
Abstract
Background:
The 2015 American Thyroid Association (ATA) clinical practice guidelines (CPGs) on management of thyroid nodules (TNs) and differentiated thyroid cancer (DTC) in adults were developed to inform clinicians, patients, researchers, and health policy makers about the best available evidence, and its limitations, relating to management of these conditions.
Methods:
We conducted a cross-sectional electronic survey of ATA members' perspectives of these CPGs, using a standardized survey (Clinician Guidelines Determinant Questionnaire) developed by the Guidelines International Network. A survey link was electronically mailed to members in February of 2019, with reminders sent to nonrespondents 2 and 5 weeks later. Data were descriptively summarized, after excluding missing responses.
Results:
The overall response rate was 19.8% (348/1761). The effective response rate was 20.2% (348/1720), after excluding a recently deceased member and individuals who had either invalid e-mail addresses or whose e-mails were returned. Of the respondents, 37.9% (132/348) were female, 60.4% (209/346) were endocrinologists, 27.5% (95/346) were surgeons, and 3.5% (12/346) were nuclear medicine specialists. The majority of respondents (71.9%; 250/348) were at a mid- or advanced-career level, and more than half were in academia (57.5%; 195/339). The majority (69.8%; 243/348) practiced in North America. The vast majority of respondents indicated that the CPGs explained the underlying evidence (92.3%; 298/323) and 92.9% (300/323) agreed or strongly agreed with the content. Most respondents stated that they regularly used the CPGs in their practice (83.0%; 268/323). Most respondents (83.0%; 268/323) also agreed or strongly agreed that the recommendations were easy to incorporate in their practice. The most popular CPG format was an electronic desktop file (78.8%; 252/320). Shorter more frequent CPGs were favored by 55.0% (176/320) of respondents, and longer traditional CPGs were favored by 39.7% (127/320).
Conclusions:
The clinical content and evidence explanations in the adult TN and DTC CPGs are widely accepted and applied among ATA survey respondents. Future ATA CPG updates need to be optimized to best meet users' preferences regarding format, frequency, and length.
Introduction
Clinical practice guidelines (CPGs) have become an increasingly important and prevalent aspect of the management of diverse medical conditions (1). CPGs are intended to guide rather than mandate (2), and need to be adapted in practice, bearing in mind the individual patient's clinical situation/contextual factors, the patient's values and preferences, and feasibility considerations. CPGs should transparently report the limitations of the evidence upon which their recommendations are based and recognize that the evidence landscape is constantly evolving. Nevertheless, CPGs increasingly influence standard practice, and may be applied by insurance companies and third-party payors to determine coverage for a particular course of action recommended by a physician.
Several challenges have generally beset the groups developing CPGs (3), including, but not limited to, conflicts of interest and their management (4,5), expenses related to systematic reviews and methodology expertise in the appraisal of the evidence, representation of the diverse view of different specialists (6 –8), formulating clinically useful recommendations in the absence of high-quality evidence while highlighting evidence uncertainties and relevant options (9), especially in the case of common medical conditions (10 –12).
The American Thyroid Association (ATA) is a professional society for all the constituents involved in research into and implementation of clinical care for those with thyroid disorders. The most frequently downloaded ATA CPG is the 2015 guideline addressing the management of thyroid nodules (TNs) and differentiated thyroid cancer (DTC) in adults (13), which has been downloaded a total of 726,277 times and cited by 2314 publications as of June, 2019 (personal communication Peter Kopp, Editor-in-Chief of Thyroid). The literature reviews that informed this CPG were conducted between 2012 and 2014, and the American College of Physicians Guideline Grading System was used for critical appraisal of evidence and grading strength of recommendations for therapeutic interventions (13).
The ATA commissioned a task force in 2017 to assist the organization in maintenance and strengthening of the quality and relevance of their CPGs (14). This task force became a standing committee of the ATA in 2018. The survey described here was launched by the ATA Guidelines and Statements Committee to inform the ATA about member perceptions and utilization of the TNs and DTC CPGs. The information collected in this survey was intended to inform the development of future ATA CPGs.
Methods
We conducted a cross-sectional electronic survey of ATA members' perspectives of the 2015 ATA CPGs on TNs and DTC in adults. We identified all current ATA members, using an updated member database maintained by the organization. The e-mail addresses of members were retrieved from this database. All ATA staff (who were members) were excluded. A link to the electronic survey was e-mailed to ATA members in mid-February 2019 and nonresponders were sent an e-mail reminder 2 and 5 weeks later. The survey link was accompanied by an e-mail message explaining that the purpose of the survey was to assist the operations of the ATA and the ATA Guidelines and Statements Committee. Furthermore, it was stated that the aggregate results of the survey would be published, but that individual responses would remain anonymous, and that consent was implied by completion of the survey. The survey was closed on April 3, 2019. The survey was conducted online (Survey Monkey [R], San Mateo, CA). Data from the survey were extracted in a deidentified manner and exported into an electronic spreadsheet (Excel, Microsoft Corporation, Redmond, WA). The intended survey population received no monetary compensation. Institutional Research Ethics Board approval was waived by the University Health Network, in Toronto Canada, as the study was considered a quality assurance study conducted on behalf of the ATA.
We utilized the Clinician Guideline Determinants Questionnaire, which is a validated instrument that comprehensively addresses potential determinants of CPG use from a clinician perspective (15). This questionnaire was developed by Gagliardi et al. of the Guidelines International Network to enable CPG developers to tailor guideline implementation planning to user needs and preferences, with the intention of achieving improved CPG utilization, optimization of health care delivery, and improved clinical outcomes (15). The survey was adapted, incorporating some specific explanations relevant to ATA members, and targeting the questions to the most widely read and cited ATA CPGs, which addresses the management of TNs and DTC (13).
The sections of the survey include background information on the respondents, respondents' opinions about the CPGs, and its implementation in clinical practice, medical learning preferences of the respondents (including sources used for medical decision-making, preferred CPG format, preferred means of accessing future ATA guidelines, and ideas for future guidelines), and a section for general comments. The survey is available as Supplementary Data. The questionnaire included yes/no/unsure, multiple choice, and Likert scale questions (on a 5-point scale from strongly disagree to strongly agree).
The data were summarized descriptively, after excluding missing responses. Categorical responses were reported as the number and percentage. Post hoc secondary comparisons of characteristics of survey respondents and nonrespondents were performed using chi-squared tests (PASW Statistics for Windows, Version 18.0, SPSS, Inc., Chicago, Illinois). For any statistical comparisons, the alpha level of statistical significance was assumed to be 0.05.
Results
Respondent characteristics
We e-mailed a link to the survey to 1761 ATA members for whom we had e-mail address contact information (Fig. 1). Of those e-mail recipients, 19.9% (351/1761) opened the e-mail. Most of the members who opened the e-mail, 99.2% (348/351) participated in the survey. The overall response rate was 19.8% (348/1761). The effective response rate after excluding a recently deceased member and individuals who had either invalid e-mail addresses or whose e-mails were returned was 20.2% (348/1720) (Fig. 1). The majority of respondents completed the survey in its entirety (90.2%; 314/348). The detailed characteristics of respondents are reported in Tables 1 and 2. Most respondents were either adult endocrinologists (60%) or surgeons (28%), the majority were male (62%), and most worked in an academic setting (58%). As given in Table 2, there were some differences in age and specialty areas of respondents compared with nonrespondents, with a relative under-representation of training/early career respondents and relative over-representation of surgical specialists among respondents.

Flow diagram of study participants.
Survey Respondent Characteristics
Excludes missing responses.
Comparison of Demographic Composition of Respondents and Nonrespondents
Data from the ATA member database. The nonrespondents in this table include 6 individuals whose e-mails were rejected (e-mail bounced back) and 1 individual who was deceased.
ATA, American Thyroid Association.
Respondents' personal determinants relating to guideline use
Approximately 33% (115/348) of respondents indicated that they had some prior personal experience in CPG development (i.e., for any organization, on any topic). The majority of respondents reported reading all or part of the ATA CPGs on multiple occasions (89.5%; 289/323), whereas 8.7% (28/323) had read all or part of the CPGs once and only 1.9% (6/323) had never read the CPGs. Moreover, the majority of respondents indicated that they clinically applied the ATA CPGs on multiple occasions 83.0% (268/323); furthermore, 14.2% (28/323) applied the CPGs once to a few times and only 2.8% (9/323) never applied the CPGs. A summary of respondents' additional personal determinants of CPG use and CPG preferences is given in Table 3. Some personal views and opinions expressed by ATA members that could potentially promote ATA CPG utilization included endorsement of a belief that CPGs optimize health care delivery and outcomes (93.1%; 324/348), a personal practice of obtaining information for clinical decision-making from CPGs (87.2%; 279/320), and the medical literature 88.1% (282/320), as well as a strong belief that following these guidelines was part of one's professional responsibility (83.3%; 269/323).
Some of the Respondents' Personal Determinants Relating to Clinical Practice Guidelines Use and Clinical Practice Guidelines Preferences
Excludes missing responses.
CPGs, clinical practice guidelines.
Self-reported personal and professional characteristics of members that would allow them to incorporate the ATA CPG recommendations in their clinical practice included having the necessary clinical training (89.8%; 290/323), clinical knowledge (97.5%; 315/323), skills (96.6%; 312/323), and practice autonomy/individual capacity (90.4%; 292/323). About two-thirds of respondents reported organizational support for utilization of the ATA CPGs (64.1%; 207/323). Most participants (81.7%; 264/323) indicated that colleagues within their organization used the CPGs and 70.9% (229/323) indicated that their colleagues or practice group expected them to use this CPG. Furthermore, 63.2% (204/323) of participants indicated that they believed that colleagues outside their organization used this CPG.
In self-reporting their preferred means of learning about a new CPG, respondents were invited to select all answers that applied. The top three preferred venues for learning about new CPGs were publication in a journal (70.6%; 226/320), educational meetings (62.5%; 200/320), and the ATA website (53.1% (170/320) (with some individuals selecting more than one option). The three most preferred formats for accessing guidelines were electronic desktop file (78.8%; 252/320), a printed copy from the ATA journal (38.4%; 123/320), and mobile applications (37.8%; 121/320). Other preferred formats were succinct electronic file summaries (33.4% (107/320) and electronic files on the ATA website (32.5%; 104/320). In describing one's preferred frequency and length of future ATA CPGs, respondents' preferences were as follows: 39.7% (127/320) preferring long comprehensive CPGs updated every 3–5 years (the status quo), 43.1% (138/320) preferring short specific modules updated every 2 years or less, and 11.9% (38/320) preferring a clinical pathway or algorithm updated yearly. Of the 127 individuals selecting the status quo of long comprehensive relatively infrequent guidelines, 80 (63.0%) were men, 76 (59.8%) were in academic practice, 74 (58.3%) were adults or pediatric endocrinologists, and 88 (69.3%) were at mid- or advanced career level. These demographic and professional characteristics appeared relatively similar to those observed in the entire survey respondent population (Table 1).
Evaluation of the ATA CPGs
The vast majority of respondents agreed or strongly agreed with the content of the ATA CPGs (92.9%; 300/323) and 89.2% (288/323) believed that adoption of the recommendations in this CPG would improve the quality of health care delivery (Table 4). Approximately three-quarters of respondents reported that they found the wording of recommendations clear and unambiguous (73.7%; 238/323), and about two-thirds reported the format and layout to be easy to navigate to find information (64.1%; 207/323). Most participants 83.0% (268/323) found it easy to incorporate the recommendations in their practice.
Evaluation of the 2015 American Thyroid Association Clinical Practice Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer (Likert Scale Questions)
Excludes missing responses.
Furthermore, 92.3% (289/323) of respondents indicated that the ATA CPGs clearly described the evidence underlying recommendations and 88.9% (287/323) indicated that the recommendations were consistent with the evidence (Fig. 2). Advantages associated with the CPGs, such as informing decision-making or patient communication, were reported by 88.9% (287/323) of respondents, and disadvantages such as time, learning curve, or costs were reported by a minority of respondents (13.6%; 44/323). Only ∼33% of respondents (109/323) perceived that the CPGs incorporated patient input (regarding guideline questions, methods, and recommendations); yet nevertheless about three-quarters of respondents thought the CPG was consistent with their patients' values and preferences (78.0%; 252/323). Furthermore, patient acceptance/adherence with the recommendations was reported by 79.6% (257/323) of respondents. About two-thirds of respondents (64.7%; 209/323) reported awareness of implementation tools (such as clinician summaries, patient summaries, algorithms, and medical record forms) that may enable the CPGs to be used in clinical practice. Finally, 80.8% (261/323) of respondents believed that the ATA CPGs would lead to improved patient outcomes.
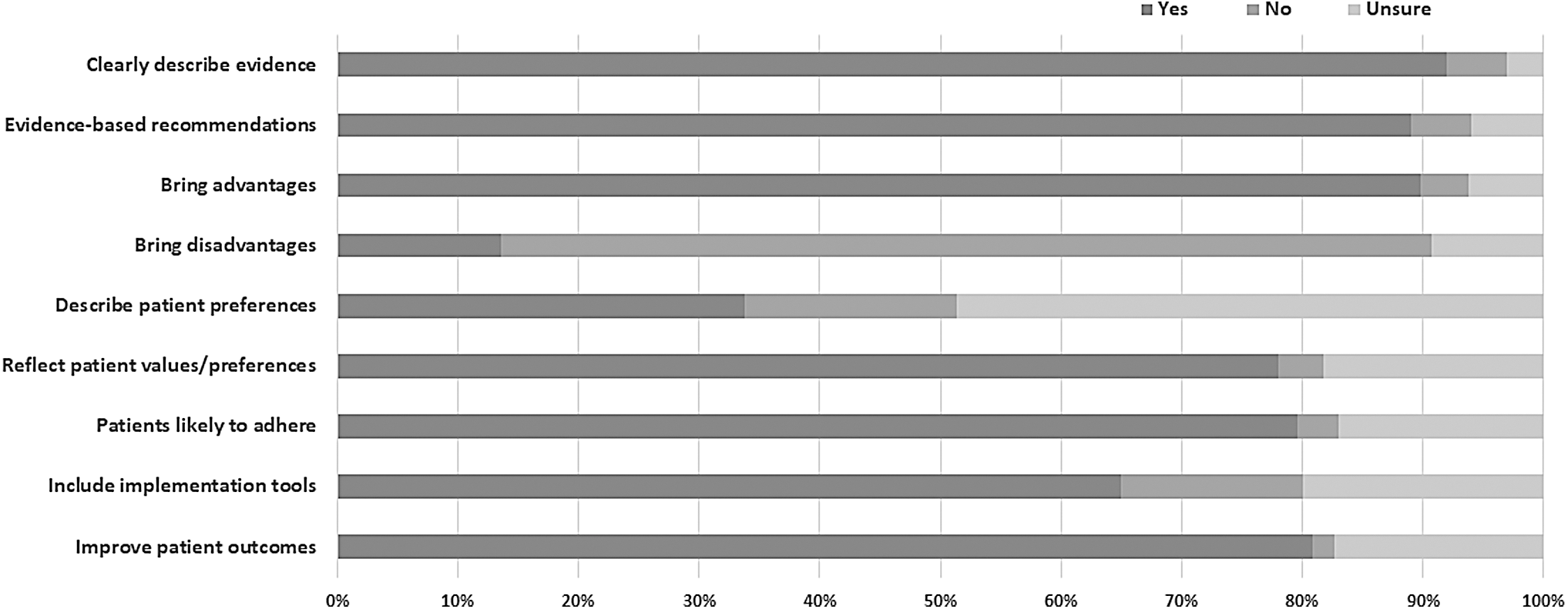
Respondents' opinions on the patient care-related implications of the 2015 ATA guidelines for management of thyroid nodules and differentiated thyroid cancer in adults. ATA, American Thyroid Association.
Discussion
As previously reported in the literature, in general, CPGs are underutilized (15). The management of TNs and DTC are both areas in which there are few randomized and controlled clinical trials and little high-quality evidence (13). Therefore, it is particularly important to note that ATA member respondents reported trusting and implementing this CPG, reflecting that it was transparent evaluation of the best currently available evidence. ATA member respondents utilized the CPGs and perceived that it was beneficial to their clinical practice. Furthermore, ATA member respondents' confidence in the CPGs extended to the belief that it was a professional responsibility to implement the CPGs. Factors that may have contributed to these findings could include bias among responders (with those who preferentially favored the guideline being more likely to respond to the survey, which may be relevant with a low response rate), an appreciation of the discussion accompanying recommendations that could enable meaningful interpretation of contextual factors and discussion with patients about disease management options (particularly in the context of weak recommendations based on low-quality evidence, where more than one option may be reasonable, depending on the clinical circumstance and patient preference), and possibly respect and loyalty to the ATA and its mission, or respect of the opinion of guideline panelists.
The ATA CPGs on management of TNs and DTC have been subject to some controversies (2). Some of these controversies relate to the use of radioactive iodine. Several nuclear medicine professional societies declined endorsement of the 2015 ATA guidelines (8,16). However, only 4% of ATA member survey respondents reported belonging to nuclear medicine specialty societies. Yet, even among nuclear medicine specialists, some disagreement about interpretation of the ATA CPGs is evident, as Frangos et al. have indicated that the 2015 ATA guidelines “better acknowledge grey areas” than in the past (17). Interdisciplinary efforts in achieving meaningful academic discourse on controversial issues are actively being pursued (6,7).
Some examples the challenges that the ATA TN and DTC CPG panelists faced included resource limitations (as literature searches, critical appraisal of literature, and writing of recommendations, and the article was undertaken by clinicians and clinician-scientists on a volunteer basis [with no dedicated funds for systematic reviews]), limited availability of high-quality evidence upon which to base recommendations (with the challenge of formulating clinically meaningful recommendations using the best available evidence, which was often low in quality), and managing competing interests of some panelists (under oversight of the ATA ethics committee). The comprehensive approach taken to address a broad clinical content area, encompassing both TNs and DTC (yielding a large volume of literature for review) also presented a barrier to timely publication of this CPG. Clearly, there is a need for more long-term outcome randomized controlled trials and prospective observational research to guide treatment decision-making regarding thyroid neoplasms. Randomized controlled trials examining the use of radioactive iodine remnant ablation in low-risk DTC are currently ongoing [Estimabl2 (18); iodine or not (19) and highly likely to influence future clinical practice.
In the limited time since publication of the ATA TNs and DTC CPGs, one study has reported that rates of hemithyroidectomy, as opposed to total thyroidectomy, have increased in the United States, with ∼10-fold quarterly increase in hemithyroidectomy rates adjusted for patient factors (20). Furthermore, rates of outpatient thyroidectomy and short-term surgical complications were reported to significantly decrease during this period (20). It is premature to infer causality and to postulate long-term outcomes with respect to changes in treatment trends after publication of the ATA CPGs. These findings may not be extrapolated to other countries. Further research is needed to validate these findings and explore the relationship between CPG recommendations, health care utilization (such as surgery, radioactive iodine remnant ablation or treatment, or others), and long-term health outcomes, both within the United States and other countries.
The finding that almost equal number of respondents preferred lengthy comprehensive CPGs versus shorter modules that were updated more frequently represents a dilemma for future ATA CPG developers. CPGs necessitate a considerable outlay of society and member resources. However, it should be feasible to satisfy both audiences by having a comprehensive CPG that comprises component modules that are updated at shorter intervals based on the available literature, with a major rewriting of the CPG thus only becoming necessary after a longer time has elapsed.
This survey identified at least two areas in which a future TN and DTC CPG could expend additional effort and provide further clarity. These areas involved patient participation (21,22) and implementation tools (23 –25). Respondents to this survey were unsure whether patient input was an integral part of the CPG development, although they nevertheless thought that the CPGs were consistent with their patients' values and preferences and that patients were likely to adhere to the CPG recommendations. Future CPGs can employ a formalized framework for patient involvement (22) that is fully described to clinicians who are using the CPGs. Some respondents were either unsure whether implementation tools were part of the CPGs or unsure as to whether such tools were helpful. Adequate provision of implementation tools for CPGs has been identified as an area requiring attention (26), and models have been developed to aid in the implementation of CPGs (23). Focusing attention on this aspect of CPGs could facilitate the yearly updates in clinical pathways and algorithms that were requested by some ATA members.
Although this survey provides very useful information to guide the ATA and the ATA Guidelines and Statement committee in their future activities, there are several limitations of this study. Foremost, the response rate to the survey was only ∼20%. While the response rate is similar to that seen in other ATA surveys [20% (27)] or professional society surveys [13.6% for ATA, 10.9% for the Endocrine Society, and 9% for the American Association of Clinical endocrinologists (28)], this low response rate does raise concerns about whether the responses are generalizable to the ATA membership as a whole, particularly with under-representation of early career trainees and professionals and possible over-representation of surgeons. Furthermore, the low response rate limits generalizability of the findings to nonresponding clinicians who are ATA members, as well as those who are not members. Most of the nonrespondents did not open their invitation e-mails from the ATA. The reasons for not opening such e-mails cannot be known. We did not survey physicians outside of the ATA membership database. There is some evidence from a systematic review of oncology physician surveys that paper-based surveys with monetary prepaid incentives may be associated with higher response rates than e-mail or online surveys (29).Yet modest monetary incentives with online surveys may not necessarily be associated with a significant increase physician survey response rate (30). Paper-based surveys with monetary incentives were not feasible for this study, given financial limitations; such surveys could be considered by the ATA in the future for priority topics. In considering potential nonresponse bias, a prior survey of the management of hypothyroidism suggested that those who were more junior tended to follow CPG recommendations (27); thus, because of possible under-representation of early career professionals in this survey, it is likely that CPG adoption is underestimated in this group as a whole. Furthermore, 33% of respondents indicated that they had personally participated in a CPG for a professional society, again potentially limiting the generalizability of the responses. Finally, the ATA member list that was used for electronic distribution of the survey and the nonresponder analysis may be potentially subject to some inaccuracies in contact information or description of members as it is not a validated research database. Another potential limitation of this work is that several coauthors (A.M.S., B.R.H., and S.J.M.) were coauthors of the original ATA CPGs under evaluation, and one author was editor of the journal in which the guidelines were published (P.A.K.), reflecting potential duality of interest. It is also possible that professional clinical or research relationships with any of the coauthors on the original CPGs or the survey article may have influenced some responses. Such limitations may limit the interpretation of implementation of the guideline recommendations. Future epidemiologic work, examining health care utilization and outcomes after publication of these guidelines, will be essential.
CPGs have become an integral part of the practice of most endocrinologists. The management of TNs and DTC is a particularly complex and controversial field (7,8). It is, therefore, notable that, based on feedback from our members, these ATA CPGs are heavily consulted, widely applied in clinical care, and considered to represent a practice pattern that brings benefits to both physicians and patients.
Footnotes
Acknowledgments
The authors thank all the ATA members who took the time to respond to this survey. This article was approved by the ATA Board of Directors.
Author Disclosure Statement
There are no financial competing interests. Three coauthors of this article (A.M.S., B.R.H., and S.J.M.) were coauthors on the guideline under evaluation in this survey and one author was editor of the journal wherein the guidelines were published (P.A.K.).
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data