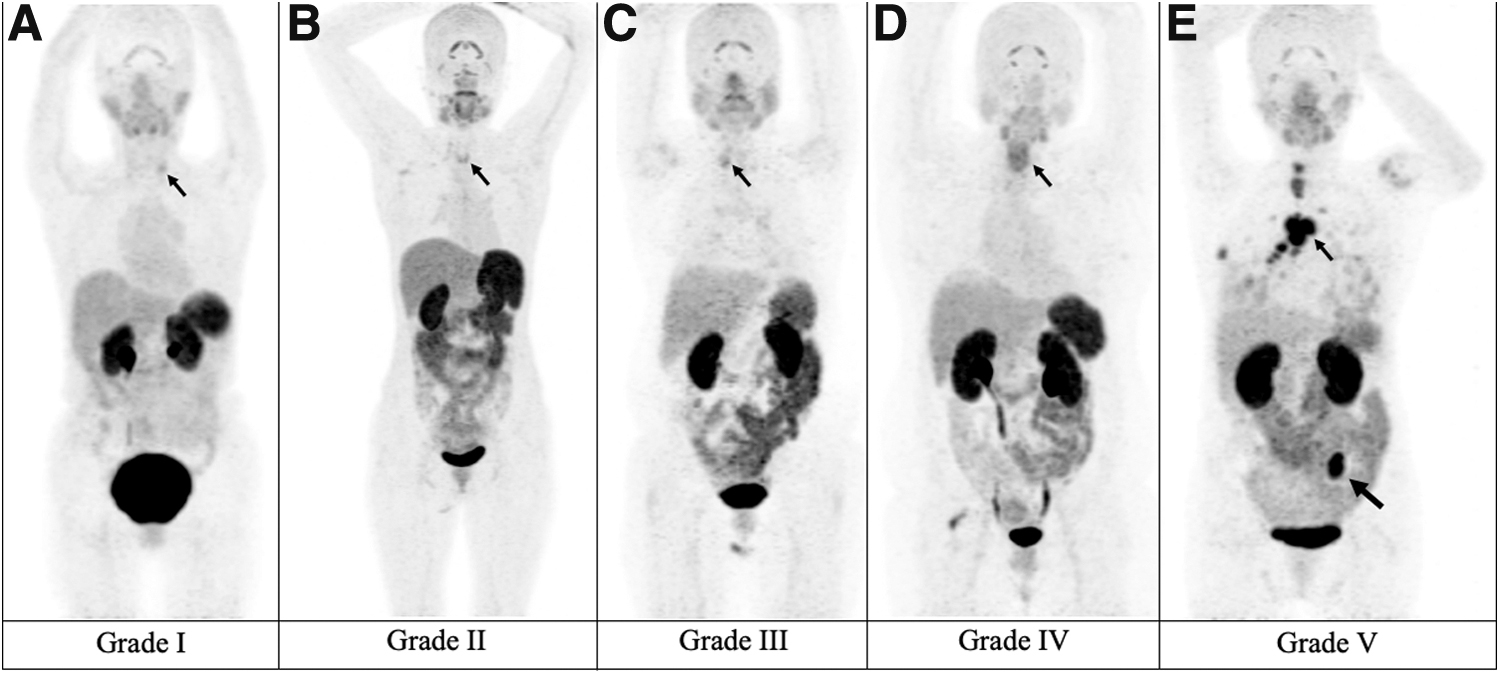
Representative maximum intensity projection images: 5-point visual grading system for radiotracer uptake on 68Ga-DOTA-RGD2 PET/CT (lesions are represented with arrows). (
Five-Point Visual Grading System for Radiotracer Uptake on 68Ga-DOTA-RGD2 PET/CT
Note that the second column on number of patients shows patient wise and not lesion wise grading.
Grade I: uptake just higher than the background tracer activity. Grade II: uptake higher than background but less than the liver tracer activity. Grade III: uptake similar to the liver tracer activity. Grade IV: uptake higher than the liver activity but less than the splenic activity. Grade V: uptake higher than the splenic activity.
Twenty-four of 28 (85.7%) patients with lesions detected on 68Ga-DOTA-RGD2 PET/CT had surgically unresectable disease at follow-up. Nineteen of the 24 (79.2%) patients had multiple foci of disease in the body, involving more than one of the four previously described sites.
Discussion
The exigent diagnosis of RAIR-DTC is a challenging situation, at both the diagnostic and therapeutic front. 18F-FDG PET/CT has proven its utility in the detection of structural disease in these patients with increasing sensitivity at higher levels of sTg (9,24). However, it has several limitations, including nonspecific accumulation of radiotracer in benign and nonneoplastic (infective/inflammatory) sites, necessitating histopathologic confirmation of a suspicious lesion, which may or may not be feasible (25). Our study also had a similar case which was false positive on 18F-FDG PET/CT but true negative on 68Ga-DOTA-RGD2 PET/CT (Fig. 3). Another limitation is the relatively low glucose metabolism by indolent slow-growing tumors, which are likely to be missed on PET/CT (26).
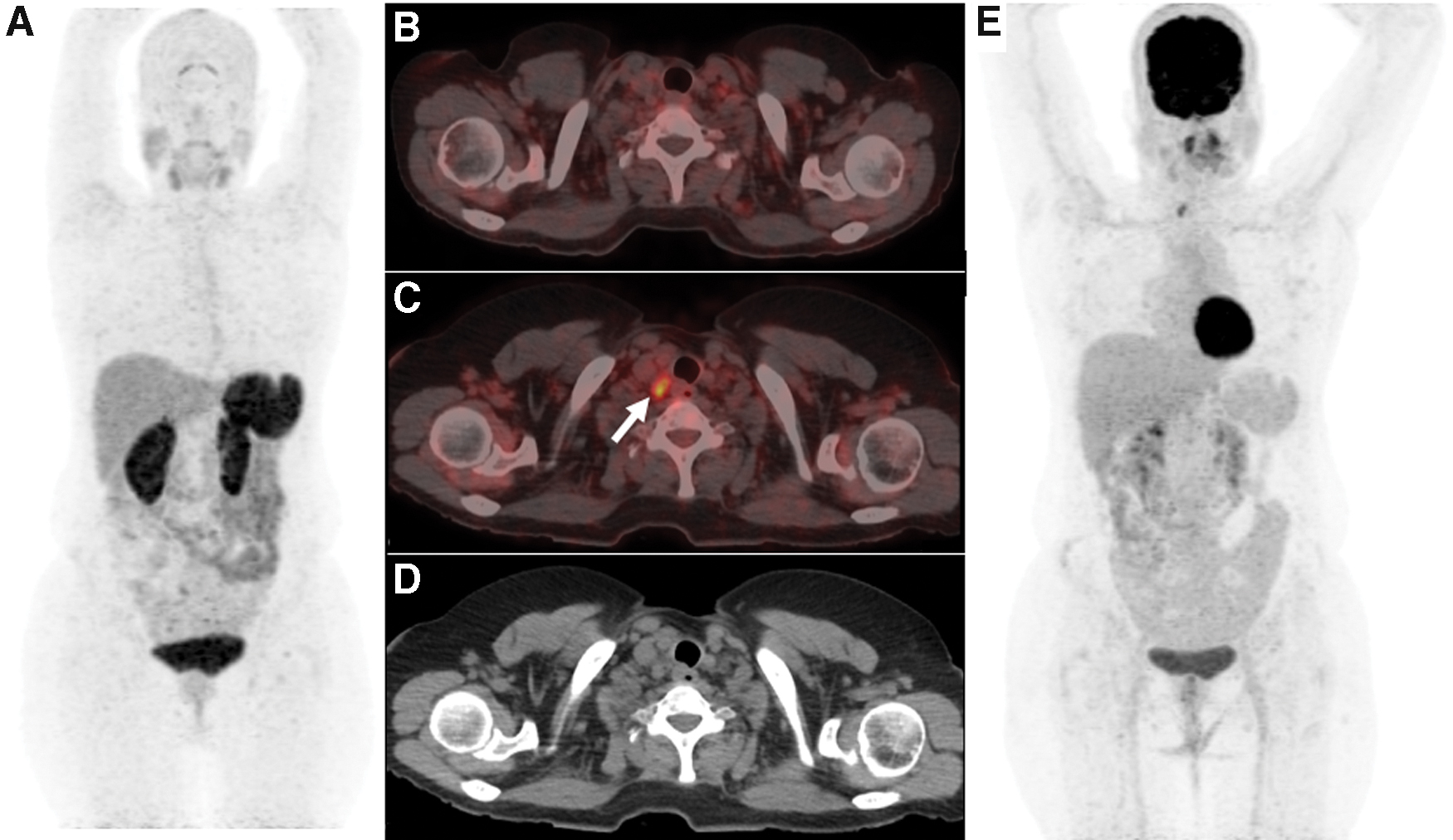
15/F with PTC, post-surgery and RAI therapy—with sTg 15 ng/mL and negative 131I post-therapy whole-body scan. 68Ga-DOTA-RGD2 PET/CT maximum intensity projection image (
One patient who was false negative on 18F-FDG PET/CT in the present study had a histopathologically proven local disease recurrence at the level VI cervical lymph nodes. The lymph nodes were, however, detected on 68Ga-DOTA-RGD2 PET/CT (Fig. 4). Since neoangiogenesis is a prerequisite for tumor growth, this could perhaps be explained by the phase of neoangiogenesis and a relatively lower rate of glucose metabolism in the tumor cells.
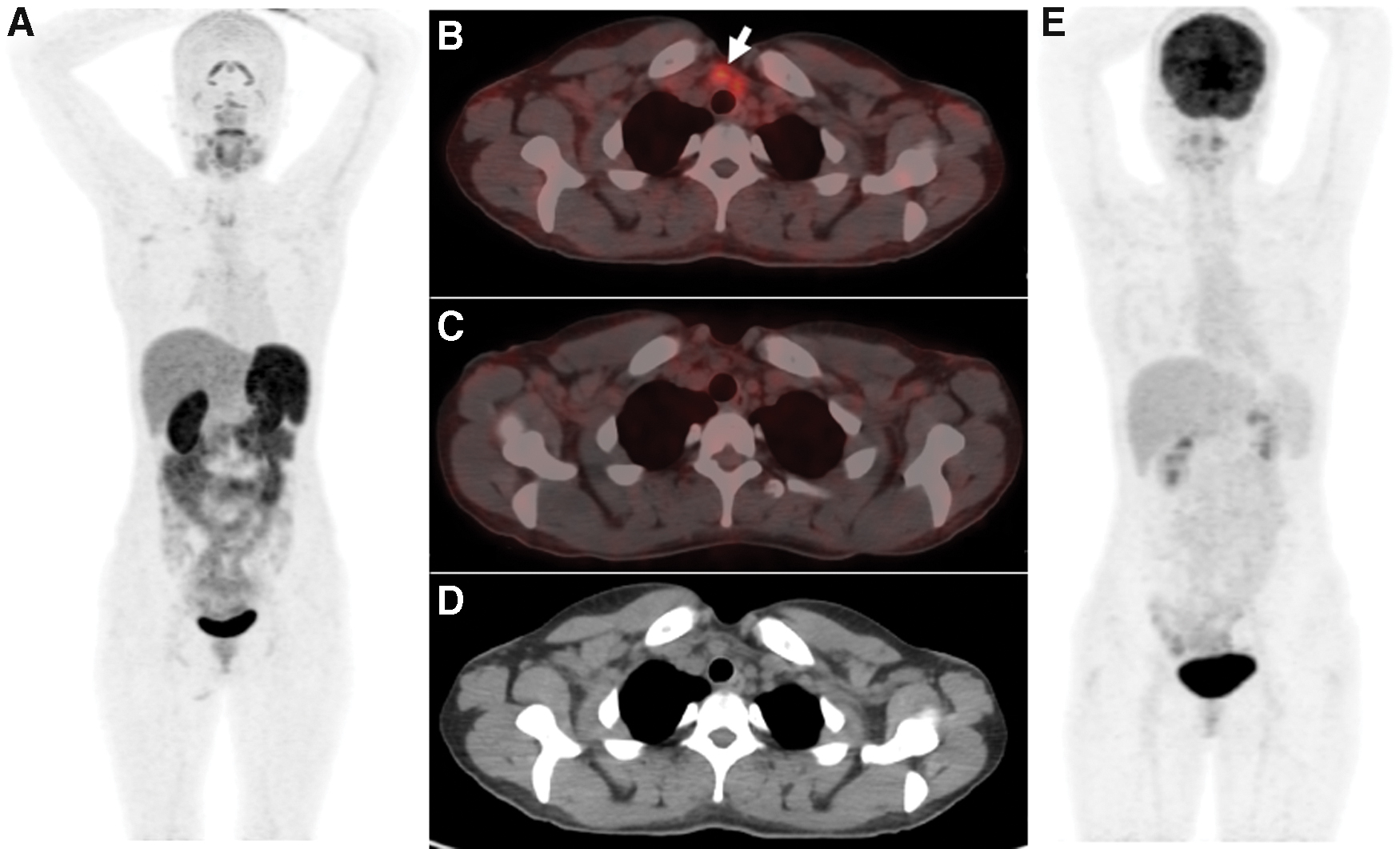
21/F with PTC, post-surgery and RAI therapy—with sTg 85 ng/mL and negative 131I post-therapy whole-body scan. 68Ga-DOTA-RGD2 PET/CT maximum intensity projection image (
68Ga-DOTA-RGD2 PET/CT is a neoangiogenesis imaging modality, which has high affinity and specificity toward αvβ3 integrin (17). Neoangiogenesis is an essential step in tumor growth and metastasis, and in its absence, tumors cannot grow beyond the size of 1–2 mm (27).
In this study, both 18F-FDG PET/CT and 68Ga-DOTA-RGD2 PET/CT showed a similar sensitivity of 82.3%; however, 68Ga-DOTA-RGD2 PET/CT had a higher specificity of 100% compared with 50% on 18F-FDG PET/CT. Five patients were FN on both PET/CT studies, of which one patient responded to treatment with TKI showing a fall in sTg. A reduction in sTg is preceded by actual tumor shrinkage as documented on conventional imaging and thus could be a reflection of changes in the tumor signaling (28,29). Thus, tumors below the detection threshold of PET/CT resolution would still be affected by TKI therapy, with a corresponding decrease in sTg levels. The remaining four patients were kept on levothyroxine suppression and close follow-up to see the trend of sTg/sATg.
The diagnostic performance of 18F-FDG PET/CT in the present study conforms to that reported in the literature, with increasing sensitivity at higher sTg values (3,5,7,30). While the role of 68Ga-DOTA-RGD2 PET/CT has not been explored in the setting of RAIR-DTC previously, Gao et al. (31) performed 99mTc-3PRGD2 single photon emission computed tomography (SPECT)/CT in 37 patients with TENIS and reported a sensitivity and specificity of 96.6% and 75%, respectively. They noted improvement in sensitivity to 100% at sTg >30 ng/mL.
However, the study has some limitations, the first being lack of histopathology as the reference standard in 72% of patients. Second, the study population constituted of candidates who had not received empirical 131I before the SPECT/CT. The utility of empirical 131I therapy has already been reported in 62% of patients having an initial negative diagnostic whole-body scan, subsequently having a positive post-therapy whole-body scans after empirical therapeutic dose of 131I (32). Thus, these patients, constituting more than 50% of the rising thyroglobulin and negative diagnostic whole-body scan population, are actually having iodine-avid and iodine-responsive disease.
Next, the standard for qualifying patients as negative for disease included spontaneously falling sTg values without considering the absolute value. Seven of 37 patients with negative SPECT/CT were classified as TN based on falling sTg values, even when not all patients had sTg <10 ng/mL. The study does not compare results of SPECT/CT with 18F-FDG PET/CT, which is the standard of care in the diagnostic workup of patients with TENIS.
In the present study, both the PET/CT modalities had increasing sensitivity with higher sTg values, with 100% sensitivity at sTg >100 ng/mL (Table 4). Since none of the patients with sTg >30 ng/mL was negative for disease as per the reference standard, the specificity values of both PET/CT modalities could not be calculated at sTg >30 ng/mL. Similar findings with 18F-FDG PET/CT have been reported in the literature (7,9).
18F-FDG positive and 131I negative disease represents a point in the dedifferentiation continuum where the tumor has lost sodium iodide symporter expression or membrane insertion but continues to produce thyroglobulin. sTg is a sensitive tumor marker after ruling out other causes and has shown to be rarely negative (3–4%) in the setting of disease recurrence (33). Given this fact, at lower levels of sTg, the tumor volume may be insufficient to be detected on PET/CT. As the tumor volume increases, sTg correspondingly increases, thus accounting for superior diagnostic performance of PET/CT at higher sTg values.
In the present study, the SUVmax of the lesions on 68Ga-DOTA-RGD2 PET/CT had a strong positive correlation (r = 0.74) with sTg, which was highly statistically significant (p < 0.0001). This is in contrast to the findings by Gao et al. who reported no linear correlation between sTg and tumor to background (T/B) SUV ratios (31). It has been shown that the tumor size and growth rates have a positive correlation with neoangiogenesis, and thus, the uptake of angiogenesis targeting radiotracers (34). Since sTg also has a positive correlation with increasing disease burden, it is comprehensible that sTg and SUVmax on 68Ga-DOTA-RGD2 PET/CT have a positive correlation. The increasing avidity of the lesions suggests higher growth and metastatic potential.
Overall, 18F-FDG PET/CT detected higher number of lesions (144) compared with 68Ga-DOTA-RGD2 PET/CT (123). Lesion detection rate by both the modalities showed excellent agreement at the thyroid bed (κ = 0.93), and fair agreement at the nodal sites (κ = 0.31). Both modalities performed equally in detection of lung and skeletal lesions. 18F-FDG PET/CT had higher mean SUVmax values for all the four disease sites compared with 68Ga-DOTA-RGD2 PET/CT (Table 2). However, since the two radiotracers have different kinetics and mechanisms of localization, a direct comparison of their uptake values would not be prudent.
68Ga-DOTA-RGD2 PET/CT was positive in 28/44 patients, of which 24 (85.7%) had surgically unresectable disease at follow-up. Additionally, 19/24 (79.2%) patients had multiple tumor foci, indicating disseminated disease and thus requiring systemic therapy. Biodistribution studies using 177Lu-DOTA-RGD2 in mice with melanoma showed 80% injected activity per gram of tissue (IA/g) being excreted at 30 minutes after tracer administration and 96% IA/g clearance at 72 hours. Among the normal organs, highest activity was observed in the kidneys (6.4% IA/g), followed by the lungs (5.6%) and liver (4.8%) at 30 minutes post-injection. The highest tumor:blood ratio was seen at 24 hours (58.4% IA/g) and decreased by 72 hours (33.6% IA/g). Highest tracer activity in the whole body at 72 hours was noted at the tumor site (1.5% IA/g) (35).
This suggests favorable kinetics with early clearance of the radiotracer from the blood pool, thus potentially minimizing marrow radiation burden. As an initial step toward proof-of-concept, our group performed the first in-human theranostics using RGD peptide and showed good response after a single cycle of 177Lu-DOTA-RGD2 in a patient of RAIR-DTC with disseminated disease and showing high uptake of 68Ga-DOTA-RGD2 (21). In the present study, the T/B and T/L ratios calculated for the four disease sites showed significant tumor to background uptake, as well as high lesional radiotracer activity compared with the hepatic uptake (Table 5). The median T/L ratio of 1.7 (0.5–7.1) suggests adequate lesional uptake of radiotracer compared with the hepatic activity. Since there are no previous data on 68Ga-DOTA-RGD2 PET/CT in TENIS, we devised a novel visual 5-point scale for categorizing radiotracer uptake, similar to the Krenning score used in somatostatin receptor scintigraphy (23). According to our 5-point visual scale, 23/28 (82.1%) patients positive on 68Ga-DOTA-RGD2 PET/CT had a radiotracer uptake higher than that of the liver (grade IV and grade V). Representative grade V radiotracer uptake is shown in Figure 5. Jois et al. evaluated the role of somatostatin receptor scintigraphy in TENIS for the purpose of estimating candidates eligible for peptide receptor radionuclide therapy (PRRT). Of a total of 19 patients, only three (15.8%) had a radiotracer uptake equal to/more than in the liver, thus provisionally qualifying for PRRT. On a per lesion basis, 3/25 (12%) lesions had a radiotracer uptake equal to/more than the liver (36).

76/M with insular variant of PTC, post-surgery and RAI therapy—with sTg 1024 ng/mL and negative 131I post-therapy whole-body scan. 68Ga-DOTA-RGD2 PET/CT maximum intensity projection image (
Because no guidelines currently exist for planning theranostics with RGD peptide, upon extrapolation from the PRRT guidelines, we propose that patients with grade IV or V scores as per our scoring can be eligible candidates for therapy with 177Lu-DOTA-RGD2 from an imaging point of view. This would include 82.1% patients in our study, a number significantly higher than the eligible candidates for PRRT, which also included uptake equal to the liver in the qualifying criteria. Since 19/23 (82.6%) patients with lesions detected on 68Ga-DOTA-RGD2 PET/CT had surgically unresectable disease at follow-up, they could be subjected to further workup for assessment of eligibility toward 177Lu-DOTA-RGD2 therapy.
Footnotes
Author Disclosure Statement
All the contributing authors declare that they have no competing financial interests.
Funding Information
No funding was received for this work.