
Abstract
Nonautoimmune hyperthyroidism caused by activating mutations in the GNAS gene is a rare condition. In this study, we report a five-year-old girl diagnosed with nonautoimmune hyperthyroidism and tall stature harboring a somatic mosaic gain-of-function mutation in the GNAS gene (NM_080425.3:
Introduction
Toxic multinodular goiter is a frequent cause of nonautoimmune hyperthyroidism. Although somatic mutations in the TSH receptor (TSHR) have been described as a common explanation for this disorder, GNAS defects can cause this phenotype as part of the complex McCune–Albright syndrome, and extremely rarely as isolated toxic thyroid adenomas due to activating GNAS mutations (1,2). In this study, we report a girl with nonautoimmune hyperthyroidism caused by a somatic mutation in the GNAS gene.
Case Report
A 4-year and 11-month-old girl of white European ancestry was found to be hyperthyroid when first evaluated for goiter and tall stature; height was +2.9 standard deviation score (SDS) and bone age 6 years and 10 months (+2.1 SDS). Her serum TSH was suppressed at <0.005 mU/L (0.4–3.6) and free thyroxine (fT4) was high at 4.52 ng/dL (0.85–1.75). Additional tests showed an elevation of her total T4 (TT4) of 17.4 μg/dL (5–11.6), TT3 of 513 ng/dL (90–180), and fT3 of 18.9 pg/mL (2–6). A thyroid autoimmunity screen (TSI, TRAb, TPO, and TG antibodies) was negative. Thyroid ultrasound showed a normal right upper lobe (RUL), while the right lower lobe and entire left lobe were heterogeneous with increased vascular flow (Supplementary Fig. S1). A 123I uptake scan showed an increased uptake at 57% (reference range 8–40). There were no café-au-lait spots and no history of fractures or bone lesions. Treatment with methimazole (MMI) in doses ranging from 7.5 to 10 mg daily kept her thyroid function tests within the reference range, and by 9 years her height was in the 90th percentile and has remained between the 75th and 90th percentile until her current age of 10.5 years. At this time she is premenarchal (Tanner pubic hair 4 and breast development 3).
Further Investigations and Results from Genetic Analysis
Written informed consents were obtained from all family members before blood and tissue collection according to a protocol approved by the IRB. Her nonconsanguineous parents and sister had no manifestations of hyperthyroidism, and no abnormalities in their thyroid glands or tests (Fig. 1A). Sequencing of genomic DNA obtained from circulating leukocytes and cDNA generated from thyroid tissue obtained by fine needle aspiration revealed no TSHR variants.
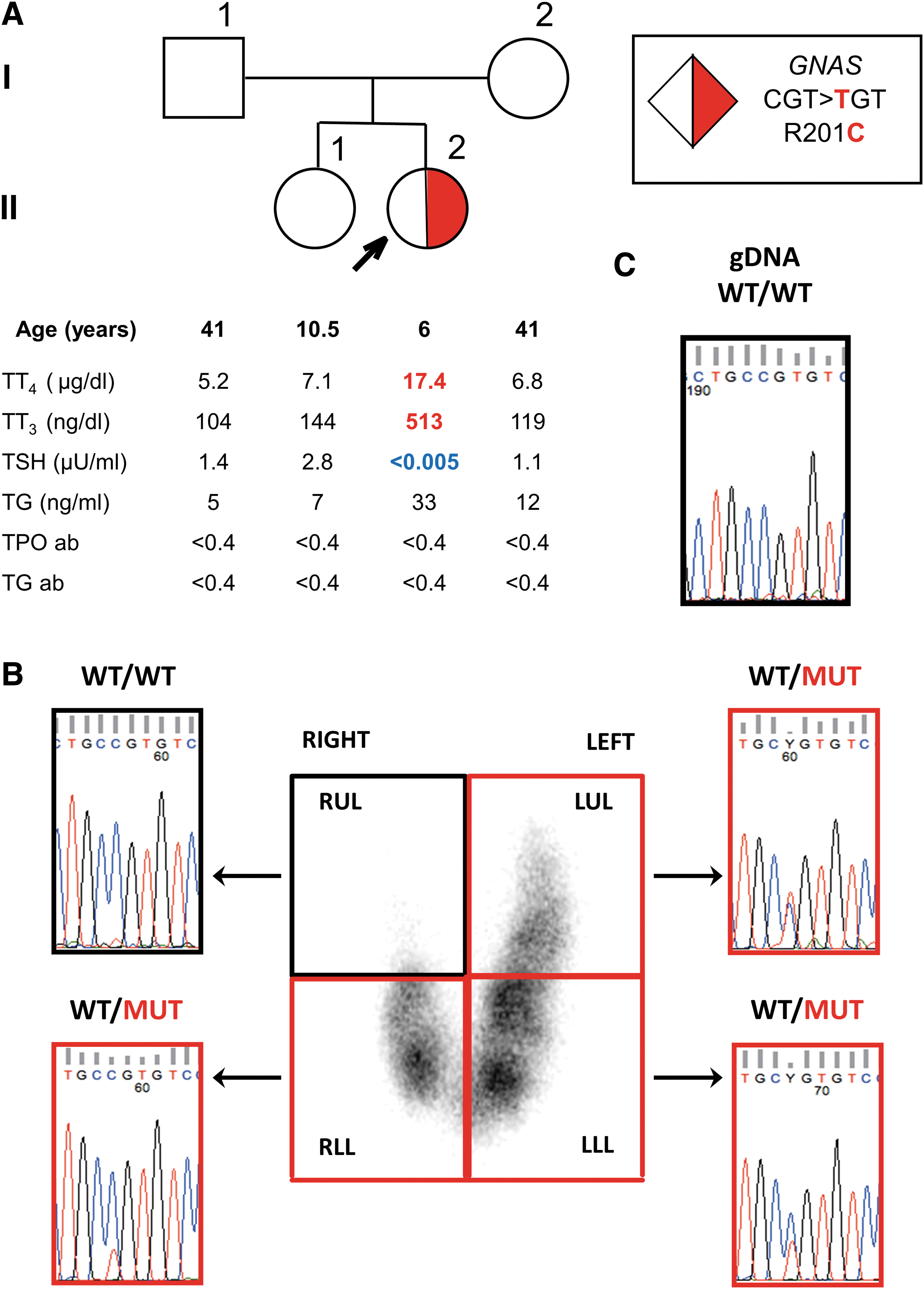
Pedigree of the family with thyroid tests results and genetic analysis.
MMI was discontinued for two weeks, which resulted in suppression of the serum TSH. A radioiodide scan was obtained, which showed no uptake in the RUL (Fig. 1B) where normal thyroid tissue was visualized by ultrasound (Supplementary Fig. S1). Total RNA was extracted from samples obtained by needle aspiration from each of the four quadrants of the thyroid gland and placed in Trizol® reagent (Life Technologies). cDNA was generated using VILO® reverse transcriptase (Life Technologies) following the manufacturer's instructions. Sanger sequencing revealedS a heterozygous missense mutation in the GNAS gene (ENST00000371100.4/NM_080425.3:
Given this finding, additional tests were obtained. Serum calcium, phosphorus, PTH, IGF1, IGF-BP3, cortisol, estrone, estradiol, FSH, and LH were all normal for sex and age.
Discussion
Gain-of-function mutations in genes of the cAMP-signaling pathway have been associated with autonomous hyperfunction of thyroid cells of mice and humans (1). The majority of activating mutations in patients with nonautoimmune hyperthyroidism involve TSHR defects, although GNAS mutations have been found in a small number of cases (2,3). In a study of 77 patients with hyperfunctioning toxic adenomas, only 5% were caused by somatic GNAS mutations (2). However, to our knowledge there is no report of a somatic GNAS mutation involving both lobes of the thyroid, yet sparing one portion. Activating GNAS mutations R201C and R201H have been reported in different endocrine tumors, involving the pituitary, testis, ovary, and thyroid adenomas and carcinomas (1). In vitro studies of R201C and R201H GNAS mutations have shown inhibition of GTPase activity leading to constitutive activation of adenylyl cyclase (4).
In conclusion, we report a case of nonautoimmune hyperthyroidism caused by a somatic mosaic GNAS mutation affecting part of the thyroid gland. Establishing that the mutation is present in only three of four quadrants of the thyroid gland allows for potentially selective surgical or radioiodide treatment, sparing the normal right upper thyroid lobe, and possibly maintaining euthyroidism without the need for lifelong thyroid hormone replacement.
Footnotes
Acknowledgments
The authors thank the patient and her family for participating in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants DK 15070 to S.R. and DK110322 to A.D. from the National Institutes of Health, USA.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2