
Abstract
Background:
Although international guidelines have become more conservative on the use of radioactive iodine (RAI) therapy, it is still one of the cornerstones of the treatment of patients with advanced differentiated thyroid cancer (DTC). As a large proportion of females diagnosed with DTC is in their reproductive years, knowledge about the effect of RAI on their gonadal and reproductive function is important. Earlier studies evaluating Anti-Müllerian hormone (AMH) as a representative of ovarian reserve were either cross-sectional, had relatively low numbers, had no patients with multiple RAI therapies, or had a relatively short follow-up. The primary aim of our study was, therefore, to prospectively evaluate the effect of RAI on AMH in women undergoing treatment for DTC.
Methods:
We included females, aged 16 years until menopause, who were scheduled to undergo their first RAI treatment for DTC at our hospital. Serum AMH was measured before initial therapy and regularly thereafter. Repeated measurement analysis was used to assess the changes of AMH concentrations over time, and how this is influenced by age and cumulative RAI dose.
Results:
Longitudinal AMH assessments were available in 65 patients (mean age 32 years, median of five measurements during median follow-up of 34 months). AMH concentrations changed nonlinear over time, decreased until 12 months in the single RAI group (−55%), and stabilized thereafter. In the multiple RAI group, after stabilization, a further decrease occurred (−85% after 48 months). Age in both RAI groups significantly influenced AMH change over time, with younger patients (<35 years of age) showing a less steep decrease.
Conclusions:
In a population of female DTC patients treated with total thyroidectomy and a single RAI therapy, AMH concentrations significantly dropped during the first year after initial therapy, and thereafter they remained stable. In patients receiving multiple RAI therapies, a further decrease was seen. Age at baseline significantly influenced AMH change over time. These results support a less aggressive treatment with RAI in low-risk patients as is advocated in the current American Thyroid Association (ATA) guidelines, especially in females older than 35 years of age with the desire to have a child.
Introduction
The worldwide incidence of differentiated thyroid cancer (DTC) has been steadily increasing over the past two decades (1,2). As mortality has remained stable, a less aggressive therapy seems more appropriate (1 –3). For this reason, current American Thyroid Association (ATA) guidelines recommend less extensive surgery in low risk tumors, and more restricted use of radioactive iodine (RAI) therapy (3), but controversies remain (4). Nevertheless, RAI is still one of the cornerstones of the treatment of patients with DTC, particularly in more advanced stages (3,5). DTC occurs more frequent in females than it does in males, and a large proportion of these female patients is in their reproductive years (2). Disease-specific survival in these young females is generally very good (6,7), leading to important questions about the influence of RAI therapy on their reproductive function.
Earlier studies showed a transient change of the menstrual cycle in 12–31%, and a temporary increase of follicle stimulation hormone during the first year after RAI therapy (8 –10). However, no increased infertility rates or adverse obstetric outcomes were seen in patients after RAI therapy (8,9). Further, four recent studies evaluated Anti-Müllerian hormone (AMH) as a representative of ovarian reserve in patients with DTC receiving RAI therapy (11 –14). AMH is relatively insensitive to inter- and intra-cycle variability and oral contraceptive use, is known to gradually decline with age, and is undetectable at menopause (15 –18). Therefore, AMH seems to be a good marker for ovarian reserve. Cross-sectionally, results were mixed as one study showed that AMH concentrations were significantly lower in patients who received RAI than in controls (13), but another study showed no significant differences (14). Earlier longitudinal studies showed a significant decrease of AMH concentrations when comparing concentrations just before RAI therapy with concentrations 12 months later (11,12). Thus, these earlier studies investigating the effects of RAI on AMH concentrations were either cross-sectional, had relatively low numbers, had no patients with multiple RAI therapies, or had a relatively short follow-up. The primary aim of our study was, therefore, to investigate the long-term effects of RAI therapy on AMH concentrations in female patients undergoing treatment for DTC.
Materials and Methods
Study population
We aimed at including all females, aged 16 years until menopause, who were scheduled to undergo treatment for DTC at the Erasmus Medical Center, Rotterdam, The Netherlands. Inclusion period was from January 2013 until December 2017, and patients were followed for at least one year. All included patients had tumors ≥1 cm and received a total thyroidectomy followed by RAI therapy according to the current Dutch guidelines (19). At baseline, that is, before surgery, just before RAI therapy, six to nine months later, and regularly thereafter, serum AMH measurements were performed. In addition, if a patient received more than one RAI therapy, just before a new therapy, and six to nine months thereafter additional AMH measurements were performed. As AMH concentrations typically do not fluctuate, the blood samples were not taken at a specific point during the menstrual cycle. Serum AMH concentrations were measured by using the AMH Gen II enzyme-linked immunosorbent assay (Beckman Coulter, Brea, CA), and they were expressed in μg/L.
Next to AMH measurements, we recorded demographic, disease, and treatment characteristics. Demographical variables included age at diagnosis and body mass index. Disease characteristics included disease type, American Joint Committee Cancer/TNM stage (eighth edition), and ATA Risk Stratification category (2015). Data regarding treatment consisted of number of RAI therapies, method of thyrotropin (TSH) stimulation before first RAI therapy (either three to four weeks of thyroid hormone withdrawal, or two subsequent injections with recombinant human TSH [rhTSH]), and cumulative dose of RAI. Further, childbirth rates were recorded during follow-up, and at end of follow-up, using a questionnaire, patients were asked about the influence of thyroid cancer diagnosis and treatment on their desire to have a child. The study was approved by the Institutional Review Board of the Erasmus Medical Center.
Statistical analysis
For continuous variables, means and standard deviations, or medians with interquartile ranges (IQR) were calculated. For categorical variables, absolute numbers with percentages were recorded. To assess the changes of AMH concentrations over time while accounting for the correlation between the repeated measurements of each patient, we used marginal models; the appropriate random-effects structure that best fitted the data was selected. To obtain a normal distribution for AMH concentrations, a log transformation was applied. Further, using a marginal model allows AMH measurements to be collected without predefined time points and therewith strengthens analysis. Analyses were performed separately for patients receiving one or multiple RAI therapies (single RAI and multiple RAI group, respectively). Our main goal was to assess changes in AMH concentrations over time. Further, additional analyses were performed to explore the effect of age (<35 years vs. ≥35 years), RAI preparation method (withdrawal vs. rhTSH), and cumulative RAI dose on AMH changes over time. In general, p-values below 0.05 were considered significant. The possibility of effect modification was studied by using a two-step strategy. First, a screening p-value cut-off for interaction of <0.10 was used, because the statistical power to identify an interaction term is less than for normal covariates. Second, to make sure that we did not identify irrelevant modification, we subsequently performed stratified analyses to replicate and quantify the effect modification so that we can interpret whether the differences are of (clinical) relevance. All analyses were performed by using either SPSS Statistics for Windows (version 24.0) or R statistical software (version 3.4.1).
Results
Population characteristics
During the inclusion period, a total of 85 female patients were eligible for the study, of whom 12 were not included because they either refused to participate (n = 5) or were missed at inclusion (n = 7). Next to this, eight patients had less than two AMH measurements and were subsequently excluded. Therefore, the analyses presented here were performed in the remaining 65 patients.
Table 1 lists the characteristics of the study population. Mean age was 32.0 years, and 59 (91%) had papillary thyroid carcinoma. Almost all patients (94%) had stage I disease. All patients received a total thyroidectomy followed by RAI therapy in correspondence with the current Dutch guidelines. Forty-seven patients received one RAI therapy (median dose 50 milliCurie [mCi]; 25–75 IQR: 30–146 mCi), and the other 18 patients received two or three therapies (median dose 291 mCi; 25–75 IQR: 284–293 mCi).
Characteristics of the Study Population
Values are means (±standard deviation), medians (25–75 IQR), or numbers (percentages).
p-Value comparing single and multiple RAI group. Significant p-values displayed in bold.
AJCC, American Joint Committee Cancer; AMH, Anti-Müllerian hormone; ATA, American Thyroid Association; mCi, milliCurie; RAI, radioactive iodine; TT, total thyroidectomy.
Anti-Müllerian hormone
For the total population, median follow-up from first RAI therapy to final AMH measurement was 34 months, and during this time a median of five measurements (25–75 IQR: 3–5) were taken. Median follow-up was six months longer for the multiple RAI than for the single RAI group.
Using repeated measurement analysis, AMH concentrations showed a significant nonlinear change over time in both RAI groups (Fig. 1 and Table 2). For the single RAI group, after initial therapy AMH, concentrations significantly dropped with the lowest values after 12 months (−55%; p < 0.0001). Thereafter, AMH concentrations remained stable. For the multiple RAI group, after initial therapy, AMH concentrations significantly dropped (−74%; p < 0.001), and after a short stabilization phase again started to decrease. AMH concentrations after 48 months were significantly lower in the multiple RAI than in the single RAI group (p = 0.005).
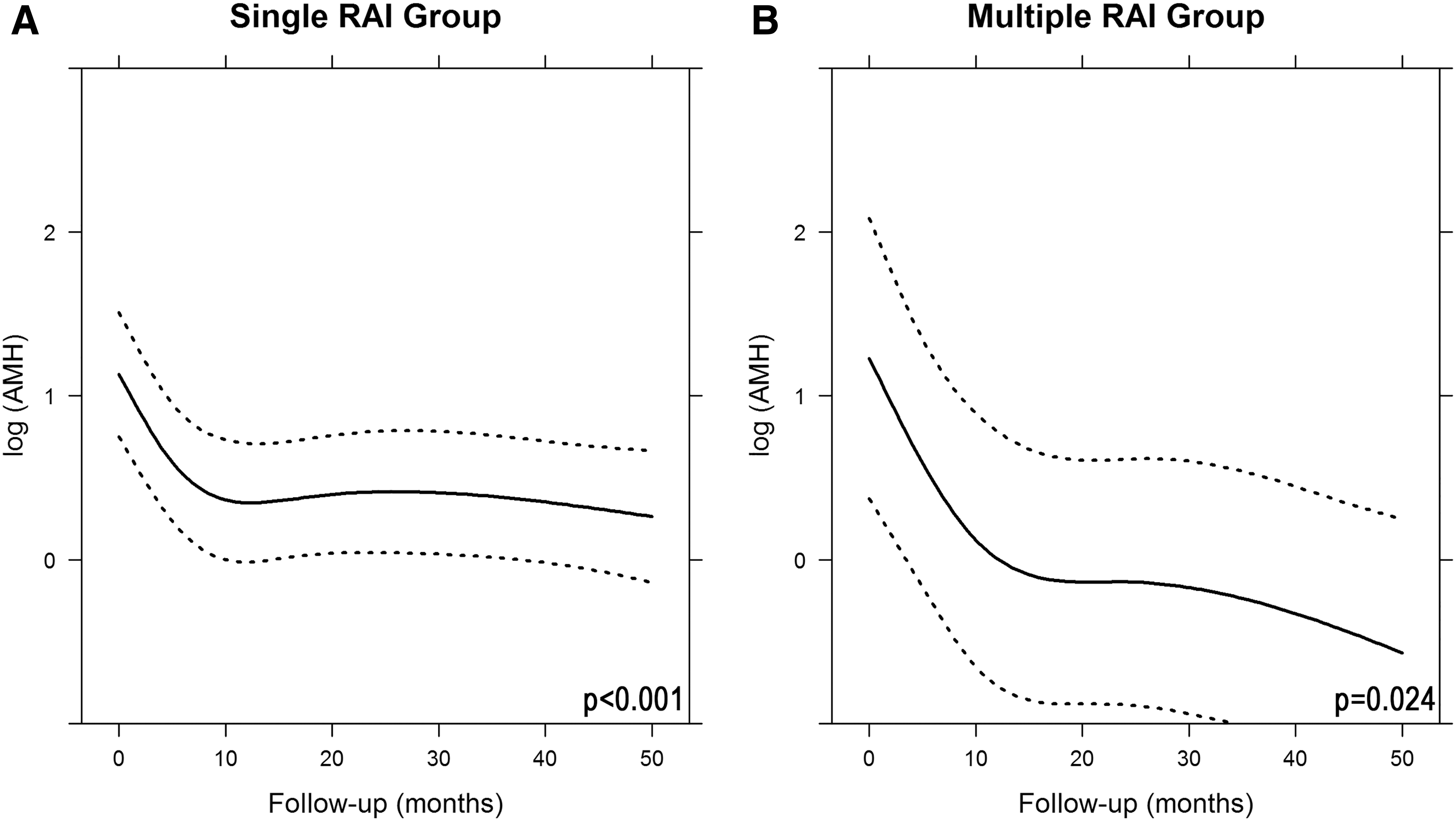
AMH concentrations over time for (
Anti-Müllerian Hormone Concentrations During Follow-Up
Values are means (±standard error) in μg/L obtained from created model.
Significant change from baseline (p < 0.05).
Age significantly influenced AMH change over time in both RAI groups (Figs. 2 and 3). In patients younger than 35 years of age, AMH concentrations showed a less steep decrease during the first year compared with patients older than 35 years (for single RAI group: −46% vs. −71%). Cumulative RAI dose did not significantly influence AMH concentrations in both RAI groups separately. In addition, we also did not find a difference in the single RAI group between females receiving <50 mCi and those receiving ≥50 mCi (p = 0.370). However, after combining both RAI groups, we did see a significant effect of cumulative RAI dose on AMH change over time (p = 0.019; Fig. 4). Further, we did not find a significant influence of RAI preparation method on AMH concentrations in the single RAI group. As only one patient in the multiple RAI group received her initial RAI therapy after rhTSH, we were unable to analyze the influence of RAI preparation method on AMH in the multiple RAI group.
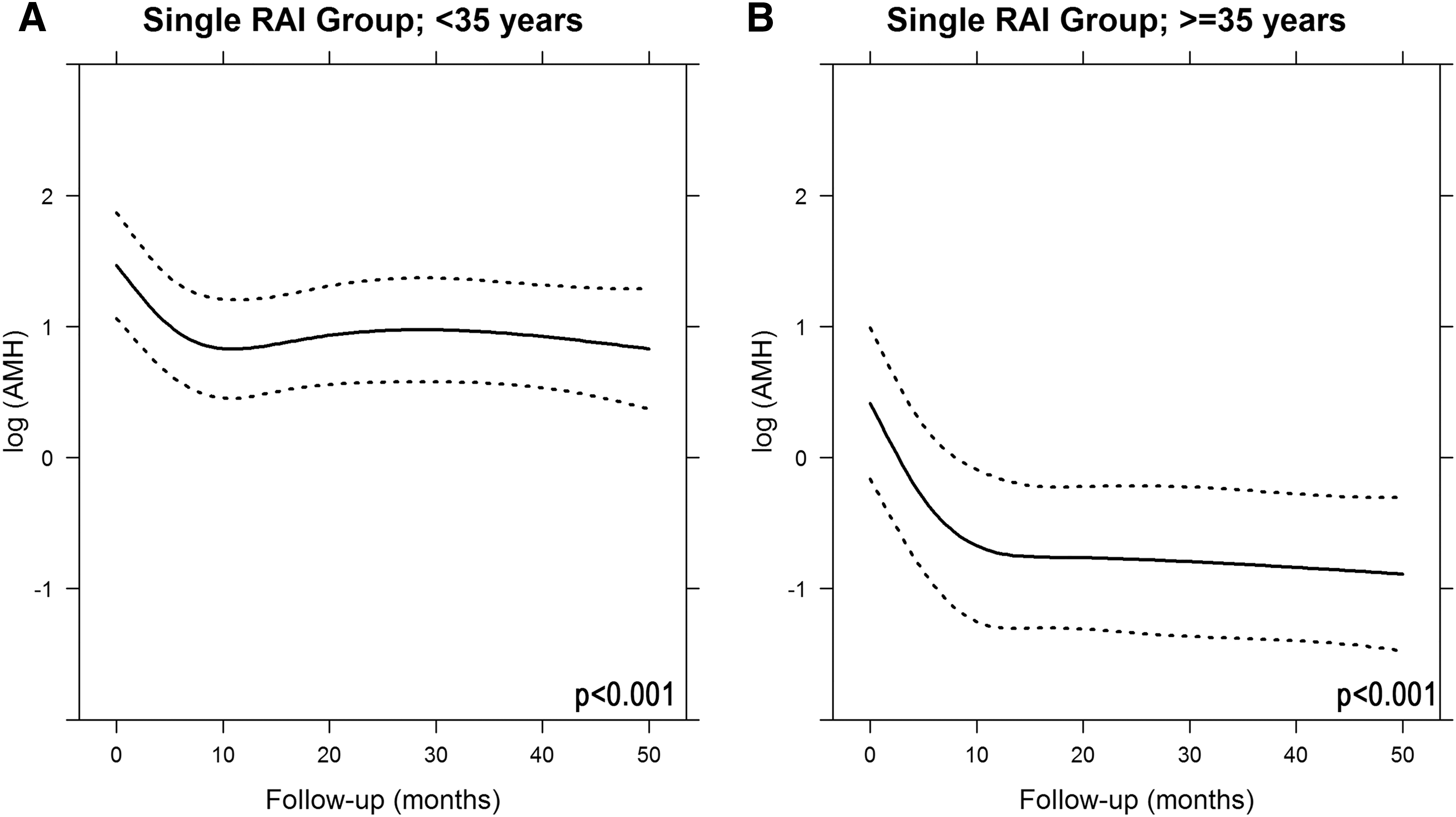
AMH concentrations over time for females (

AMH concentrations over time for females (
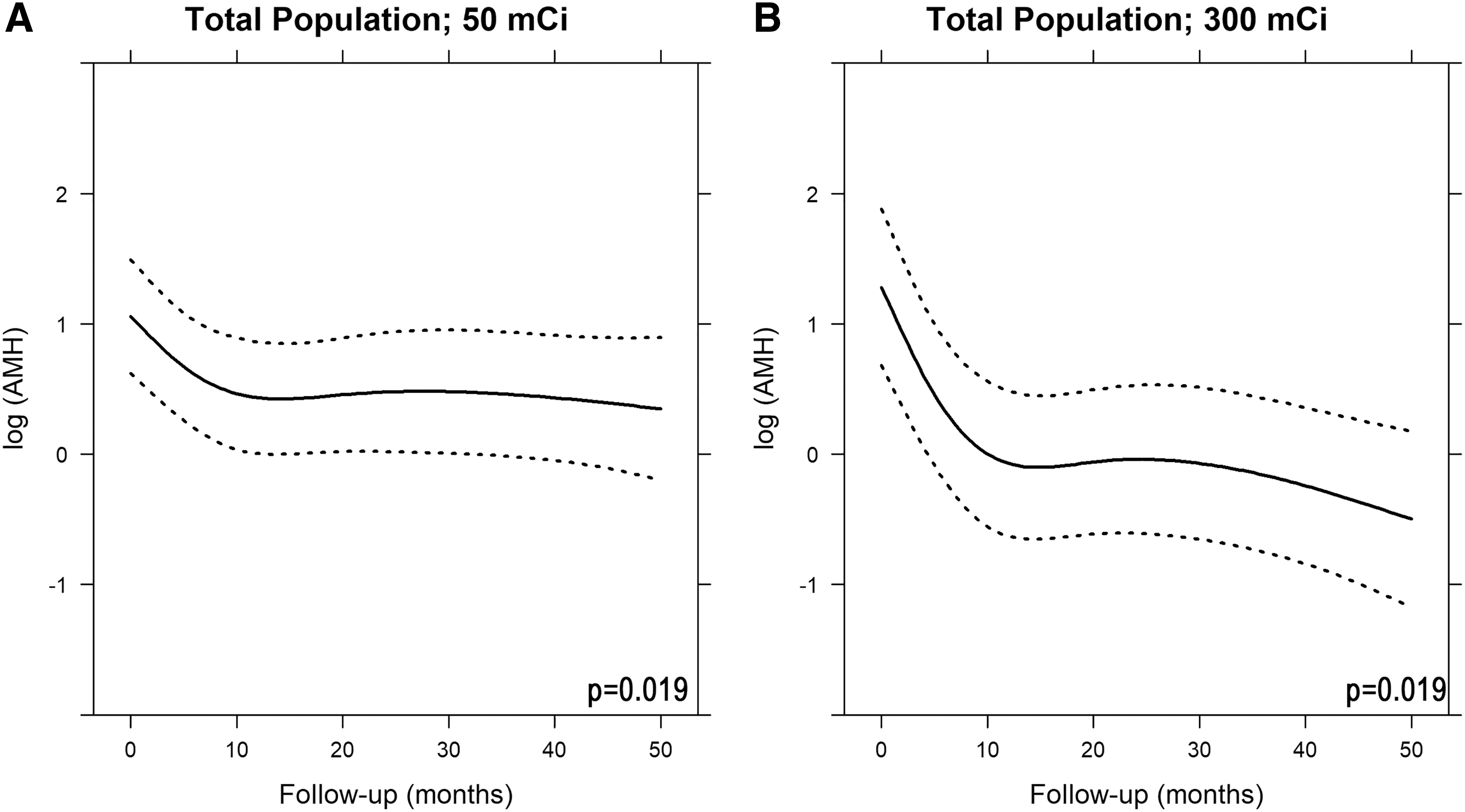
AMH concentrations over time for females receiving (
Desire to have a child and childbirth
Median time between first RAI therapy and end-of-follow-up was 43 months. During follow-up, seven children (11%) were born (Table 3); all children were born in patients younger than 35 years of age at diagnosis. Median time from initial RAI therapy to birth was 34 months. During follow-up, eight patients became menopausal; seven (88%) were older than 35 years of age at diagnosis.
Outcomes Related to Childbearing
Values are medians (25–75 IQR) or numbers (percentages).
Information missing in 13 subjects.
Information missing in seven subjects.
Information missing in six subjects.
IQR, interquartile range.
Fifty-two patients (80%) completed the questionnaire about the influence of the diagnosis and treatment of thyroid cancer on their desire to have a child. Of these patients, 16 (40%) in the single RAI and 4 (33%) in the multiple RAI group stated that their desire to have a child was, indeed, influenced by the diagnoses or treatment. In the majority of these patients, they were either not wanting a child anymore (40%), or the medicalization of an upcoming pregnancy (30%), whereas the rest had other reasons or did not specify them. There were more women in whom their desire to have a child was influenced in the below 35 than in the above 35 years of age group (47% vs. 19% respectively; p = 0.051).
Discussion
This study shows that in women with DTC, who were treated with total thyroidectomy followed by a single RAI therapy, AMH concentrations significantly dropped by 55% in the first year after initial therapy, and thereafter were more or less stable. In patients receiving multiple RAI therapies, after a short stabilization, a further decrease was seen (−85% after 48 month). Next to this, age significantly influenced AMH change over time, with a more pronounced decrease in AMH concentrations in women older than 35 years of age. Further, DTC diagnosis and treatment influences the desire to have a child in almost 40% of the patients.
We found a significant nonlinear change over time for both RAI groups. For the single RAI group, AMH concentrations significantly dropped by 55% during the first 12 months, and thereafter stabilized. In two earlier longitudinal studies with follow-up of 12 months, a significant decrease of AMH concentrations was also seen after initial RAI therapy (11,12); in these studies, AMH concentrations after 12 months were ∼30% and 58% lower than at baseline. The nadir in these studies was seen after three months. Thereafter, a slight recovery occurred, followed by stabilization. We did not have measurements that early after RAI therapy, and we were therefore unable to compare our results with these findings. However, one might argue that in these studies stabilization of AMH concentrations was already seen at 12 months, and, based on our results, one could speculate that thereafter AMH concentrations would remain stable. AMH concentrations later on were lower than at baseline, which is in line with the cross-sectional findings of Acibucu et al. showing significant decreased AMH concentrations compared with healthy controls (13). In the multiple RAI group, we also found a significant drop of AMH concentrations in the first year (−74%). This drop is followed by short stabilization, and thereafter a further decrease is seen. This latter decrease is most likely due to additional RAI therapy, but the decrease is less severe than the initial drop. This pattern might be caused by the fact that the patients received their therapies at different points in time (median time between first and second therapy was 9 months) and hence the expected step-wise decrease was not found, or oocytes of less quality were already damaged by the initial RAI therapy and those with better quality prevail. As we were the first to study women receiving multiple RAI therapies, we cannot compare our results with other studies, and further research is needed to confirm our findings.
We observed a significant influence of age on AMH change over time in both RAI groups; females younger than 35 years of age showed a less steep decrease than those older than 35 years. In correspondence with our results, two other longitudinal studies also showed a less steep decrease after RAI therapy in younger females (11,12). The steeper decrease of AMH concentrations in females older than 35 years compared with those younger than 35 years (−71% vs. −46% in the single RAI group) indicates that they might be more prone to become menopausal after receiving RAI therapy, taking into account that AMH concentrations are related to menopause (20,21). This steeper decline might be caused by their older oocytes of lesser quality, which are therefore more easily damaged by RAI therapy. In addition, in the single RAI group, baseline AMH concentrations were also already lower in females older than 35 years compared with those younger than 35 years. Further, although causality cannot be proven due to the lack of a control group, 88% of the patients who became menopausal after RAI therapy were older than 35 years of age at initial diagnosis. Therefore, these results suggest that clinicians should thoroughly balance the indication for RAI therapy in females older than 35 years of age with the desire to have a child.
We did not find an effect of cumulative RAI dose on AMH change over time in both RAI groups separately, which is in correspondence with earlier studies that did not show an effect of cumulative RAI dose on AMH (11,12,14). However, one might argue that there is, indeed, an effect of cumulative RAI dose in our study because (a) AMH concentrations after 48 months were significantly lower in the multiple RAI than in the single RAI group, and (b) combining both RAI groups we, indeed, found a significant effect of cumulative RAI dose on AMH change over time, suggesting that the cumulative RAI dose distribution in each RAI group separately is probably too small to find an effect.
DTC diagnosis and treatment influenced the desire to have a child in almost 40% of the patients included in this study. This high percentage reflects the struggles of patients after being diagnosed and treated for thyroid cancer, especially at a young age. Therefore, one might argue that this is one of the reasons that younger females showed lower quality of life in earlier studies (22,23). Carefully counseling these patients is, therefore, very important.
The main strength of this study, compared with previous studies, is the relatively large number of women with DTC who were studied prospectively. Further, the availability of follow-up AMH measurements with a median of almost three years positions our study, as far as we know, as the longest longitudinal study available. Besides, the use of marginal models for repeated measurement analysis allowed us to create a model for AMH change over time, thereby enabling the calculation of AMH at each moment in time. In addition, these models also enabled us to correct for missing AMH measurements. A possible limitation of the study might be the lack of a control group, and, therefore, one might argue that the discovered decline over time in our study reflects the biological decrease. However, both the stabilization one year after RAI therapy and the AMH decline in our study, which is far beyond the expected age-related decline (16), suggest causality. Further, it is important to note that AMH concentrations do not reflect the quality of the oocytes and, hence, diminished AMH concentrations do not necessarily mean reduced fertility (24), but undetectable concentrations are related to menopause (15). Although being the largest and longest prospective study available, the statistical power in the multiple RAI group might have been hampered due to the availability of only 18 patients. However, an indication of the effect of multiple RAI therapies on AMH concentrations can still be extracted from our results.
In conclusion, this study shows that in a population of female DTC patients treated with a single RAI therapy, AMH concentrations significantly dropped the first year after initial therapy by 55%. Thereafter, AMH concentrations remained stable but no recovery was seen. In patients receiving multiple RAI therapies, AMH concentrations decreased further after a short plateau phase. In addition, patients older than 35 years showed a much stronger decrease than those younger than 35 years. Finally, DTC diagnosis and treatment influenced the desire to have a child in almost 40% of the female patients. Therefore, clinicians should be aware of both the psychological and biological impact of DTC diagnosis and treatment on female patients in their reproductive years. Our results support a less aggressive treatment with RAI in low-risk patients as is advocated in the current ATA guidelines, especially in females older than 35 years of age with the desire to have a child.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.