
Abstract
Background:
Hyperthyroidism is associated with various cardiovascular risk factors. However, the relationship between hyperthyroidism and myocardial infarction (MI) or stroke has not been fully elucidated; only a few studies have investigated the association of hyperthyroidism with survival after MI or stroke.
Methods:
We included 59,021 hyperthyroid patients and a control cohort with 1,180,420 age- and sex-matched subjects from the Korean National Health Insurance database. Blood pressure, body mass index (BMI), glucose and cholesterol levels, and smoking history were obtained during National Health screening examination. We compared the incidence of MI, stroke, and survival after cardiovascular events between subjects with hyperthyroidism and the control cohort.
Results:
Subjects with hyperthyroidism had higher blood pressure, fasting glucose, and smoking rate, but lower cholesterol levels and a lower obesity rate compared with the control cohort. After adjusting these differences, as well as atrial fibrillation, hyperthyroidism was associated with increased risk of MI and ischemic stroke. Adjusted hazard ratios (HRs) for MI and ischemic stroke with hyperthyroidism was 1.16 [95% confidence interval, CI 1.03–1.30] and 1.12 [CI 1.04–1.20], respectively. In age-, sex-, and BMI-stratified analyses, an increased risk of MI and ischemic stroke remained significant in females, the older age group (≥50 years), and nonobese subjects (BMI <25 kg/m2), but not in males, the younger age group (<50 years), and obese subjects (BMI ≥25 kg/m2). The risk of hemorrhagic stroke was not different between subjects with hyperthyroidism and controls. Adjusted HRs for mortality in subjects with hyperthyroidism who developed MI, ischemic stroke, and hemorrhagic stroke were 1.11 ([CI 0.86–1.43], p = 0.44), 0.89 ([CI 0.75–1.05], p = 0.16), and 1.13 ([CI 0.88–1.47], p = 0.34), respectively.
Conclusions:
Hyperthyroidism is associated with increased risk of MI and ischemic stroke, independent of cardiovascular risk factors. This association is prominent in subjects with age ≥50 years, in females, and in the nonobese group. Hyperthyroidism did not significantly affect the mortality secondary to cardiovascular events.
Introduction
Hyperthyroidism is a common endocrine disorder with a prevalence of ∼0.3–0.5% in an iodine-replete area (1,2). Excessive amount of thyroid hormone has profound effects on the cardiovascular system (3). Hyperthyroidism is known to induce many effects on the cardiovascular system, such as increased heart rate, contractility, wide pulse pressure, systolic hypertension, changes in peripheral vascular resistance, predisposition to dysrhythmias, and especially atrial fibrillation (AF) (3,4). Many previous studies have also shown an increased all-cause mortality or cardiovascular mortality in hyperthyroid patients (5 –14), due to higher incidence of heart failure events (10,12 –14).
In addition to these well-known effects, there is increasing evidence that hyperthyroidism may accelerate atherosclerosis (15,16). Endothelial dysfunction, hypercoagulability, and thyroid autoimmunity have been suggested as potential contributors (16 –19). Recent study reported that thyroid hormone excess is associated with a procoagulant state, independent of conventional cardiovascular risk factors (16). Although hyperthyroidism has generally been shown to be associated with these various contributing factors, there are quite inconsistent results with respect to the association between hyperthyroidism and atherosclerotic cardiovascular events including myocardial infarction (MI) and ischemic stroke (12,13,15,20 –25). Furthermore, to the best of our knowledge, only a few studies have investigated the association between hyperthyroidism and survival after MI or stroke (26).
A notable limitation of previous epidemiological studies assessing the relationship between hyperthyroidism and MI or stroke is that they failed to appropriately adjust for individual cardiovascular risk factors (12,20,22,27,28). Moreover, only a few studies have considered smoking and body mass index (BMI) as confounding factors (15,21), although smoking is a risk factor for both hyperthyroidism and cardiovascular disease, and weight loss is a common presenting symptom of hyperthyroidism. Therefore, it is unclear whether the reported risks of cardiovascular morbidity and mortality in hyperthyroidism were attributable to thyroid hormone-mediated changes of cardiovascular risk profiles, confounding factors such as smoking and BMI, or excess of thyroid hormone itself.
As the Korean government operates a mandatory standardized health examination for all individuals older than 20 years, information about individual cardiovascular risk profiles can be obtained from the National Health Insurance (NHI) claims database (29). In the present study, we specifically investigated the incidence of atherosclerotic cardiovascular events including MI, stroke, and death after a cardiovascular event in hyperthyroid patients compared with age- and sex-matched control subjects.
Methods
Data source
This nationwide retrospective cohort study was based on the Korean NHI claims database. The NHI system covers more than 97% of the entire Korean population, and the database of the NHI includes all forms of medical service usage in Korea. The NHI database contains the following information: sociodemographic information of the beneficiaries; information about the diagnosis based on the International Classification of Diseases Tenth Revision (ICD-10) codes, all inpatient and outpatient claims data, primary and secondary diagnosis codes and treatments; and the National Health screening data (results of general health examinations and questionnaires on lifestyle and behavior) (29,30). The National Health screening data consisted of a health checkup database for the entire Korean population, via the NHI (31). Under the National Health screening effort, all insured adults are eligible to participate in the health screening program and are recommended to undergo standardized medical examinations every two years. It was known that about 70% of the entire cohort underwent a national health checkup. The death registration database of the Korean National Statistical Office is linked to the NHI database. For all-cause mortality, death certificates from the National Statistical Office were identified via individual identification numbers. This study was approved by the institutional review board of Myongji Hospital, and the requirement for informed consent was waived due to the retrospective nature of the study.
National Health screening examinations
The National Health screening examination of NHI was conducted through two stages (29). The first stage was a massive screening program to determine the presence of disease among the general population. The National Health screening data included medical interviews, physical examinations, regular blood and urine tests, chest X-ray examinations, and questionnaires that included information on the lifestyle, medical history, including smoking history. Blood samples for the measurement of serum glucose and lipid levels were drawn after overnight fasting. The second stage was a consultation for screening tests and a more detailed examination to confirm presence of disease(s). The NHI database contained only the first-stage screening data (29).
Study population
Hyperthyroid cohort
We extracted hyperthyroid patients diagnosed between January 2005 and December 2014 from the NHI database (Fig. 1). Hyperthyroid patients were defined as those who visited the clinic more than twice within the first year of diagnosis, with an ICD code of E050-059 and underwent thyroid function tests at the same time and those who visited the clinic more than once in the following year. Among these patients, subjects who underwent National Health screening examinations were included.
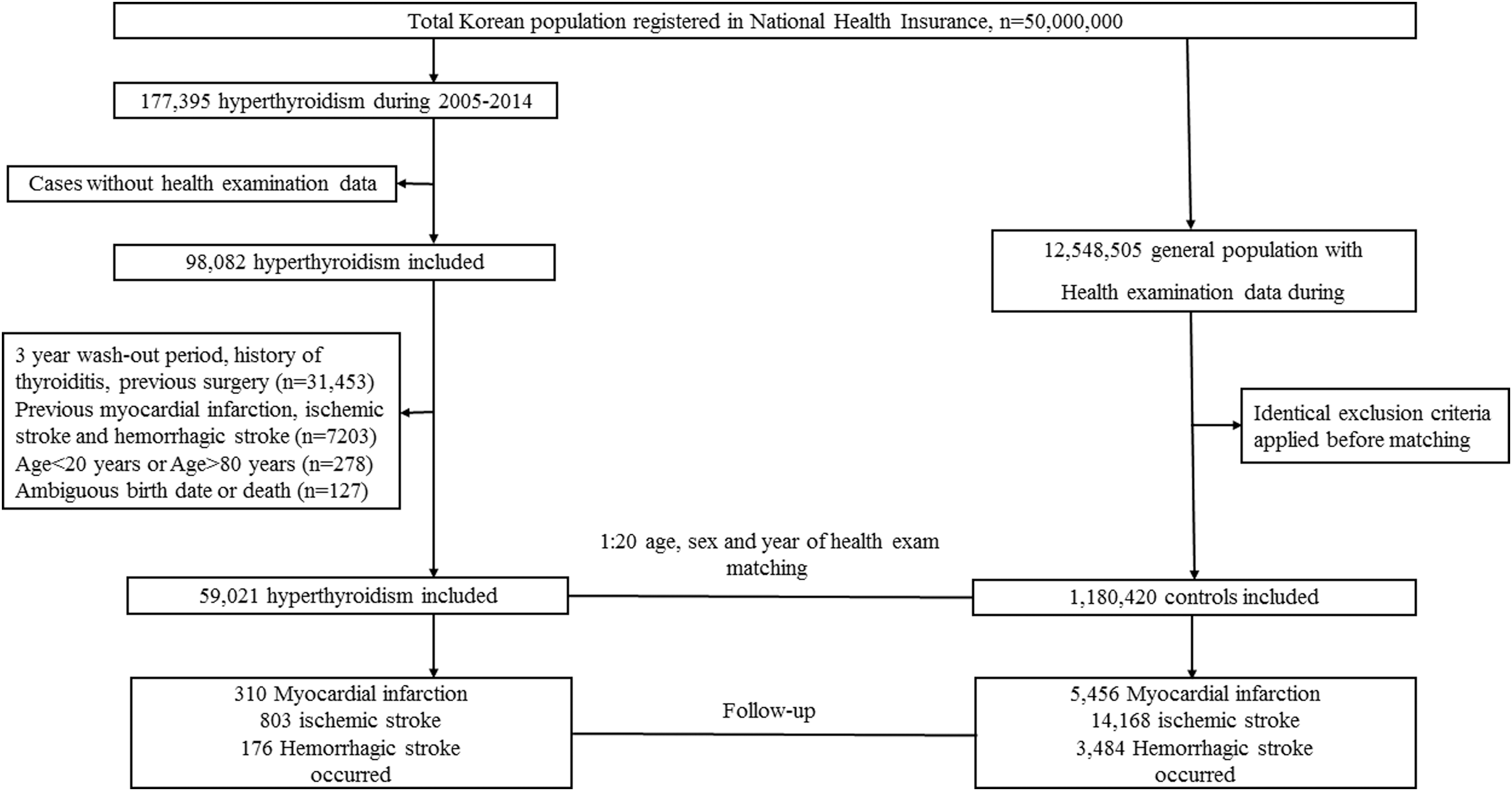
Flowchart of the study.
A three-year washout period was applied to define newly diagnosed cases of hyperthyroidism. The washout period was defined as the period between January 2002 and the timing of diagnosis of hyperthyroidism (the “index date”). The exclusion criteria were as follows: (i) those with thyroiditis (E06.0, E06.1) at any time to maximize specificity of diagnosis of hyperthyroidism; (ii) patients who underwent thyroid surgery to exclude any effects of iatrogenic thyrotoxicosis or postoperative hypothyroidism; (iii) patients who had previous MI or stroke; and (iv) patients who were aged <20 or ≥80 years.
Control cohort
The control cohort was also retrieved from the NHI database. For every patient with hyperthyroidism, 20 hyperthyroidism-free individuals on the “index date” were sampled from the general population, matched by birth year, sex, and year of National Health screening examination. The same exclusion criteria were applied before matching to the hyperthyroid cohort.
Cardiovascular risk profiles
Baseline cardiovascular risk profiles including blood pressure, fasting blood glucose, total cholesterol, BMI, and smoking status were obtained from National Health screening examination, which had been performed within three years before the diagnosis of hyperthyroidism. If the subjects underwent a health screening examination more than twice, the latest health screening examination data subsequent to the hyperthyroidism diagnosis were used. For the control cohort, baseline cardiovascular risk profiles were based on the National Health screening examination data, which were performed in the same year as in the subjects with hyperthyroidism.
Study outcomes
The primary outcomes for our study included the first occurrence of MI, ischemic stroke, and hemorrhagic stroke. MI, ischemic stroke, and hemorrhagic stroke were defined as inpatient hospitalization with the recording of ICD-10 codes of I21-I22, I63, and I60-I62, respectively, similar to previous studies (31,32). We also evaluated the mortality after each cardiovascular event and compared it between subjects with hyperthyroidism and controls.
Verification of the diagnosis
To identify patients with hyperthyroidism using the diagnosis code, we developed several case algorithms based on the number of visits to the clinic and the frequency of thyroid function tests performed for hyperthyroidism as the principal diagnosis (Supplementary Table S1). To assess the diagnostic accuracy, we performed medical chart reviews for hyperthyroid patients. We also retrieved the medical records of suspected nonhyperthyroidism patients to identify any misclassification bias. For suspected nonhyperthyroidism cases, we selected patients with nontoxic goiter, nontoxic thyroid nodules, and benign thyroid nodules. Two experienced endocrinologists reviewed the clinical data and biochemical results of the hyperthyroid and suspected nonhyperthyroid subjects. For each combination of algorithms, we determined the diagnostic accuracy, including sensitivity, specificity, positive predictive value, and negative predictive value from the hospital records and claims database. Our research team decided on an algorithm with the maximum sum of sensitivity and specificity to achieve an accurate diagnosis. In a validation study, we found that among the 160 hyperthyroidism patients who met the reference standard, 152 cases had been included in the claims data as hyperthyroidism with a sensitivity of 95%. We also found that among the 240 suspected nonhyperthyroidism cases, 22 were included as hyperthyroidism with a specificity of 91% in the claims data.
Statistical analyses
All variables are categorized and presented as frequencies and percentages. The chi-square test was used to compare the categorical variables of the hyperthyroid cohort and the control cohort. Crude incidence rates for MI, ischemic stroke, and hemorrhagic stroke were calculated as a number of each cardiovascular event per 1000 person-years. The incidence rates and incidence rate ratios were further analyzed by age (<50 and ≥50 years) and sex. Kaplan–Meier curves were used to describe the cumulative incidence of each cardiovascular event in the two cohorts. Follow-up started on the index date and was censored on the date of outcome occurrence, date of death, or last day of follow-up (December 31, 2017).
To examine the independent association between hyperthyroidism and risk of cardiovascular events, the Cox proportional hazard model was used, and hazard ratios (HRs) were computed with a 95% confidence interval [CI]. We conducted multivariable adjustment for age, sex, blood pressure, fasting blood glucose, total cholesterol, BMI, smoking status, and AF. We further stratified the analyses by age (<50 and ≥50 years), sex, BMI (<18.5 kg/m2, between 18.5 and 25 kg/m2, and ≥25 kg/m2), as well as smoking status.
We analyzed mortality in the subjects who developed MI, ischemic stroke, and hemorrhagic stroke. We compared the survival after each cardiovascular event between the hyperthyroid cohort and the control cohort. The follow-up started on the date of the diagnosis of cardiovascular disease onset and was censored on the date of death or the last day of follow-up (December 31, 2017). Kaplan–Meier curves were used to describe and compare the cumulative survival between the hyperthyroid and the control cohort. To evaluate the independent impact of hyperthyroidism on the mortality after MI or stroke, Cox regression analysis was performed adjusting for age, sex, Charlson comorbidity index, blood pressure, fasting blood glucose, total cholesterol, BMI, smoking status, and AF.
All statistical tests were evaluated using a two-tailed 95% CI; p < 0.05 was considered statistically significant. All statistical analyses were conducted using the statistical package SAS 9.1 (SAS Institute, Cary, NC).
Results
Baseline characteristics of the subjects
A total of 59,021 incidence cases of hyperthyroidism between January 2005 and December 2014 were included and analyzed. Baseline characteristics of the subjects are presented in Table 1. There were 62.2% females, and 46.1% of patients were older than 50 years at the time of diagnosis. There was a higher proportion of hyperthyroid patients with high blood pressure and hyperglycemia, compared with the age- and sex-matched control cohort. The smoking rate was also higher in the hyperthyroid cohort. In contrast, patients with hyperthyroidism had a lower frequency of obesity and hypercholesterolemia. In sex-stratified analysis, differences in the cardiovascular risk profiles were similar between male and female subjects. Compared with the control cohort, both male and female hyperthyroid patients had a higher proportion of high diastolic blood pressure, hyperglycemia, and higher smoking rates, but lower rates of obesity and hypercholesterolemia. Female hyperthyroid patients also showed higher systolic blood pressure than the control cohort.
Baseline Characteristics of the Study Population
BMI, body mass index; BP, blood pressure; FBG, fasting blood glucose.
Incidence rates of cardiovascular events
Cumulative incidence for each cardiovascular event is presented in Figure 2. Hyperthyroid patients had higher cumulative incidence of MI and ischemic stroke compared with the control subjects. There was a constant difference of cumulative incidence between the two groups. The number of events, incidence rates, and incidence rate ratios for cardiovascular events are shown in Table 2. During the follow-up period, a total of 5766 MI, 14,971 ischemic stroke, and 3659 hemorrhagic stroke events occurred. Among the hyperthyroid patients, 310 MI, 803 ischemic stroke, and 176 hemorrhagic stroke events developed. The incidence rates for MI, ischemic stroke, and hemorrhagic stroke was 0.72, 1.86, and 0.41 per 1000 person-years, respectively. Compared with the control group, hyperthyroid patients had an increased risk of MI and ischemic stroke. The incidence rate ratios for MI and ischemic stroke were 1.14 [CI 1.01–1.27] and 1.13 [CI 1.06–1.22], respectively, whereas the incidence rate of hemorrhagic stroke was not different between the two groups (incidence rate ratio 1.01 [CI 0.86–1.18]). When analyses were stratified by sex and age, the increased risk for MI and ischemic stroke in hyperthyroid patients was observed in females only. Age- (<50 and ≥50 years) and sex-stratified incidence curves are shown in Supplementary Figure S1.
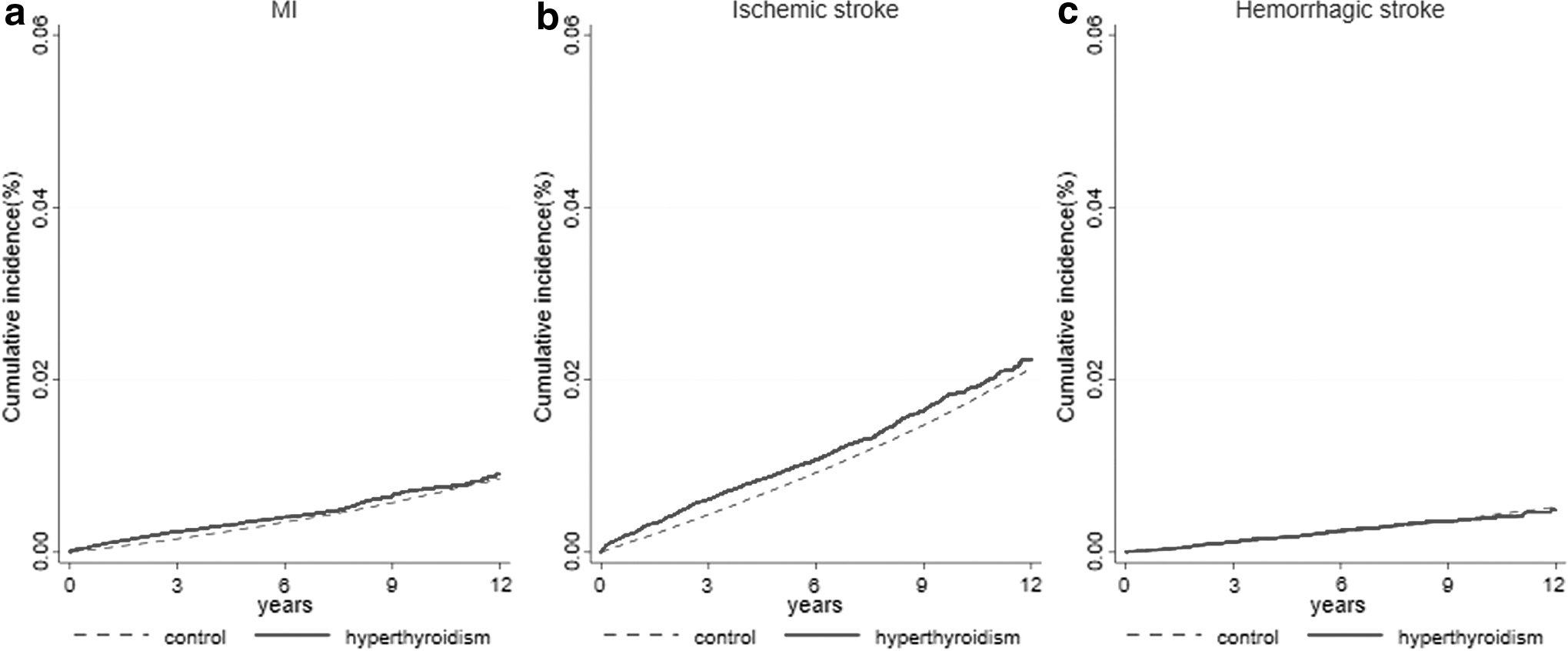
Kaplan–Meier curves for incidence of cardiovascular events in hyperthyroid patients and the control cohort. Kaplan–Meier curves for (
Incidence Rates of Cardiovascular Events in the Hyperthyroidism Cohort and the Control Cohort
CI, 95% confidence interval; IRR, incidence rate ratio; PYS, person-years.
Per 1000 person-years.
Risk factors for cardiovascular events by Cox proportional hazard model
The adjusted HRs for each cardiovascular event are presented in Table 3. After adjusting for various cardiovascular risk factors, hyperthyroidism was still an independent risk factor of MI and ischemic stroke (HR for MI: 1.16 [CI 1.03–1.30], p < 0.001, and HR for ischemic stroke: 1.12 [CI 1.04–1.20], p < 0.001, respectively). These adjusted HRs for MI and stroke were similar to the crude incidence rate ratio. The risk of hemorrhagic stroke was not different between the two groups (HR 0.99 [CI 0.85–1.15]). As expected, increasing age, male sex, higher blood pressure, hyperglycemia, high cholesterol level, obesity, and smoking were independently associated with MI and ischemic stroke.
Adjusted Risk for Each Cardiovascular Events by Cox Proportional Hazard Model
HR, hazard ratio.
Subgroup analyses for risk of each cardiovascular event in patients with hyperthyroidism
The subgroup analyses for each cardiovascular event are presented in Figure 3. The age- and sex-stratified analyses showed that hyperthyroidism increases the risk of MI and ischemic stroke only in subjects older than 50 years and in female subjects, independent of cardiovascular risk factors. In the stratified analysis by BMI category, independent association between hyperthyroidism and MI/ischemic stroke was generally observed in nonobese subjects (BMI <18.5 and 18.5–25 kg/m2), but not in obese subjects (BMI ≥25 kg/m2). The subgroup analysis of smoking status showed an independent relationship between MI and hyperthyroidism in the smokers, and an independent association between ischemic stroke and hyperthyroidism in the nonsmoker group. Hyperthyroidism was consistently not associated with risk of hemorrhagic stroke in stratified analysis.
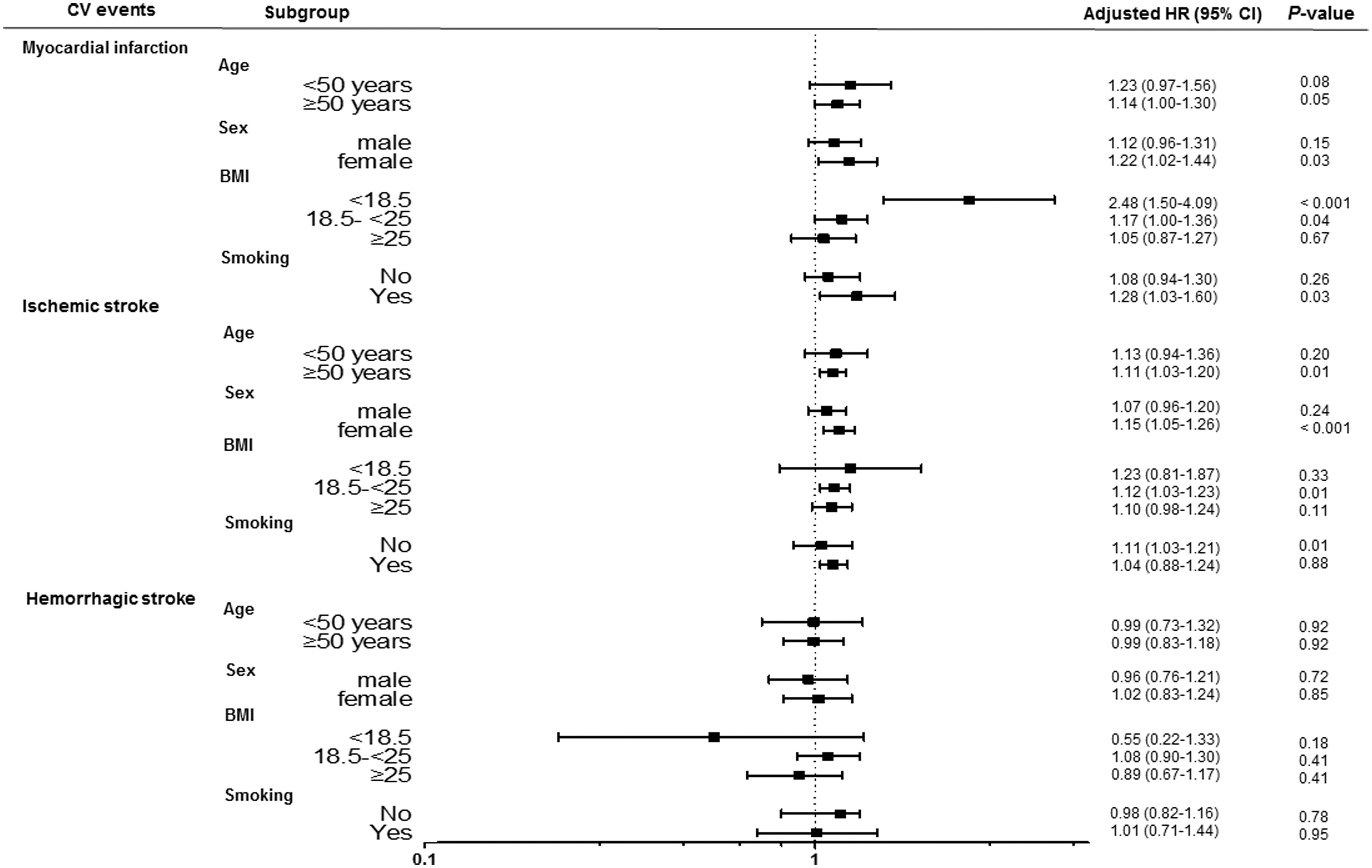
Subgroup analyses on each cardiovascular event stratified by age, sex, BMI, and smoking status. BMI, body mass index; CI, 95% confidence interval; CV, cardiovascular; HR, hazard ratio.
Survival after cardiovascular events between hyperthyroid patients and the control cohort
Cumulative survival after each cardiovascular event is shown in Figure 4. Among the subjects who experienced a cardiovascular event, the survival rate tended to decrease in the hyperthyroid cohort compared with the control cohort; however, this finding was not statistically significant. The 5-year survival rates in the hyperthyroid cohort with MI, ischemic stroke, and hemorrhagic stroke were 78%, 80%, and 58%, respectively, compared with 83%, 80%, and 67% in the control cohort.
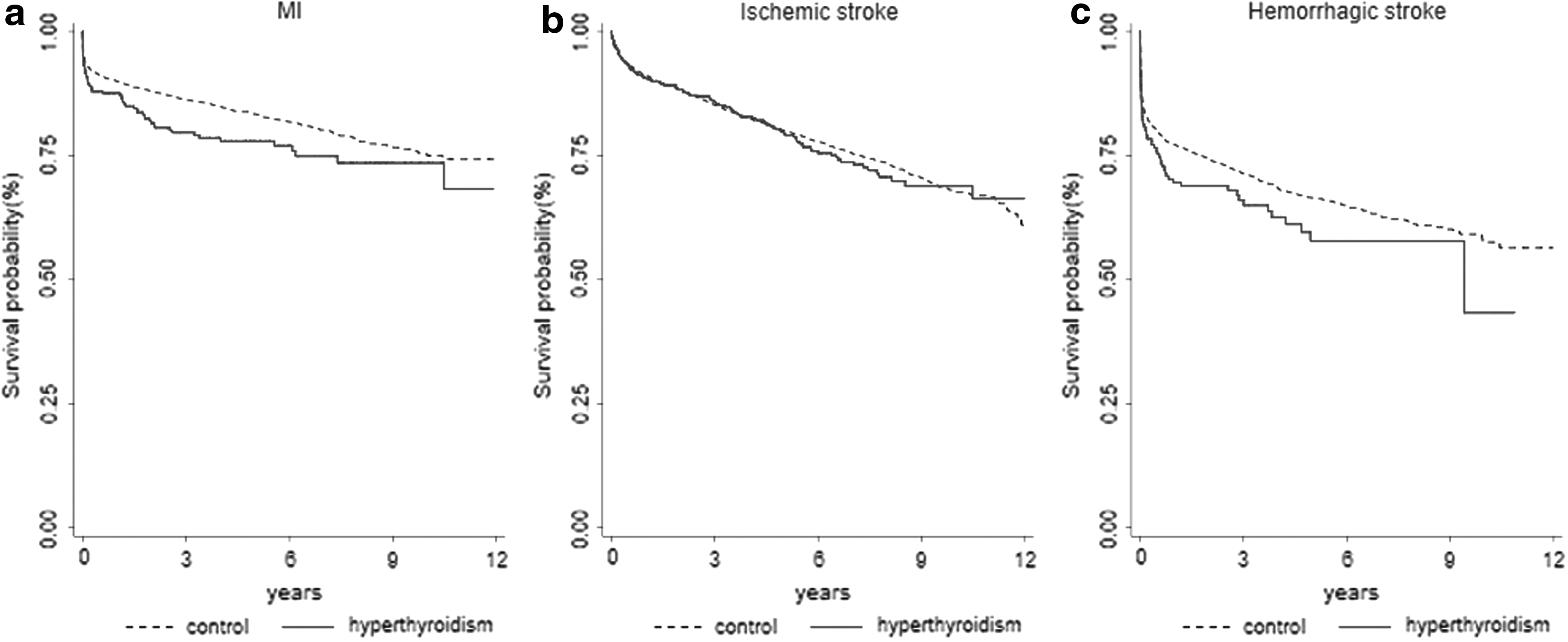
Kaplan–Meier curves for survival after each cardiovascular event between hyperthyroid patients and the control cohort. Kaplan–Meier curves for survival after (
The adjusted HRs for mortality after each cardiovascular event are presented in Supplementary Table S2. After adjusting for the Charlson comorbidity index and baseline cardiovascular risk profiles, HRs for mortality in hyperthyroid patients who developed MI, ischemic stroke, and hemorrhagic stroke were 1.11 ([CI 0.86–1.43], p = 0.44), 0.89 ([CI 0.75–1.05], p = 0.16), and 1.13 ([CI 0.88–1.47], p = 0.34), respectively.
Discussion
In this nationwide, large cohort study, we found that hyperthyroidism was associated with an increased risk of MI and ischemic stroke. The risk of hemorrhagic stroke was not different between patients with hyperthyroidism and controls. Furthermore, the increased risk of MI and ischemic stroke remained significant in females, older age group (≥50 years), and nonobese subjects (BMI <25 kg/m2), even after adjusting for the baseline cardiovascular risk profiles. We also found that hyperthyroid patients with MI or stroke tended to have decreased survival rates compared with the controls with MI or stroke, although this finding did not reach statistical significance.
Consistent with the findings presented here, some studies have found an association between hyperthyroidism and coronary heart disease or ischemic stroke (13,15,20,22), however, not all have done so (12,21,23,24). Possible reasons for this inconsistency may include heterogeneity between studies regarding the differences in design, characteristics of participants, control for comorbidities, and explored cardiovascular outcomes. It should be noted that important cardiovascular risk factors such as blood pressure and glucose or cholesterol levels were not properly adjusted in some studies (12,20,22,27). Moreover, potential confounding factors, such as BMI and smoking, were also not consistently controlled for (12,20,22). The present study adjusted for cardiovascular risk factors using individual laboratory and physical examination data instead of using ICD codes or comorbidity index, unlike previous register-based data (12,13,20). Using this valid method for the control of cardiovascular risk profiles, we found an increased risk of MI and ischemic stroke in hyperthyroid patients.
In this study, hyperthyroid patients, compared with controls, were found to have higher risk cardiovascular profiles in terms of systolic blood pressure, fasting blood sugar level, and smoking status, but lower frequency of obesity and hypercholesterolemia, similar to the findings of previous reports (3,33,34). After adjusting these differences, hyperthyroidism was consistently associated with increased risk of MI and ischemic stroke, but not associated with risk of hemorrhagic stroke, suggesting that hyperthyroidism is associated with atherosclerotic cardiovascular events. Recently, in the prospective Rotterdam study, free thyroxine levels were positively associated with atherosclerosis throughout the whole spectrum, from subclinical atherosclerosis to overt atherosclerotic events, including coronary disease and cerebrovascular events, independent of cardiovascular risk factors (15). Taken together with our study, these findings suggest that excessive thyroid hormone may itself contribute to the development of atherosclerosis.
Although the risk of cardiovascular disease in hyperthyroid patients may differ by age group and sex, not all studies performed stratified analyses (10,21). In line with some previous studies that found increased cardiovascular risk only in the elderly and female hyperthyroid patients (12,25), the findings reported here show an independent association between hyperthyroidism and MI as well as ischemic stroke, especially in patients aged ≥50 years and in females. In stratified analysis by BMI category and smoking status, an increased risk of MI and ischemic stroke was generally observed in nonobese (BMI <25kg/m2) hyperthyroid subjects and an increased risk of ischemic stroke in nonsmoker hyperthyroid subjects. Although this is not in itself evidence of a causal link, the results of these subgroup analyses suggest that hyperthyroidism significantly increases the risk of MI and/or ischemic stroke even in subjects with conventional low risk such as the nonobese or nonsmokers.
Among the various cardiovascular outcomes, the present study specifically investigated association between hyperthyroidism and MI/stroke. Because hyperthyroidism is associated with hyperdynamic circulation characterized by increased cardiac contractility and cardiac output, previous studies reported that risk of heart failure is increased in hyperthyroidism (1,12,13,25). However, heart failure is defined as a clinical syndrome, caused by structural or functional impairment of ventricular filling or ejection of blood, rather than distinct cardiovascular events (35). Furthermore, hyperthyroidism-induced heart failure can be caused by various contributing factors as well as by ischemic heart disease. Therefore, this study focused on the association between hyperthyroidism and distinct atherosclerotic cardiovascular events such as MI and stroke.
There are several possible mechanisms that could explain the increased risk of atherosclerotic events in hyperthyroid patients. First, thyroid hormone can increase indicators of endothelial damage by affecting endothelial function (16,17,36,37). Second, decreased fibrinolysis is commonly observed in hyperthyroidism (18). Third, it has been suggested that thyroid autoimmunity contributes to increased atherosclerosis (19). It has been speculated that thyroid autoantibodies may be associated with atherosclerotic plaque development and rupture (19). In our study, hyperthyroid patients had a higher cumulative incidence of MI and ischemic stroke compared with controls, and the difference in the cumulative incidence remained constant over the years. Because autoimmune hyperthyroidism accounts for more than 95% of hyperthyroidism in Korea, and since most hyperthyroid patients receive treatment, this finding suggests that thyroid autoimmunity may play a role in the development of atherosclerosis, despite recovery of an euthyroid status.
Previous studies have reported increased cardiovascular mortality (5 –7,38), although there are some exceptions (27). However, only a few studies have reported an association between hyperthyroidism and death after a cardiovascular event (26). Our study shows that among subjects who experienced cardiovascular events, mortality tended to increase in hyperthyroid patients compared with controls, although this finding did not reach statistical significance. The authors of several reports hypothesized that elevated thyroxine levels stiffen the arterial walls, thereby decreasing the reactivity of the vessels to the changes in blood flow (39). Beyer et al. have shown that hyperthyroid patients were more likely to have high-grade coronary stenosis and high-risk plaque features compared with euthyroid patients (40). Considering that hyperthyroid patients are more likely to receive treatment for cardiovascular risk factors during the follow-up period, which could eventually reduce their risk for cardiovascular mortality compared with the control subjects, the tendency of an increased death rate in hyperthyroid patients suggests that hyperthyroidism may be an important prognostic factor in patients with cardiovascular events.
Our study has several limitations. First, the diagnosis of hyperthyroidism relied on the administrative claims data, reported by physicians or hospitals, similar to other registry-based studies. However, to maximize the diagnostic accuracy, we developed case algorithms based on the number of hospital visits and thyroid function tests, and selected a combination of algorithms that offer sensitivity and specificity of greater than 90%. Second, the present study lacks information about the etiology of hyperthyroidism. However, Korea is known to be an area of excessive iodine intake (41) and Graves' disease is the most prevalent cause of hyperthyroidism in iodine-sufficient areas (42). Toxic adenomas account for less than 1% of hyperthyroidism in Korea (43). Thus, the results of this study may be interpreted as the influence of Graves' disease on the risk of cardiovascular disease. Third, this study lacks information on the treatment modality for hyperthyroidism and biochemical thyroid function tests. Previous studies reported increased cardiovascular morbidity and mortality after radioiodine treatment in hyperthyroid patients (5,6,10,38). However, in Korea, 97% of hyperthyroid patients have been treated with antithyroid drugs as first-line treatment over the past few decades and primary radioiodine therapy remains restricted to patients who relapse after anti-thyroid drugs (43,44). Therefore, the potential effects of radioactive iodine on the results of our study are likely minimal. Recently, studies suggested that early and effective control of hyperthyroidism is a more important factor determining cardiovascular risk than the treatment modality (13,25). However, it was not possible to determine whether increased risk of MI/stroke was due to duration of incomplete biochemical control of hyperthyroidism in the current study.
In conclusion, hyperthyroidism appears to be associated with increased risk of atherosclerotic cardiovascular events such as MI and ischemic stroke, independent of conventional cardiovascular risk factors. This association is prominent in subjects with age ≥50 years, in females, and in the nonobese group. This study shows that hyperthyroid patients with cardiovascular events tend to have decreased survival rates compared with the control subjects, although this finding was not statistically significant. More careful management strategies for cardiovascular disease are warranted in hyperthyroid patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2