
Abstract
Background:
Lenvatinib, an oral multikinase inhibitor, is the latest addition to the treatment options for radioactive iodine (RAI)-refractory progressive differentiated thyroid carcinoma (DTC). This study investigated the efficacy of lenvatinib in real-world practice and prognostic biomarkers of survival.
Methods:
This multicenter study included 43 patients receiving lenvatinib as first-line or second-line treatment after sorafenib for RAI-refractory DTC. Progression-free survival (PFS) was evaluated according to various clinical factors including thyroglobulin doubling time (TgDT), tumor volume DT (TVDT), and tumor growth slope (TGS; slope of tumor change rate).
Results:
Patients were treated with lenvatinib for a median of 14 months; 32 were previously treated with sorafenib. The median follow-up from lenvatinib initiation to the last censoring or death was 16 months. The median starting dose of 20 mg was reduced to a median sustainable dose of 10 mg in accordance with patient adverse events (AEs). The median PFS was 21.8 months; the median overall survival was not reached. The disease control rate was 97.7%, with the first objective response at 3.8 months. PFS was not significantly associated with previous sorafenib treatment, metastatic sites, or sustainable dose. TGS measured before (TGSpre, p = 0.003) and after (TGSpost, p = 0.036) the initiation of lenvatinib was associated with PFS. The sum of the largest diameters of target lesions (p = 0.043) and TgDT (p = 0.024) were associated with PFS, but TVDT calculated before (TVDTpre, p = 0.923) or after (TVDTpost, p = 0.966) lenvatinib treatment did not impact PFS. Lenvatinib was withdrawn in 24 patients (55.8%): in 6 patients because of treatment-induced AEs and in 18 patients because of disease progression or poor performance status. AEs of any grade were reported in all patients, and grade 3–4 AEs in 23.2% of the patients. The most frequent AE was fatigue or asthenia.
Conclusions:
Our results indicate that reduced doses of lenvatinib triggered by emergent AEs did not abrogate its apparent efficacy in patients with RAI-refractory DTCs. Rather, the sustained use of reduced doses of lenvatinib with a low rate of severe AEs may have contributed to the favorable outcomes. TgDT and TGS can assist in predicting the outcomes in these patients.
Introduction
Differentiated thyroid carcinoma (DTC) is well known for its excellent prognosis (1). Surgical resection and radioactive iodine (RAI) ablation followed by thyrotropin suppressive therapy lead to a 10-year survival of 95–98% (2,3). However, about 10% of DTC patients develop distant metastases and about two-thirds of these patients become refractory to RAI, which results in significant deterioration in survival (4,5). The effectiveness of conventional chemotherapy with doxorubicin or radiotherapy for control of the progression of RAI-refractory DTCs is limited (6,7). However, recently, sorafenib and lenvatinib, oral multikinase inhibitors affecting both tumor cell proliferation and angiogenesis (8,9), have revolutionized treatment for these patients with encouraging outcomes. Recent studies reported that sorafenib and lenvatinib prolonged progression-free survival (PFS) by 5 months (10) and 14.7 months (11) compared with placebo and had disease control rates of 54.1% and 87.7%, respectively. Clinical experience has confirmed the effectiveness of lenvatinib for RAI-refractory DTCs (12 –15), but the median PFS of 7.2–10.8 months (not reached in one study) was lower than the median 18.3 months reported in the SELECT trial (11). Previous reports of lenvatinib in clinical practice did not investigate the patient characteristics that predicted favorable treatment outcomes. This study conducted in seven tertiary medical centers in Korea assessed the effectiveness of lenvatinib in real-world practice and identified prognostic biomarkers of tumor growth of survival.
Methods
Patients
Patients at seven tertiary hospitals who were diagnosed with RAI-refractory progressive DTC and treated with lenvatinib for intractable locally advanced or metastatic disease between September 1, 2015, and April 30, 2019, were included. Diagnosis of RAI-refractory DTC required least one target lesion with lack of RAI uptake or progressive disease (PD) according to the Response Evaluation Criteria in Solid Tumors (RECIST) criteria (16) after any of the following: (1) cumulative RAI activity ≥600 mCi or (2) a single RAI treatment for RAI avid disease within the previous 14 months. Eligible patients were ≥18 years of age, with least one measurable lesion, and with an Eastern Cooperative Oncology Group performance status of 0–2. Patients who previously received TKI other than sorafenib or were candidates for surgery or radiotherapy were excluded. The study protocol was approved by the institutional review boards of each of the participating hospitals.
Effectiveness
The responses to lenvatinib treatment included complete response (CR), partial response (PR), stable disease (SD), and PD following the RECIST version 1.1 criteria (16). The disease control rate was reported as CR + PR + SD, and the clinical benefit rate was reported as CR + PR + SD for ≥23 weeks (11). PFS was the interval between lenvatinib initiation and the first documentation of PD. Overall survival (OS) was the interval between lenvatinib initiation and death from any cause.
Measurement of tumor growth rate
The association between thyroglobulin doubling time (TgDT) (17), tumor volume doubling time (TVDT) (18), and tumor growth slope (TGS) with PFS was evaluated (19). TgDT was calculated after the initiation of lenvatinib (TgDTpost) by a method used at Kuma Hospital (
As described in a previous study (19), TGS was the change from baseline in the sum of target lesions per month. TGSpre, the TGS in the pretreatment period, was calculated as (
Safety and adverse events
Safety and adverse events (AEs) were evaluated during follow-up visits by physical examination and laboratory tests. AE severity was graded using the National Cancer Institute Common Terminology Criteria for Adverse Events v4.03 (20). AEs were reported as lenvatinib-related when a causal relationship could not be ruled out.
Statistical analysis
The statistical analysis was performed with R version 3.4.0 (R Foundation for Statistical Computing; Vienna, Austria), and graphs were drawn with GraphPad Prism version 5.0 (GraphPad Software, San Diego, CA). Continuous variables are reported as medians and interquartile range (IQR), and categorical variables are reported as numbers and percentages. PFS and OS were estimated by the Kaplan–Meier method. Univariate regression analysis with calculation of hazard ratios (HRs) and their 95% confidence intervals [CIs] were used to identify patient baseline characteristics that were associated with survival. Differences with a two-tailed p-value <0.05 were regarded as significant.
Results
Patients
A total of 43 eligible patients with lenvatinib treatment for progressive RAI-refractory DTC were included. The baseline characteristics are summarized in Table 1. The median age was 67 years, 17 (39.5%) were men, and 32 patients (74.4%) had previously received sorafenib. Forty-one patients (95.3%) had lung metastases, and the lungs were the most frequent site of target lesions (58.1%). The median duration of lenvatinib treatment was 14 months (IQR 4.9–19.9), and the median follow-up from lenvatinib initiation to the time of the last censoring or death was 16 months (IQR 7.2–20.7). Lenvatinib was initially administered at a median dose of 20 mg/day (IQR 18–22). Thirty-two patients (74.4%) required dose reduction due to AEs; the median time to the first dose reduction was 3.3 months (IQR 1.7–7.3), resulting in median sustainable dose of 10 mg/day (IQR 10–14).
Baseline Patient Characteristics
Values are expressed in numbers (%) or medians (IQR).
FTC, follicular thyroid carcinoma; IQR, interquartile range; PDTC, poorly differentiated thyroid carcinoma; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; RECIST, Response Evaluation Criteria in Solid Tumors; Tg, thyroglobulin.
Efficacy
The median PFS was 21.8 months [CI 13.8–NE]. The median OS was not reached at the end of the observation period (April 30, 2019, Fig. 1). The median time to the first objective response was 3.8 months (IQR 2.4–10.4, Table 2). A CR was not achieved by any patient. PR was achieved by 18 patients (64.7%), SD in 24 patients (55.8%), and PD in 1 patient (2.3%). The overall disease control rate was 97.7%, and the clinical benefit rate was 86%. The tumor burden of the target lesions decreased in 90.7% of the patients (Fig. 2). At the end of the observation period, 17 patients had PD. Progression of the target lesion was observed in five patients (29.4%, 5/17), progression of a nontarget lesion occurred in one patient (5.9%, 1/17), new lesions developed in the target organ in six patients (35.5% 6/17, 35.5%), and new lesions developed in a nontarget organ in five patients (29.4%, 5/17).

Cumulative (
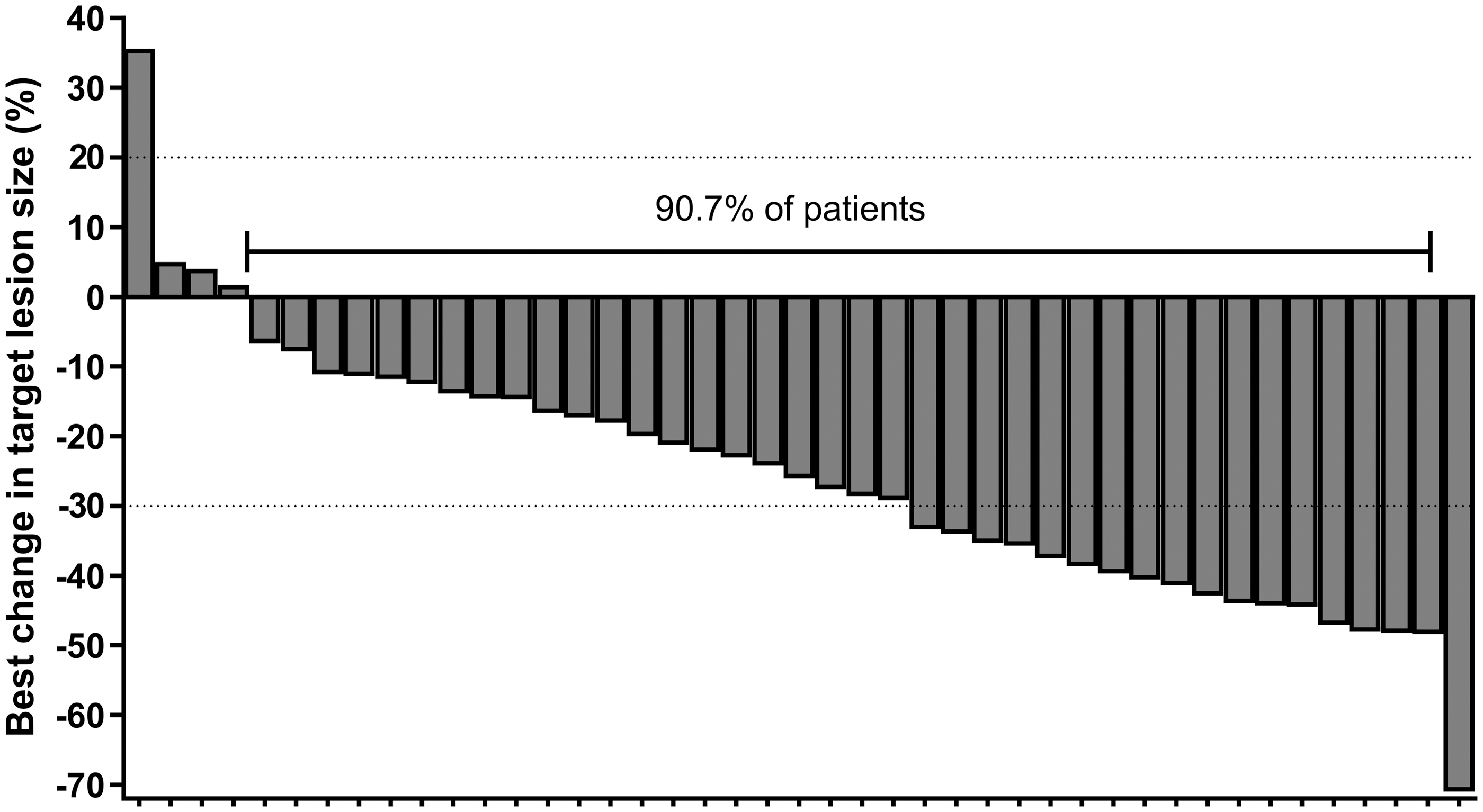
Greatest change of target lesion size from baseline after lenvatinib treatment.
Disease Response to Lenvatinib
CR + PR + SD.
CR + PR + SD at ≥23 weeks.
CR, complete response; PD, progressive disease; PR, partial response; SD, stable disease.
Factors associated with survival
Previous sorafenib treatment, metastatic sites (lung metastasis only vs. metastasis to other organs), daily sustainable dose of lenvatinib (≤10 mg vs. >10 mg), median baseline Tg (≥231.3 ng/mL vs. <231.3 ng/mL), and reduction in Tg (≥60% vs. <60%) were not significantly associated with PFS (Fig. 3 and Table 3). However, patients with a sum of the initial diameters of the target lesions of ≥5.2 cm (median value) had poorer PFS than their counterparts (HR = 2.66 [CI 1.02–6.96], p = 0.045, Fig. 3F and Table 3).

Progression-free survival according to (
Univariate Analysis of Patient and Tumor Growth Characteristics and Progression-Free Survival
Median of 5.2 cm.
CI, confidence interval; HR, hazard ratio; PFS, progression-free survival; Tg, thyroglobulin; TgDT, thyroglobulin doubling time; TGS, tumor growth slope; TVDT, tumor volume doubling time.
The analysis of the association of tumor growth rate found that TgDTpost was significantly associated with PFS (HR = 1.55 [CI 1.06–2.28], p = 0.024). The median TgDTpost was −3.2 months (−12.1 to −0.75). Neither TVDTpre (p = 0.923) nor TVDTpost (p = 0.966) had a significant impact on PFS. The median TVDTpre was 5.5 months (1.5 − 10.8), and the median TVDTpost was −6.2 months (−16.1 to −1.3). Figure 4 shows the pre- and post-treatment TGS of each of the patients. The median TGSpre was 2.8 months, and the median TGSpost was −4.6 months. The TGSpost/TGSpre ratio was −1.6. TGSpre (HR = 1.08 [CI 1.03–1.14], p = 0.003) and TGSpost (HR = 1.08 [CI 1.00–1.16], p = 0.039) were associated with an increased risk of disease progression. The TGSpost/TGSpre ratio was not significantly associated with PFS (p = 0.714).
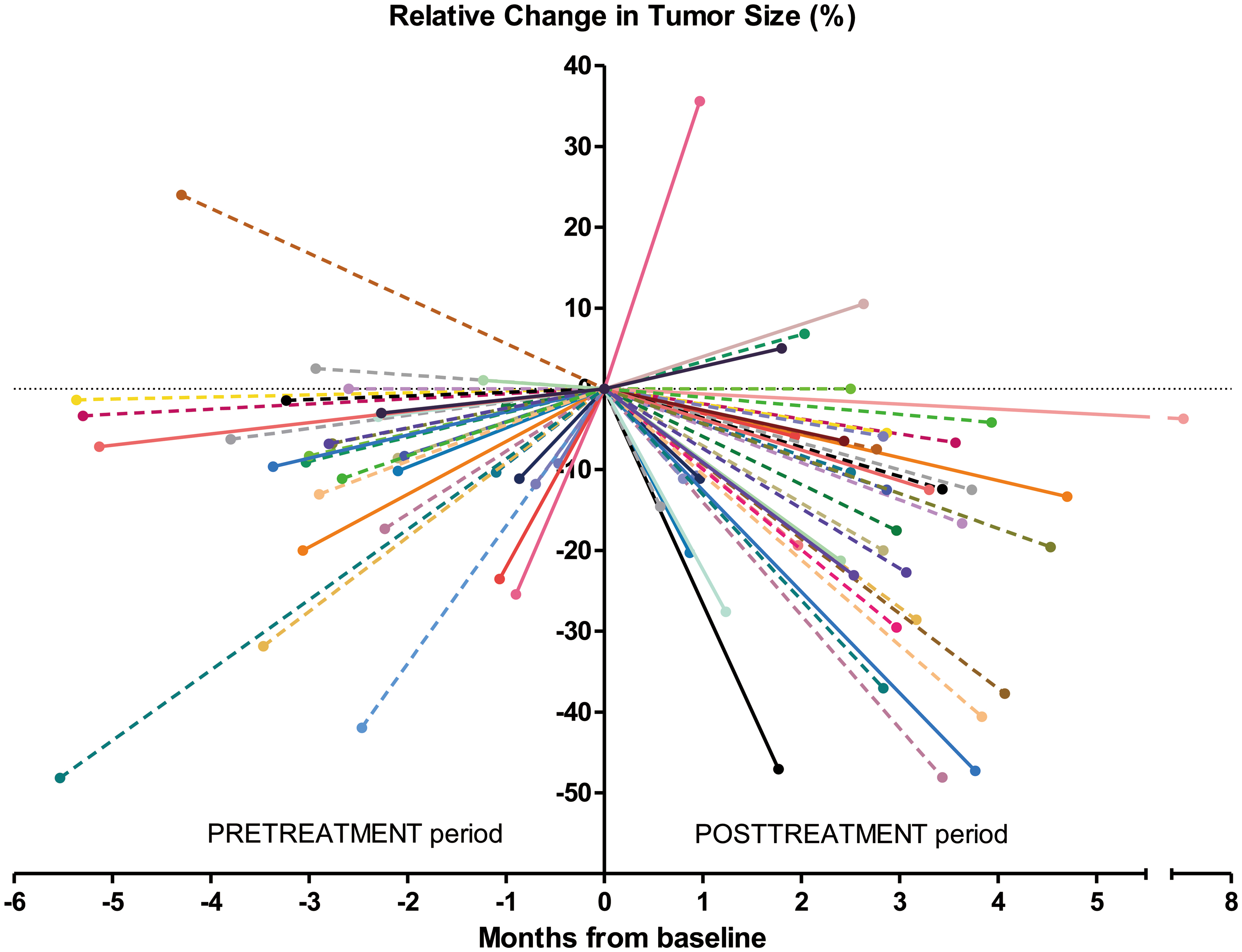
TGS of individual study patients representing the change in sum of the largest diameters of target lesions from baseline. TGS of patients with disease progression is plotted as continuous line and TGS of patients without disease progression is plotted as dotted line. TGS, tumor growth slope. Color images are available online.
Safety and adverse effects
AEs of any grade were observed in all patients, but grade 3–4 AEs occurred in only 10 patients (23.2%, Table 4). The most frequent AE was fatigue or asthenia (72.1%), followed by hypertension (62.8%) and proteinuria (58.1%). Lenvatinib was withdrawn in 24 patients (55.8%): in 6 patients (13.9%) because of AEs and in 18 patients (41.9%) because of disease progression or poor performance status.
Treatment-Related Adverse Events
Discussion
This multicenter, retrospective cohort study evaluated the efficacy and safety of lenvatinib in patients with progressive RAI-refractory DTCs. With a low sustainable dose of lenvatinib 10 mg/day, the median PFS was 21.8 months and the disease control rate was 97.7%, which supports the clinical benefit of lenvatinib in real-world practice. This result also indicates that reduced doses of lenvatinib in accordance with severe AEs do not abrogate its apparent efficacy in these patients. Tumor shrinkage was observed in 90.7% of the patients and 64.7% achieved PR. These efficacy outcomes were consistent with the findings reported by the SELECT trial despite a higher prevalence of bone metastasis in our study (11). Treatment-related AEs occurred in all study patients, but most were manageable. The percentage of severe grade 3–4 AEs was less in this study (23.2%) than in the SELECT trial (75.9%), which might be attributable to the low tolerated dose of 10 mg/day that was used here. The standard lenvatinib dose in the SELECT trial was 24 mg/day (11), which is based on the phase I trial reporting a maximum tolerated dose of 25 mg/day (21). However, the standard dose of 24 mg is based on data obtained in western populations, and thus, dose adjustment is required for Asian populations because of their smaller physique. A subgroup analysis of the SELECT trial reported that dose reduction was more frequent in Japanese patients (90%) than in the overall study population (67.8%) (22). Despite a starting dose of 20 mg/day in this study, 74.4% of the patients required an interruption of treatment or an early dose reduction. However, the PFS of patients receiving lenvatinib doses of more or less than 10 mg was not significantly different. Patients' quality of life can be maintained by appropriate dose reduction resulting in control of major AEs with provision of adequate efficacy.
Several clinical characteristics and tumor growth rate parameters were found to be associated with the prognosis during lenvatinib treatment. The PFS of patients treated with lenvatinib as first-line therapy or as second-line therapy after sorafenib was not different, which is in line with the SELECT trial results. The median PFS of patients previously treated with a TKI, mainly sorafenib, was 15.1 months. That is shorter than the median 18.2 months in drug-naive patients, but significantly longer than the 3.6 months with placebo administration. Salvage treatment with lenvatinib is the only available, and widely used, option in Korea for disease progression following first-line sorafenib treatment. Lenvatinib was effective as second-line treatment and was generally well tolerated in this patient series and should be considered as salvage therapy after sorafenib. The only clinical characteristic that had an impact on PFS was the sum of largest initial diameters of target lesions, which indicates that high tumor burden was associated with poorer prognosis. The results of a subgroup analysis of the SELECT trial also found that a smaller baseline tumor size (<median) was associated with a better PFS (HR = 0.61, p = 0.03) (23). Patients with very low tumor burden, that is, target lesions of <1.5 cm, were found to have less strong responses to TKIs, although this phenomenon is more evident with sorafenib than with lenvatinib (9). In this regard, it is important to choose an appropriate time to initiate TKI: not too early but not too late.
Recent studies highlight the importance of tumor growth rate, rather than the tumor size at one time point, as a key factor for deciding the optimal time to initiate TKI treatment or to predict the outcome of TKI treatment (19,23). In this study, TgDTpost was associated with PFS, but this was confined to 34 patients with a negative TgAb. Analysis of the impact of TGSpre and TGSpost on PFS, which reflect the tumor growth rates at pre- and post-treatment period (19), confirmed that patients with faster growing tumors at baseline (higher TGSpre) and patients with a slower decrease of tumor burden (higher TGSpost) had poorer survival. The TGSpost/TGSpre ratio did not have any impact on PFS. The results are not in agreement with those reported by Suzuki et al. who investigated the prognostic value of TGS in 30 patients receiving lenvatinib for RAI-refractory DTC (19). That study found no association of TGSpre with PFS but did find that TGSpost and the TGSpost/TGSpre were associated with PFS. The discrepancies might be explained by differences in the patient cohorts. Most patients included by Suzuki et al. (96.2%) received lenvatinib as first-line treatment for fast-growing aggressive disease. Additional study is needed to validate the prognostic value of TGS in larger prospective studies.
The study limitations include, first, the retrospective nature, which cannot eliminate selection bias and limits the evaluation of prognostic values of clinical parameters. Second, information on patient body surface area or body weight was lacking and could not be included in the evaluation of lenvatinib effectiveness after adjusting for these factors. Third, because most of the patients had disease-related symptoms before the administration of lenvatinib, the association of survival outcome with the presence of symptoms, which is an important consideration during sorafenib treatment (24), could not be evaluated. Despite these limitations, the study identified important clinical characteristics and tumor growth rate parameters as candidate biomarkers associated with survival during lenvatinib treatment in real-world practice.
In conclusion, lenvatinib was effective for treating patients with advanced RAI-refractory DTCs, with a median PFS of 21.8 months. Although lenvatinib was reduced to a median sustainable dose of 10 mg/day in accordance with patients' AEs, adequate efficacy of lenvatinib was still observed with an eventual low frequency of severe AEs. TgDT and TGS helped to predicting the clinical outcomes of these patients.
Footnotes
Author Disclosure Statement
Y.K.S. and W.B.K. have received consultation fees and honoraria from Bayer and Eisai.
Funding Information
The authors received no specific funding for this work.