
Abstract
Background:
An important side effect of radioactive iodine (RAI) therapy in patients treated for papillary thyroid cancer (PTC) is chronic sialadenitis. Neck ultrasonography (US) easily recognizes radioiodine-induced salivary gland abnormalities. The objectives of this study were to determine the prevalence of US-detected sialadenitis caused by RAI and to identify the risk factors associated with this damage.
Methods:
This nonconcurrent cohort study includes all PTC-operated patients who were treated with RAI between 2007 and 2017 and were systematically evaluated with preoperative and follow-up neck US that included targeted exploration of the major salivary glands. Patients with pre-existing salivary gland diseases were excluded. The anatomical damage (diminished glandular volume, wavy contours, hypoechogenicity, and heterogeneity) was qualitatively assessed and compared with the preoperative study. RAI activity, sex, age, and preparation method were evaluated as risk factors using univariate and multivariate analyses with logistic regression.
Results:
Enrolled in this study were 570 patients who received a median RAI activity of 3700 MBq (100 mCi). On US, we found 143 patients (25.1%) with damage in at least one of their salivary glands: all had parotid damage (77 bilaterally) and 14 (9.8%) also had submandibular gland damage (7 of them bilaterally). The multivariate analysis indicated that the risk of sialadenitis was significantly (p < 0.01) correlated with both RAI activity and sex (14.1% of males vs. 28.5% of females). However, the main risk factor was RAI activity; no injury was detected in 156 patients who received 1110 MBq (30 mCi) and 1850 MBq (50 mCi) of RAI. In the groups of patients receiving 3700 MBq (100 mCi), 5550 MBq (150 mCi) and ≥7400 MBq (≥200 mCi), atrophy was found in 21%, 46.9%, and 77.7% of patients, respectively. Age and preparation method were not related to an increased risk of atrophy in this study.
Conclusions:
Chronic sialadenitis is common and affects approximately one fourth of patients who receive 3700 MBq (100 mCi) or higher RAI activity. The main risk factor for this injury is the total RAI activity administered. By using the lowest effective activity possible, irreversible anatomical damage in salivary glands can be minimized. US is an excellent tool to diagnose post-RAI atrophy.
Introduction
Papillary thyroid cancer (PTC) accounts for ∼85% of differentiated thyroid cancer cases (1). Since 1940, radioactive iodine (RAI) has been used very widely as an adjunct treatment for PTC patients who have undergone surgery (2). Until the year 2000, most patients with PTC received postoperative RAI. The most commonly administered activity is 3700 MBq (100 mCi) for remnant ablation, and even greater activities are being used for higher risk patients: 5550 MBq (150 mCi) for locoregional nodal disease and 6475–7400 MBq (175–200 mCi) for distant metastases (3).
It has been reported for the past 30 years that RAI is not completely innocuous. Organ-specific side effects such as damage to bone marrow, gonads, bladder, and lacrimal glands have been detected (4 –7). Salivary glands are most commonly affected (7 –10). Their functional alterations have been studied in-depth with scintigraphy (11 –13), but few studies detail the contribution of radiological images such as ultrasonography (US) or computed tomography (CT) to quantify anatomical post-RAI damage (14 –18).
In our practice, we systematically use US for staging before thyroidectomies and for follow-up in patients treated for malignant thyroid diseases. Targeted exploration of the major salivary glands is an essential part of these screenings. Based on our experience, alterations in the major salivary glands are frequently identified by US in patients who received higher activities of RAI. However, this association remains underestimated and underrecognized by many clinicians.
The objectives of this study were to determine the prevalence of US-detected RAI-induced salivary gland damage in patients treated for PTC and to identify risk factors associated with this damage and assess the clinical repercussions on the patient's quality of life. In addition, we evaluated the effects of management modifications introduced in the last decade based on the results of this work on the prevalence of such damage.
Materials and Methods
Design
This is a nonconcurrent cohort study approved by our institutional ethics review board, and a waiver for informed consent was obtained.
Patients
We enrolled all PTC-operated patients who received RAI treatment and were referred to our Radiology Department for a follow-up US between January 2007 and December 2017. Inclusion criteria were presurgery US neck examination and follow-up US (at least 12 months after receiving RAI), both performed in our institution, including targeted US evaluation of major salivary glands with images and radiological reports available in PACS (Picture Archiving and Communication System). We excluded patients with pre-existing salivary diseases (e.g., hypoplasia, agenesis, sialolithiasis, Sjögren syndrome, external radiation therapy of the neck, and previous salivary gland surgery due to a benign or malignant pathology).
US examination
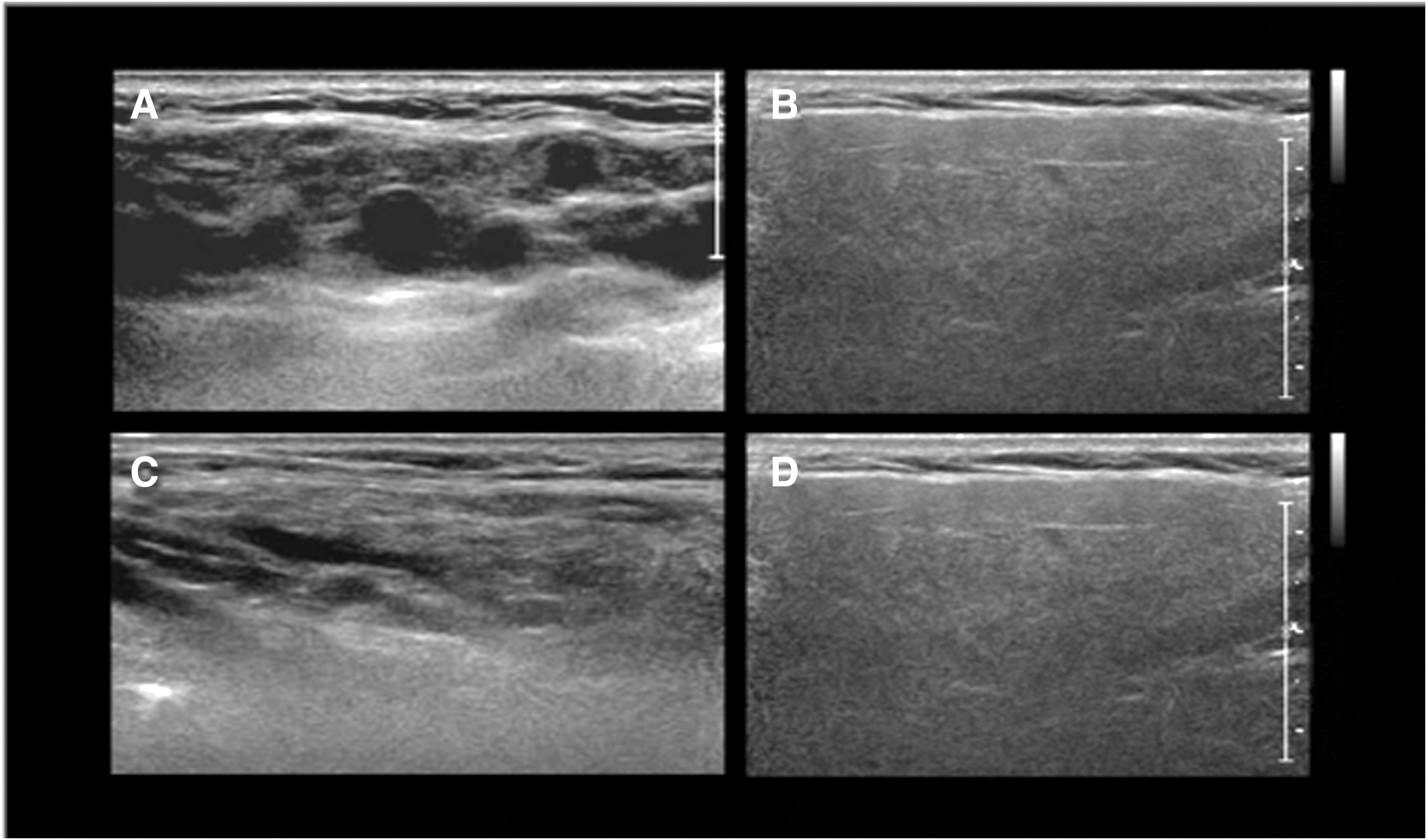
The primary endpoint of this study was salivary damage detected by US. These examinations were performed by four specialized radiologists (E.H., C.W., J.P.N., and P.G.) who work in a multidisciplinary environment in our institution's Thyroid Center. Each radiologist has more than 15 years of experience in thyroid US. IU22 Gemini and Epiq7G equipment (Philips Healthcare) with 5–12, 5–17, and 5–18 MHz transducers and color Doppler mode were used. The morphological characteristics observed in each case were as follows: size (normal or diminished), echogenicity (hyper- or hypoechogenicity), sonographic pattern (homogeneous or heterogeneous), and contours (smooth or wavy). The parotid and submandibular glands were considered undamaged when they appeared symmetrical, normal in size, with smooth contours, homogeneous in structure, with hyperechogenic appearance compared with subcutaneous tissue and adjacent muscles, and with no dilation of the excretory systems (Fig. 1).

US of the main salivary glands before RAI treatment (
The features that define post-RAI treatment anatomical damage are the coexistence of decreased glandular size, lobulated margins, hypoechogenic pattern, and coarse echotexture, all findings reported in the literature (14 –16). The severity of these alterations in the four major salivary glands was not quantified, only visually evaluated as normal or damaged, comparing pre- and post-RAI sonograms and/or the damaged gland with the contralateral undamaged gland (Fig. 2). It is our standard practice to include the major salivary glands in all cervical (and thyroid) ultrasound examinations and to describe their normality or abnormality in the corresponding ultrasonographic reports.
Damaged, atrophic parotid glands (
Inter-reader agreement
A retrospective review of the anonymized US images of the first 139 patients' salivary glands was performed by a blinded radiologist (C.W.), who evaluated the consistency of her findings with the original sonographic reports. When discrepancies were found, the opinion of a third specialist (J.P.N.) was required to reach a consensus.
RAI preparation method
RAI was administered using traditional thyroid hormone withdrawal (THW) or recombinant human thyrotropin (rhTSH). The type of preparation method used depended on the patient's financial situation, as rhTSH is costly and not covered by health insurance in our country. According to the hypothyroidism protocol, levothyroxine was withdrawn 3–4 weeks before ablation (up to >30 UI TSH levels). The rhTSH group received an intramuscular dose of 0.9 mg of rhTSH (Thyrogen; Genzyme Corp.) on days 1 and 2, with RAI administered on day 3. Patients were prescribed a low-iodine diet for 2 weeks before RAI treatment and were instructed to drink abundant liquids and suck on sour candy for 24–48 hours, starting 24 hours after receiving RAI. In this study, we did not evaluate the effects of sialagogues.
RAI activity
The RAI activity was prescribed on a case-by-case basis for each patient according to their risk for persistent or recurrent disease and postoperative evaluation with thyroglobulin (Tg), Tg antibodies, and neck US (6–24 weeks after surgery). In this work, patients were divided into five groups depending on the total RAI activity received: Group A, 1110 MBq (30 mCi); Group B, 1850 MBq (50 mCi); Group C, 3700 MBq (100 mCi); Group D, 5550 MBq (150 mCi); and Group E, ≥7400 MBq (≥200 mCi). Given that the actual activity administered is often not exact, Group A includes patients who received RAI activity of 1110–1295 MBq (30–35 mCi); Group B, 1776–2146 MBq (48–58 mCi); Group C, 3663–4070 MBq (99–110 mCi); Group D, 5550–5920 MBq (150–160 mCi); and Group E, 7400–18,500 MBq (200–500 mCi).
Evaluation of salivary gland symptoms
For 6 months during 2012, 54 consecutive patients voluntarily filled out a locally created, self-administered questionnaire regarding symptoms of the salivary and lacrimal glands. This subgroup of patients provided a written and informed consent to participate in this survey. They were asked about changes they might have experienced immediately or gradually after RAI, such as alteration of taste, painful swelling of the parotid gland, chronic mouth dryness, and lacrimal problems. They rated the degree to which their quality of life had changed after RAI on a scale from 1 to 4 (no change, mild, moderate, or severe). The questionnaire was given only to this subset of patients and only once (at the time of their follow-up US examination). The rest of the patients included in this study were not surveyed.
Statistical analyses
Continuous variables with normal distribution are presented as mean ± standard deviation (SD). Continuous variables with skewed distribution are presented as medians with 25th and 75th percentiles (interquartile range [IQR]). Categorical variables are presented as numbers and percentages. Group differences were tested using the analysis of variance (ANOVA) test, the Pearson chi-square, or the Fisher exact test where appropriate. Univariate and multivariate analyses with logistic regression were performed using US gland damage as a dependent variable and RAI activity, sex, age, and preparation method as independent variables. Inter-reader agreement was determined by kappa coefficients for pairwise comparisons. Agreement was defined as poor (0.20), fair (0.21–0.40), moderate (0.41–0.60), good (0.61–0.80), or excellent (0.81–1.00). Statistical significance was defined as p-values of <0.05. Analyses were performed using STATA version 14 (STATA Corp., USA).
Results
Complete medical records from 2007 to 2017 were available for 1912 PTC-operated patients, of which 667 (34.9%) received RAI. We excluded 97 patients whose presurgery US examinations were performed in other institutions, for whom less than 12 months had passed since receiving RAI or had pre-existing salivary gland abnormalities. In total, 570 patients (435 [76.3%] female) with a median age of 43 years (range 13–82 years, IQR 15–76) met the inclusion criteria. Table 1 shows their clinical characteristics.
Clinical Features of 570 Papillary Thyroid Carcinoma-Operated Patients with Subsequent Radioactive Iodine Treatment
IQR, interquartile range; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; rhTSH, recombinant human thyrotropin; THW, thyroid hormone withdrawal.
Among those who received RAI, 25.1% (143/570) had salivary gland abnormalities on US: all suffered damage to the parotid glands and 77 (53.8%) of them had bilateral atrophy. Fourteen (9.8%) subjects had additional atrophy to the submandibular gland, seven of them bilaterally.
Risk of salivary gland abnormalities on US was significantly associated with RAI activity and sex in both univariate and multivariate analyses (Tables 2 and 3). However, the main risk factor for anatomical abnormalities was RAI activity: no injury was detected in 156 patients (77 in Group A and 79 in Group B) who received RAI activities between 110 and 2146 MBq (30 and 58 mCi). The risk of damage increased with higher activities: it was found in 21.0%, 46.9%, and 77.8% of patients in Groups C, D, and E, respectively (Fig. 3). Regarding sex, 19/135 (14.1%) males and 124/435 (28.5%) females had atrophy in at least one of the salivary glands (p < 0.01).
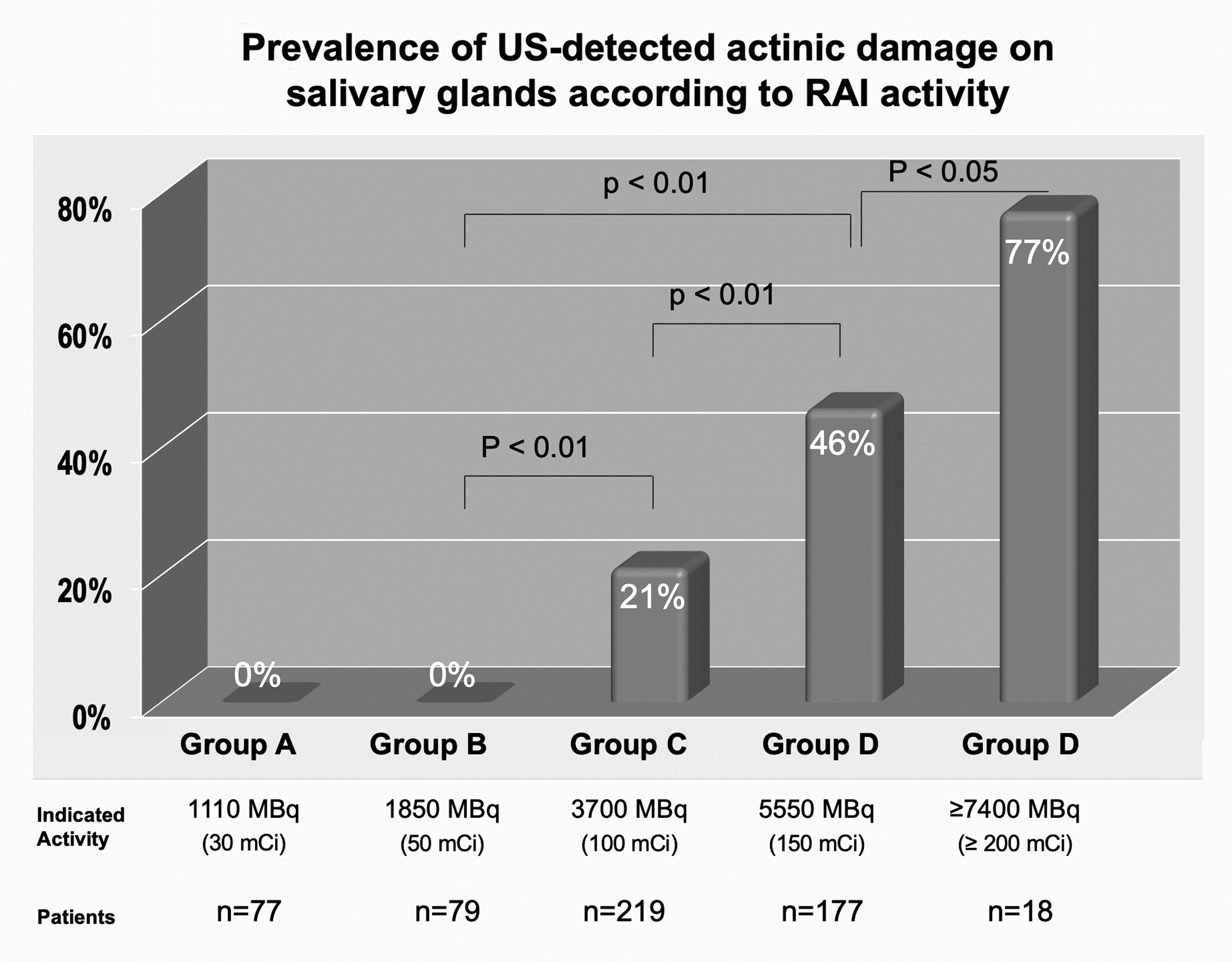
This graphic shows the prevalence of RAI-induced salivary gland damage in 570 patients, which depends on the total RAI activity received. There was no RAI-induced damage in the 1110 MBq (30 mCi) and 1850 MBq (50 mCi) groups. There is a clear, activity-dependent risk of damage, reaching up to 77% in patients with doses ≥7400 MBq (≥200 mCi).
Univariate Analysis for Risk of Salivary Gland Damage on Ultrasonography in 570 Papillary Thyroid Cancer-Operated Patients Treated with Radioactive Iodine
Multivariate Analysis for Risk of Salivary Gland Damage on Ultrasonography in 570 Papillary Thyroid Cancer-Operated Patients Who Received Radioactive Iodine Treatment
CI, 95% confidence interval.
The preparation method was THW in 425 (74.6%) patients and rhTSH in the remaining 145 (25.4%). Of the patients prepared with THW, 27.2% had damage, and of those prepared with rhTSH, 18.6%, a statistically significant difference (p = 0.037) in the univariate analysis (Table 2), but not in the multivariate analysis (p = 0.66) (Table 3).
Age was not related to an increased risk of atrophy (p = 0.42). By age group, percentages of atrophy were: <20 years = 17 (3%); 20–39 years = 223 (39.2%); 40–59 years = 275 (48.2%); and >60 years = 55 (9.6%).
Each patient had between 1 and 11 follow-up US during a median of 49 months (range 12–120 months). We found that US images did not change significantly over time after the first year.
Patient survey
As previously stated, during 6 months in 2012, a subgroup of 54 consecutive patients (44 [81.5%] female), with a mean age of 42.8 years (SD 13), 12–60 follow-up months after RAI treatment, and a mean RAI activity of 5298 MBq, SD 2671 (143.2 mCi, SD 72.25), voluntarily answered a self-administered questionnaire regarding their quality of life after RAI. Nineteen (35%) patients mentioned transitory taste alterations, 20 (37%) noted a painful parotid volume increase in the weeks or months following RAI, 9 (16%) experienced deglutition disorders, and 8 (15%) had lacrimal production symptoms (only 1 needed surgery for lacrimal duct obstruction). Regarding US alteration in these 54 patients who answered the survey, 23 (42.5%) had atrophy in at least one of their major glands, and of these 23 patients, 14 suffered bilateral atrophy. Sixteen of these patients with atrophy (16/23 [69.6%]) reported discomfort (2 with unilateral and 14 with bilateral atrophies). Specifically, 2/7 (28.5%) with unilateral US salivary gland damage and 14/14 (100%) with bilateral damage presented salivary symptoms. All 14 patients with bilateral US salivary gland damage stated that after receiving RAI their quality of life deteriorated to some degree (mild or moderate).
Reader agreement
One hundred thirty-nine patient images, stratified by age and sex, were randomly selected for an inter-reader agreement assessment. The kappa value was 0.91 [95% confidence interval, CI, 0.84–0.99] for chronic sialadenitis on submandibular glands and 0.93 [CI 0.86–1.00] for parotid gland damage.
Discussion
Since 1940, RAI has been used as an adjuvant therapy in patients operated on for papillary and follicular cancers. However, from the 1980s onward, the awareness for multiple adverse effects, some of them harmful, has increased; the effects on the salivary glands are particularly prevalent and can affect ∼25% of treated patients (4). Despite these findings, these effects are poorly understood and clearly underestimated in clinical practice.
Our results, as reported in the literature (14 –16,19), state that chronic sialadenitis correlates with the RAI activity received. In this study, the side effects on the salivary glands were found to be directly proportional to the total RAI activity administered (a greater activity is associated with greater damage: 21%, 46.9%, and 77.8% [p < 0.01] with RAI activity in the groups that received 3700, 5550, and ≥7400 MBq [100, 150, and ≥200 mCi], respectively) (Fig. 4). None of the patients (n = 156) who received a low activity (Groups A and B) presented alterations in their major salivary glands on follow-up US performed after 12–120 months (Table 2).
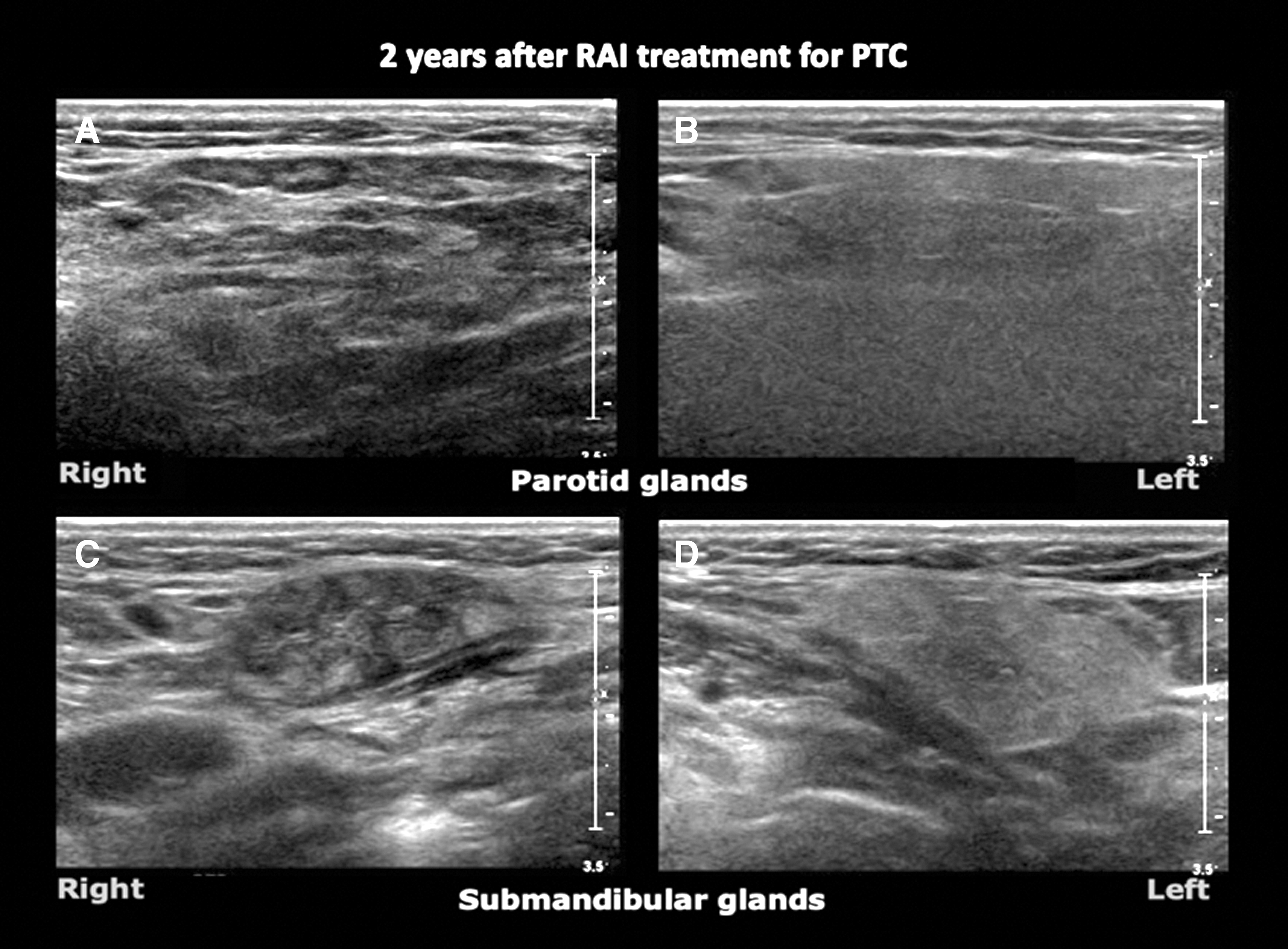
US of the major salivary glands in this PTC-operated 51-year-old patient, 2 years after 5550 MBq (150 mCi) of RAI treatment. Due to a high RAI activity, both the right parotid and right submandibular glands suffered actinic damage (
We have found that in addition to activity, age, sex, and method of preparation, there could also be other potential risk factors. However, in this study, only sex showed a statistically significant difference (p < 0.01): 19 of 135 males (14.1%) and 124 of 435 females (28.5%) had atrophy in at least one of the salivary glands. Age does not appear as an independent risk factor (possibly due to the small number of young patients) (Table 2).
Regarding the preparation method, it is known that the use of rhTSH increases the local concentration of RAI in the remnant thyroid tissue, thus increasing the treatment's efficacy even with lower activities. However, it significantly reduces the whole-body effective half-life of RAI (20). This faster clearance is expected to also reduce the exposure of the salivary glands and could lead to the reduction of their potential damage. Rosario et al. (21) found a lesser incidence of sialadenitis with the use of rhTSH compared with THW (36.6% vs. 80%). We have recently initiated the use of rhTSH and have limited experience: 74.6% of our patients were prepared with hypothyroidism and 25.4% with rhTSH. We also found chronic sialadenitis in 27.2% of the THW group versus 18.6% with rhTSH (p < 0.037) (Table 2). Nonetheless, this result could be distorted as the implementation of rhTSH coincides with the use of lower activities over the years. In fact, when performing a multivariate analysis including RAI activity, statistical significance disappears (Table 3).
As a result of this study and the increasing evidence of similar benefits with low RAI activities and/or no RAI treatment in low-risk patients, we have modified the existing recommendations in our Thyroid Center and prepared new local guidelines to diminish possible damage to major salivary glands. These guidelines include explicit instructions to patients who will receive RAI on the importance of maintaining adequate hydration and permanent stimulation of salivary secretions with lemon juice, candy, or gum. However, according to the literature, these precautions are not completely effective (22). We warn these patients treated with RAI of the possible painful increase of their parotid volume in the following months and advise them that no additional diagnostic tests are required. Finally, we limited the prescription of RAI to patients who are expected to have a clinical benefit by administering the lowest possible effective activity (1110–1850 MBq vs. 3700 MBq [30–50 mCi vs.100 mCi]), and we have ceased to administer RAI after each reoperation and carefully calculated activity in children. Since 2015, we have followed the guidelines of the American Thyroid Association (ATA) for the use of RAI (23).
Figure 5 summarizes these changes: the number of PTC surgeries has increased in our center over the past 11 years because of an increase in referrals, but the number of patients receiving RAI has diminished. The median activity administered has also decreased since 2010. As a consequence, damage to the major salivary glands has significantly decreased from 50% (2008) to 13% (2015). Since 2016, we have detected no new cases of post-RAI atrophy, although not all patients had complied with their annual checkup upon completion of this article.
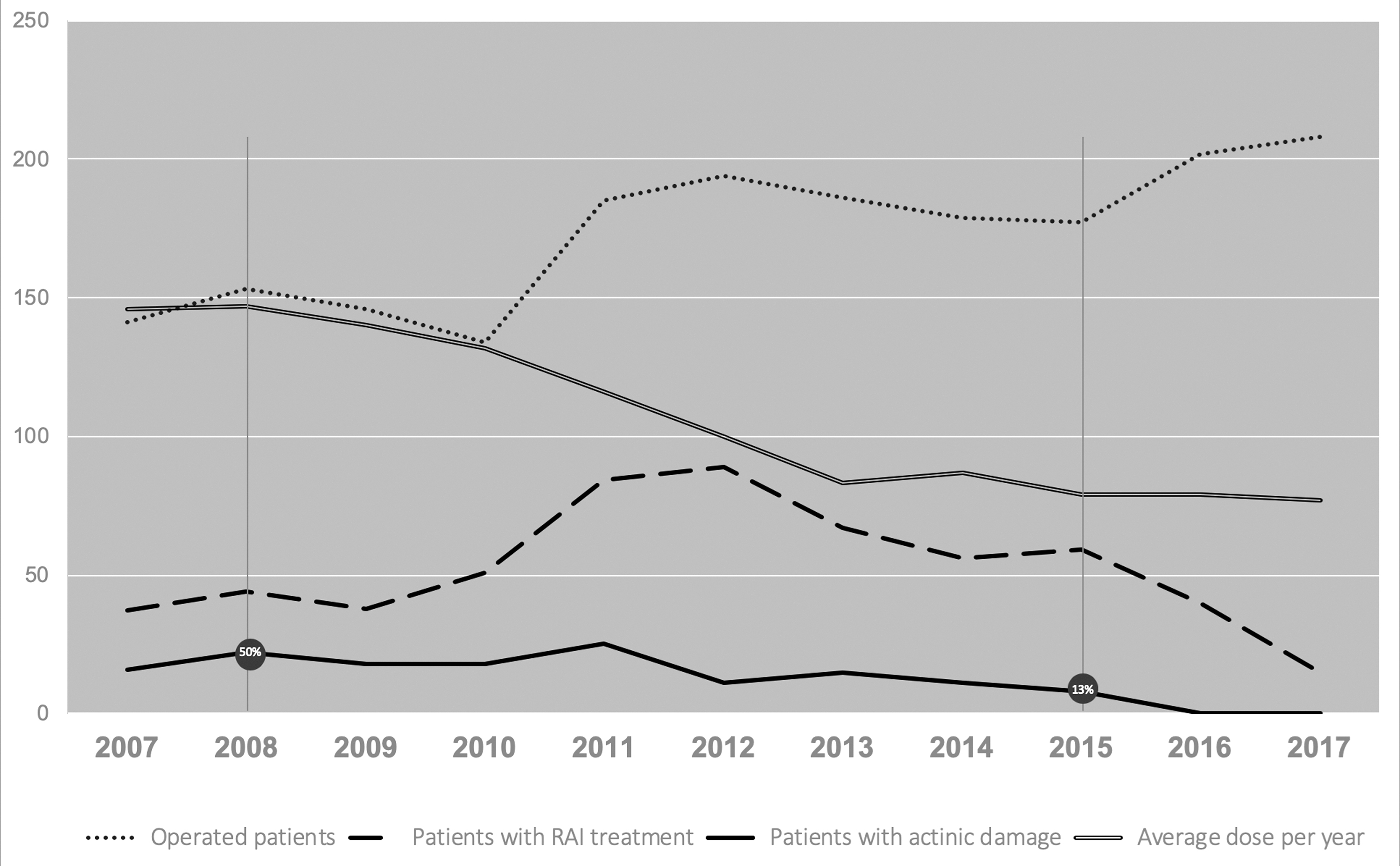
This graphic shows the effects of management modifications introduced in the past 10 years in our center, based on the results of this work regarding the prevalence of RAI-induced salivary gland damage. Thyroid surgeries have increased in the last decade (dotted line). Since 2012, the number of patients receiving RAI treatment has been decreasing (dashed line). The median administered dose is also clearly decreasing (double line). As a consequence, the damage in the major salivary glands has decreased significantly (continuous line) from 50% (2008) to 13% (2015), and even to 0% since 2016.
We used US to evaluate salivary gland damage because it is an excellent low-cost, noninvasive diagnostic tool for the study of the major salivary glands. The US examination can confirm their morphological integrity and reveal anatomical changes such as atrophy related to different chronic diseases (Sjögren syndrome, sialolithiasis, and actinic damage after external radiotherapy of the neck and after RAI), which all have the same appearance on US (24 –26). However, there are few reports on the use of US in patients treated with RAI, despite the noninvasive nature of this easily performed imaging test. In 2013, Brozzi et al. (14) studied salivary damage in 43 patients treated with RAI for differentiated thyroid cancer, identifying changes in parotid volume and echogenicity in patients with xerostomia symptoms. Kim (15), in his retrospective series, also described US changes post-RAI (coarse echotexture, decreased echogenicity, lobulated margin, and decreased gland size) in 94 of 202 (46.5%) patients operated on for PTC and treated with RAI. Roh et al. (16) retrospectively identified 111 (43.4%) of 256 patients with morphological changes on US in the major salivary glands after RAI but found no association between xerostomia and sonographic features.
To the best of our knowledge, this is the largest and first study that systematically and prospectively analyzed the damage to the major salivary glands by US in RAI-treated patients with PTC. Because the salivary glands are easily accessible, we recommend that this group of patients have routine US neck examinations. According to this experience, US changes are evident after one-year post-RAI. For this reason, one of our inclusion criteria was that at least 12 months had to have elapsed between RAI and the first US follow-up. In early-performed US controls (at 6–8 months), we can observe normal salivary glands or a slight alteration in size, margins, structure, and echogenicity. After the first year, the established atrophy remains virtually unchanged and with no perceptible changes over time. Color Doppler does not provide relevant additional information in this pathology.
It is necessary to highlight that US-detected atrophy of the parotid glands is not synonymous with clinical symptoms. Of our 54 patients surveyed, 23 (42.5%) suffered atrophy in at least one of their major glands on US, but only 16 reported discomfort (2 with unilateral and 14 with bilateral atrophies), and 7 of 9 patients with unilateral parotid damage were asymptomatic. In addition to the salivary symptoms, 8 (14.8%) of the women surveyed had lacrimal symptoms (excessive lacrimation) caused by duct stenosis. Only one woman was operated on. Of the 54 respondents, 14 (25.9%, all with bilateral atrophy) stated that after receiving RAI their quality of life deteriorated to some degree (mild or moderate).
The salivary glands function is studied with scintigraphy with technetium-sodium pertechnetate (99mTc). The quantitative or semiquantitative method provides an unspecific but sensitive method for detecting dysfunction of the salivary glands. Dynamic scanning shows that after the radiotracer injection, healthy glands avidly concentrate it to levels up to 100 times higher than in plasma. After orally administered diluted lemon juice, the dynamics of the excretion (washout fraction) are observed (12,13). Malpani et al. (20) observed abnormal parenchymal uptake, duct secretory clearance, or both, in 73% of patients who received an average of 13,875 MBq (375 mCi) of RAI. In our practice, we initially performed several salivary gland scintigraphies, which showed absent excretion of the glands with US abnormalities (Fig. 6). Nowadays, this study is no longer necessary since ultrasound, despite being an anatomical imaging method, is sufficient to assess irreversible morphological damage and dysfunction of the affected glands.
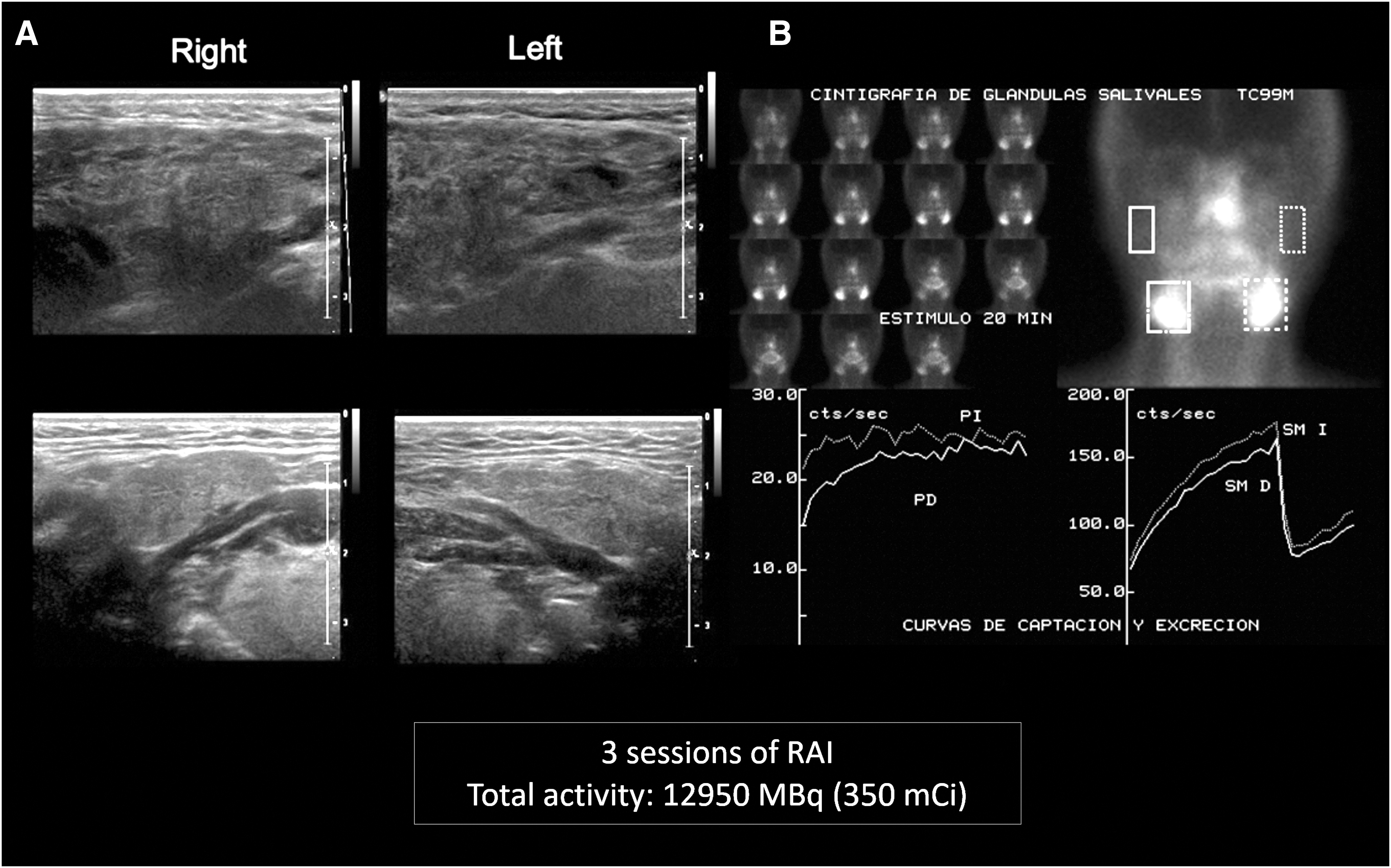
US (
Consistent with the findings by other authors (14,15), we also observed that the submandibular glands are less frequently damaged: in this series, we found 143 patients with parotid atrophy (unilateral or bilateral), but only 14 of them (9.8%) had additional damage to the submandibular glands. This could be explained by the fact that the parotid gland is mainly composed of serous, radiosensitive epithelial cells and has greater activity than the submandibular gland, and therefore, it is more likely to be damaged (10,19,27,28). However, the submandibular glands have a mixed composition (serous and mucous cells), which makes them more resistant.
We would like to mention that the majority of patients with parotid damage experienced a painful increase in parotid volume throughout the first months (caused by acute inflammatory infiltration). This complication is less well known among many clinicians. Since this side effect is sometimes not associated with RAI, affected patients may visit maxillofacial surgeons or dentists and undergo useless and complex diagnostic testing (sialogram, CT, etc.). It is important to educate RAI-treated patients and advise them that if they experience painful swelling of their parotids, they should stimulate the damaged gland with citrus (lemon juice) to allow passage of the ductal debris/mucous plug that is momentarily obstructing the Stenon conduit. External massage of the gland and Stenon's duct may also be helpful (29). These episodes may recur a few times and then resolve spontaneously.
Finally, it should be noted that in this study all patients received the same recommendation before the administration of RAI regarding the use of sialagogues: they were instructed to drink abundant liquids and suck on sour candy for 24–48 hours, starting 24 hours after receiving RAI. We did not evaluate the patient's compliance with the recommendations. However, it is interesting to note that after January 2011—the time of implementation of our new guidelines that put special emphasis on the explanation how to reduce the risk of salivary gland damage—we have observed that this factor (general information vs. personalized instruction) also proved to be significant in both the univariate and multivariate analysis, without changing the activity-related risk. The potential benefit conferred by the use of sialagogues using various protocols will have to be assessed in future studies.
Our work has certain limitations: (i) it is a single-institute study, (ii) we did not correlate the results of US atrophy with scintigraphy, the reference standard used in the literature (after our first studies, we considered it useless to perform expensive, invasive radiation-based examinations), and (iii) only a sample of patients was surveyed.
In summary, US was used for the first time to systematically evaluate the major salivary glands in preoperative evaluation and follow-up of patients who underwent RAI treatment after thyroidectomy for PTC. Sialadenitis is common and affects ∼25% of patients who receive 3700 MBq (100 mCi) or more RAI. The total RAI activity administered is the main factor related to this radioiodine-induced chronic atrophy, fact that should be taken into consideration when determining the activity of RAI in the treatment of patients with thyroid cancer.
Footnotes
Acknowledgments
Our gratitude to Dr. Jorge Sapunar for his valuable advice on the statistical analysis of data, Olenkha Cepeda for her help in providing bibliographical material, Dr. Guillermo Chong for his assistance on nuclear medicine issues, and Raquel Vicuña for her invaluable collaboration in the editing of this article and submission process to Thyroid Journal.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.