
Abstract
Background:
The impact of thyroid disorders on in vitro outcomes of assisted reproductive technology (ART) remains controversial. Therefore, the aim of our study was to investigate whether thyroid peroxidase antibodies (TPO-Abs)/thyroid autoimmunity (TAI) or thyroid function (serum thyrotropin [TSH])/subclinical hypothyroidism are associated with an altered number of oocyte retrieval (NOR), fertilization rate (FR), and embryo quality (EQ).
Methods:
Cross-sectional study in 279 women in a single center, comprising 297 cycles and 1168 embryos. In vitro data (NOR, FR, and EQ) were documented in two groups; one according to thyroid function in women without TAI (TSH ≤2.5 and >2.5 mIU/L) and one according to the presence/absence of TAI (determined by TPO-Abs). EQ was evaluated according to international criteria and classified as excellent/good and poor. Women treated with levothyroxine (LT4) were excluded. Furthermore, the impact of thyroid parameters on outcomes, normal NOR (>6 or 8) and high FR (>60%), was verified in a multivariable logistic regression model.
Results:
In women without TAI, 27% had TSH levels >2.5 mIU/L, the prevalence of TAI was 8%, and overall, 6% of women had TSH levels >4.2 mIU/L. NOR, FR, and EQ were comparable between study groups. In the regression analysis, women aged ≥30 years and receiving a high ovarian stimulation dosage (>2300 IU/cycle) had lower rates of normal NOR (odds ratio [OR] 0.18 [95% confidence interval, CI 0.04–0.72]; p = 0.016 and OR 0.17 [CI 0.06–0.48]; p < 0.001, respectively).
Conclusions:
Our results do not suggest an impact of thyroid antibodies/autoimmunity and (dys)function on ART in vitro outcomes.
Introduction
Thyroid hormones (TH) may interact directly with oocyte physiology via the presence of TH receptors in granulosa/cumulus cells and indirectly by facilitating the actions of the follicle stimulation hormone (FSH) on granulosa cells in terms of the steroidogenic activity, cellular morphology, the expression of the LH/CG receptor, and by protecting them against apoptosis via the PI3-K pathway (1 –3). Thyrotropin (TSH) receptors are also present on human ovarian tissue and granulosa cells, but their function needs to be investigated further (4).TH and thyroid antibodies are present in follicular fluid (FF) in concentrations that correlate with those in the serum, and recently, it has been suggested that thyroid peroxidase (TPO) might be present in granulosa cells (5 –8).
Therefore, thyroid antibodies can be cytotoxic for the zona pellucida and hamper the interaction between the oocyte and the sperm cell (9,10).
Subclinical hypothyroidism (SCH) and thyroid autoimmunity (TAI) have been associated with an impaired ovarian reserve, lower oocyte quality, decreased fertilization rates (FRs) and a lower rate of high-quality embryos (6,11 –16). However, this was not the case in other studies (7,17 –19). Heterogeneity in study results may be explained by differences in the anti-Müllerian hormone (AMH) assays, as well as the timing of the measurement and reference ranges of TSH, and in the definition of ovarian reserve and embryo quality (EQ).
Therefore, the aim of our study was to investigate whether thyroid peroxidase antibodies (TPO-Abs)/TAI or thyroid function (serum TSH)/SCH were associated with altered in vitro outcomes of an assisted reproductive technology (ART) procedure, and more in particular with the number of oocyte retrieval (NOR), the FR, and EQ.
Materials and Methods
Overall study design
All data were retrieved from the CHU St-Pierre clinic of medically assisted procreation (PMA), a public university hospital in Brussels, Belgium. The enrollment consultation is systematically completed with a biological analysis, including the measurement of TSH, free thyroxine (fT4), and TPO-Abs. Furthermore, demographic data, including the women's background and fertility (obstetrical) history, are also noted in the records.
We report here on data of a cross-sectional analysis of infertile women (period 01-01-2017/31-05-2018), nested within an ongoing prospective collection of women's infertility history and biological data. The determination of the background of the women was based on a history taken by the social workers that includes systematically the nationality at birth and the origin of the women.
From 631 women visiting the PMA clinic during the study period, 279 were included of whom 1168 embryos were scored for their quality. Women who consulted for social/oncological reasons (n = 35), in whom thyroid function or antibody tests were not complete, who performed their analyses more than three months before the pickup day (n = 287), and those treated with levothyroxine (LT4) before screening (n = 30) were excluded.
Figure 1 illustrates the study selection process in a flowchart.
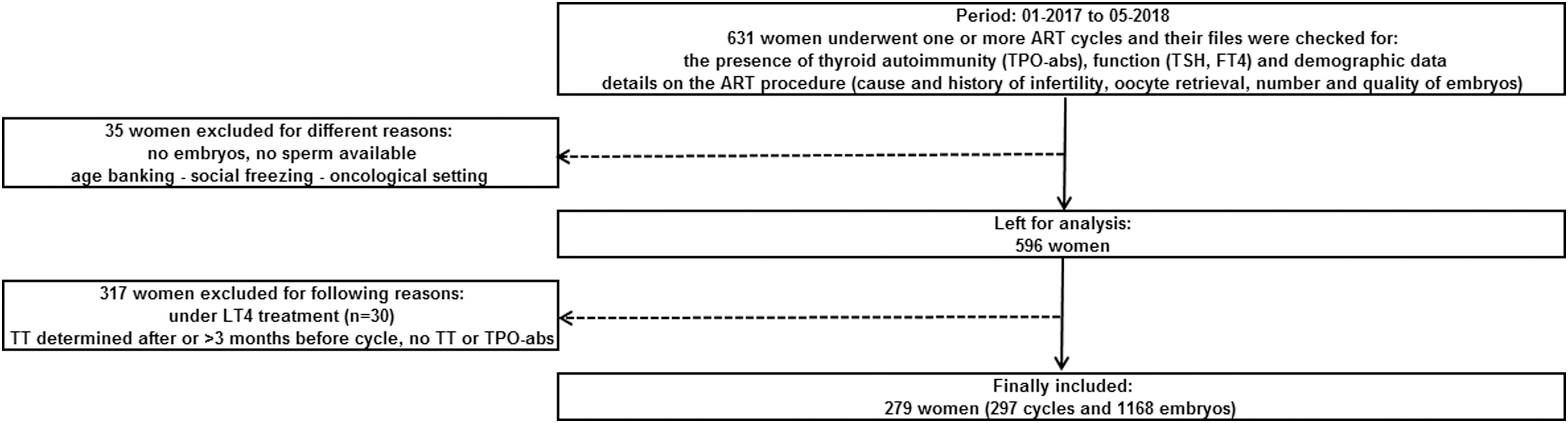
Flowchart of the study selection process. ART, assisted reproductive technology; ATD, antithyroid drugs; BMI, body mass index; fT4, free thyroxine; LT4, levothyroxine; TPO-Abs, thyroid peroxidase antibodies; TSH, thyrotropin; TT, thyroid tests.
In both study groups (one according to the presence/absence of TAI and one in women without TAI with TSH levels ≤2.5 and >2.5 mIU/L), parameters were expressed as continuous data for TSH, fT4, TPO-Abs, women's and partners age, BMI, parity, number of cycles, units of ovarian stimulation (OS), oocyte retrieved, FRs, and embryos obtained, transferred, and frozen. Older age (≥30 years), obesity (≥30 kg/m2), smoking (yes/no), history of miscarriage (≥2), primary infertility, and EQ (excellent/good and poor) were expressed as categorical data.
EQ was assessed using criteria established in the Vienna Consensus workshop (20). Embryos were considered of good quality if they reached four-cell stage on day 2 after fertilization and eight-cell stage with Grades 4 or 5 on day 3. They were considered of poor quality if they arrested, degenerated, or only reached Grade 2; and they were considered fair if they fell in-between the first two other groups. We pooled good and fair embryos into one group.
The study was approved by the institutional review board (CE/19-01-16).
ART procedure
OS was performed with hMG (Menopur®; Ferring), recombinant FSH (Puregon®; MSD or Gonal-F®; Merck-Serono or Bemfola®; Gedeon Richter), or corifollitropin alfa (Elonva®; MSD). The dose of gonadotropins was determined on an individual basis according to the woman's age, day three serum FSH value, and antral follicle count. Pituitary inhibition was obtained by a gonadotropin-releasing hormone (GnRH) analog (long or short protocol) (Suprefact®; Sanofi-Aventis or Decapeptyl®; Ipsen) or GnRH antagonist (Orgalutran®; MSD or Cetrotide; Merck-Serono). Cycle monitoring was carried out using transvaginal sonography and laboratory assays. When three or more leading follicles reached 17 to 18 mm, 5000–10,000 IU of hCG (Pregnyl®; MSD) was administered. Oocyte retrieval was performed transvaginally and ultrasound-guided 34 to 36 hours after hCG injection.
The collected cumulus–oocyte complexes (COCs) were counted and routinely incubated in an organ dish; then oocytes were stripped of cumulus cells with hyaluronidase and mechanical denudation. Semen was prepared by the gradient technique. Oocytes were subsequently inseminated using either conventional in vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI). After having excluded severe male factor infertility, the indications for IVF technique were tubal factor or unexplained infertility, and ovulation failure with all possible conventional methods. ICSI was preferred in case of previous fertilization failure with conventional IVF, retrieval of poor-quality oocytes or of a small number of oocytes, high titers of antisperm antibodies, and fertilization with frozen/thawed oocytes.
In idiopathic infertility during the first ART attempt, half IVF or half ICSI was preferred to identify a possible fertilization problem that would explain infertility.
Serum assay
All laboratory analyses were provided by the laboratory of hormonology at our institution.
Serum TSH was measured using a sandwich immunoassay with electrochemiluminescence detection on a Roche analytical platform (TSH; Roche Diagnostics, Mannheim, Germany). The coefficient of variation (intermediate precision) is 3.5% at 1 mIU/L, and reference values are 0.27–4.2 mIU/L (P2.5-P97.5).
Serum fT4 was measured using a competitive immunoassay with electrochemiluminescence detection on a Roche analytical platform (fT4; Roche Diagnostics). The coefficient of variation (intermediate precision) is 3.5% at 12.8 pmol/L. Reference values are 12–22 pmol/L (P2.5–P97.5).
Serum TPO-ab levels were measured using the Elecsys electrochemiluminescence immunoassays on a Cobas 6000 immunoanalyzer (Roche Diagnostics). The inter- and intra-assay CV for TPO-Abs is <5% and ≤7%, respectively, and the reference values are <34 kIU/L.
Statistical analysis
Data were stored in a Microsoft Excel database. Continuous data are expressed as median (Q1–Q3) when not normally distributed, and as mean ± SD for normally distributed data. Categorical data are presented as numbers (percentage) of cases. Differences between groups (TAI− vs. TAI+ and TSH ≤2.5 vs. TSH >2.5 mIU/L) were analyzed by chi-square or Fisher's exact test for categorical data and by the Mann–Whitney U test for continuous data. Correlations between continuous variables were quantified using Spearman's ρ correlation coefficient when data were not normally distributed, and a Pearson's correlation for normally distributed data.
For the logistic regression analysis, the independent variables were fT4 levels in the whole range, TSH 2.5–4.2 mIU/L, TSH >4.2 mIU/L, TAI (TPO-Abs ≥34 kIU/L), age ≥30 years, BMI ≥30 kg/m2, tobacco use, male infertility (corrected for donor sperm), age of the male ≥40 years, type of pituitary downregulation, high OS/cycle (>2300 IU), ICSI as type of ART (without taking split cycles into account), and >1 previous ART cycle. Two dependent outcomes were taken into account: age-adapted normal oocyte retrieval rate (for women <36 years >8 oocytes and ≥36 years >6) and high FR (>60%) (20).
All statistical tests were considered significant whenever p < 0.05.
Results
Table 1 shows baseline demographic and thyroid parameters in the two study groups.
Baseline Demographic and Thyroid Parameters in the Two Study Groups
Significant values are indicated in bold.
Continuous data are expressed as mean ± SD when normally distributed, or as median (Q1–Q3) otherwise.
Data available in 260 women.
fT4, free thyroxine; Q1–Q3, quartile 1 and 3; N/A, not applicable; TAI, thyroid autoimmunity; TPO-Abs, thyroid peroxidase antibodies; TSH, thyrotropin.
Serum TSH and fT4 levels of all women included were 1.93 (1.30–2.61) mIU/L and 15.5 ± 2.0 pmol/L, respectively. Median (Q1–Q3) TPO-ab levels for all women were 15 (15 –17) kIU/L.
Eight percent of all women had TAI (n = 25). In women with TAI, 28% (n = 7) had TSH levels 2.5–4.2 mIU/L and 20% (n = 5) had TSH levels >4.2 mIU/L. The prevalence of TSH levels >4.2 mIU/L was significantly lower in women without TAI, 4% (n = 12); p = 0.001.
In women without TAI (n = 272), the majority had low-normal TSH levels ≤2.5 mIU/L (n = 199; 73%). By definition, serum TSH levels in women with TAI were significantly higher compared with those in women without TAI (2.27 [1.73–3.86] vs. 1.88 [1.28–2.56] mIU/L; p < 0.001).
Overall, the mean age of the women was 36.4 ± 5.0 of whom 89% were ≥30 years; 13% were obese and 13% smoked.
In women with a sub-Saharan background and without TAI, the prevalence of serum TSH levels ≤2.5 mIU/L was higher compared with TSH levels >2.5 mIU/L (30% vs. 16%; p = 0.023). The opposite was true in a pooled group of women with different backgrounds (Hispanic, Turkish, and Asian), in whom the prevalence of TSH levels >2.5 mIU/L was higher compared with TSH levels ≤2.5 mIU/L (19% vs. 7.0%; p = 0.004).
Table 2 shows details on infertility/obstetric history and in vitro outcomes in the two study groups.
Details on Infertility/Obstetric History and In Vitro Outcomes in the Two Study Groups
Significant values are indicated in bold.
Continuous data are expressed as mean ± SD when normally distributed, or as median (Q1–Q3) otherwise.
Data available in 277 women.
ART, assisted reproductive technology; FR, fertilization rate; GnRH, gonadotropin-releasing hormone; ICSI, intracytoplasmic sperm injection; IVF, in vitro fertilization.
The prevalence of women with primary infertility was 52% and comparable between study groups. The median (Q1–Q3) number of cycles women had before the one taken into account for this study was 1 (1–2) and comparable between groups.
In women with TAI, the prevalence in whom the cause of infertility was due to a male factor, was higher compared with that in women without TAI (48% vs. 23%; p = 0.006). ICSI was applied mostly as type of ART (55%), with a slightly (nonsignificant) higher percentage applied in women with TAI compared with that in women without TAI (68% vs. 54%; p = 0.179). GnRH antagonists were used mostly to initiate the ART procedure (81%) and the mean dosage of gonadotropins used to stimulate the ovaries was 1961 ± 966 IU (comparable between groups).
The mean (SD) number of oocytes retrieved was 6.5 ± 4.4, the FR was 61.2% ± 29.8%, the number of embryos obtained was 3.9 ± 3.1, that of transferred embryos 0.9 ± 0.8, and the median (Q1–Q3) of embryos frozen 0 (0–2). All results were comparable between groups.
The number of embryos scored for quality evaluation was 1168. Overall, 44% were scored as good to excellent and 56% as poor; results were comparable between groups.
The FRs in women with TAI only treated with ICSI (n = 16) versus IVF (n = 3) were comparable (59% vs. 63%; p = 0.806).
Table 3 shows the correlations between the in vitro outcome data and thyroid parameters expressed as continuous variables.
Correlations Between the In Vitro Outcome Data and Thyroid Parameters Expressed as Continuous Data
For the correlation between the outcomes and TSH/fT4, a Pearson's test was used, and for that with TPO-Abs, a Spearman's test.
None of the in vitro outcomes correlated with serum TSH, fT4, or TPO-ab levels.
For details and p-values see (Table 3).
Table 4 shows the results of the multivariable logistic regression analysis with thyroid, demographic, and ART characteristics as independent variables, and normal NOR and high FRs as dependent outcomes.
Multivariable Logistic Regression Analysis with Thyroid, Demographic, and Assisted Reproductive Technology Characteristics as Independent Variables, and Normal Number of Oocyte Retrieval and High Fertilization Rates as Dependent Outcomes
Significant values are indicated in bold.
Normal oocyte retrieval rate is age dependent: for women <36 years this is >8 oocytes and ≥36 years >6.
Controls corrected with serum TSH levels >4.2 mIU/L.
Corrected for donor sperm.
Corrected for split ART cycles.
aOR, adjusted odds ratio; CI, 95% confidence interval; TAI, thyroid autoimmunity.
Normal NOR (>6 or >8 oocytes according to age) and high FRs (>60%) were not associated with any of the thyroid parameters. Variables associated with a normal NOR rate were age ≥30 years (odds ratio [OR]: 0.18 [95% confidence interval, CI 0.04–0.72]; p = 0.016) and a high OS per cycle (>2300 IU) (OR: 0.17 [CI 0.06–0.48]; p < 0.001).
Discussion
Women pregnant after an ART procedure with thyroid disorders have impaired live-birth rates compared with women without thyroid disorders. The precise underlying pathophysiological mechanism for that association remains unclear, but an impact of thyroid disorders on the earliest stages of the ART procedure—that is, on the number of oocytes retrieved, the FR, and the EQ—has been suggested (7,11 –15,21,22).
We did not observe an association between thyroid function (TSH, fT4), thyroid antibodies (TPO-Abs), and the NOR, FR, or EQ. Moreover, our results did not change when SCH (TSH >4.2 mIU/L) or TAI (TPO-Abs ≥34 kIU/L) was taken into account.
Concerning the absence of an association between TAI and NOR, our data are in line with those in several other studies (7,12,15,21,23 –26). The NOR is determined by a number of parameters, such as the ovarian reserve and stimulation, the underlying causes of infertility, and the women's age (27). In our study, age and other baseline characteristics were comparable between women with and without TAI, but in the logistic regression analysis, age ≥30 years was a negative predictor of a normal NOR. It has been hypothesized that TAI might have a negative impact on the NOR, by decreasing the ovarian reserve (14,16), although in a large number of other studies, this was not the case (7,15,18,19,24 –26).
Thyroid antibodies are present in FF in concentrations that correlate with those in the serum, and therefore may have a direct cytotoxic impact on the oocytes (5 –10). Opposite study results might have been due to differences in study populations (idiopathic low ovarian reserve and genetic causes, among others) and in the methodology used to determine ovarian reserve. It is noteworthy that the detrimental impact of TPO-Abs in the study by Korevaar et al. was independent of the FSH levels, and that there was no impact of Tg-Abs (16).
Since the presence of TAI is the most important cause of SCH, the impact of TAI on the NOR and ovarian should be adjusted for thyroid function (28,29). In our study, the NOR was not associated with thyroid (dys)function. To the best of our knowledge, the only other study that investigated the impact of thyroid function (all TSH levels and as a group with TSH >2.5 mIU/L) on the NOR was also negative (12).
In some studies, ovarian reserve showed a correlation with serum TSH (13,16,18). In the study by Polyzos et al., no correlation was present between TSH/fT4 and low ovarian reserve of all causes (18). However, when the authors investigated genetic causes of low ovarian reserve only, a significantly higher prevalence of (subclinical) hypothyroidism was present compared with women with unexplained low ovarian reserve (and adjusted for age) (18). In a study by Weghofer et al., AMH levels were significantly lower in women with serum TSH levels >3.0 mIU/L after adjustment for TAI and age (13). Finally, in a study by Korevaar et al., lower serum free triiodothyronine (fT3) levels were associated with a lower antral follicle count (16). T3 is the bioactive form of TH and mainly produced intracellularly via deiodination of T4 in peripheral tissues. Animal studies have shown that the ovary can concentrate iodine, produce local T3 through deiodination, and that T3 has an effect on estrogen availability, and maybe on other hormones in the FF (1,8,30,31).
FF is easily available during oocyte pickup and could represent an optimal source of noninvasive biochemical predictors of oocyte quality (32). However, the impact of TAI on oocyte quality was investigated only in one study, without revealing a significant association (7). It is noteworthy that oocyte quality is ill-defined due to a lack of consensus of the criteria, and therefore, in most studies (including ours) oocyte quality was not investigated as outcome.
FRs were comparable between women with and without TAI, in analogy with most data in the literature (7,15,22,25,33,34). However, in two studies, lower FRs were present in women with TAI (6,35). The authors speculated that TPO-Abs may bind to the surface of the egg and/or embryo and interfere with fertilization and subsequent embryo development. Furthermore, we did not observe an association between thyroid (dys)function (TSH/fT4 and SCH) and FRs. Our results were comparable with those in the study by Michalakis et al. (TSH values 2.5–4 mIU/L) (36). However, in the study by Cramer et al., TSH levels were inversely proportional to the FR, and in the study by Scoccia et al., lower FRs were present in hypothyroid women not treated optimally with LT4; in the meta-analysis by Velkeniers et al., LT4 treatment improved the FR in women with SCH (11,37,38). Differences in study results on the FR may be due to different definitions of thyroid dysfunction and/or the absence of information on TAI.
In some studies, ICSI has been associated with better FRs compared with that in IVF cycles (39). ICSI has been used for over 20 years, and high FRs have been reported since its implementation (40). The concept that in women with TAI, ICSI might be the better ART technique is based on the fact that, in contrast to IVF, it may overcome the impact of thyroid antibodies in the FF (hampering the interaction between the oocyte and the sperm cell) (6,39). However, in our logistic regression analysis, ICSI was not a predictor for a high FR. In the study by Andrisani et al., in which no difference in the FR was present in relation to TAI, IVF was used more frequently in women with TAI compared with that in women without TAI (15). In the two studies with a lower FR in women with TAI, Zhong et al. did not report on the type of ART used (the selection of fertilization program was based on the semen condition on the day the oocytes were collected), and in the study by Monteleone et al., the application of ICSI was comparable between women with and without TAI (6,35).
In the future, head to head studies should be performed comparing the FR in women with TAI treated either with IVF or with ICSI to clarify this issue.
A successful fertilization depends on a number of covariates besides the ART technique. The most important are the woman's age, the cause of infertility, and thyroid function. In a recent meta-analysis by Poppe et al., TSH levels were <3.0 mIU/L in all studies included (34). In the study by Zhong et al. (with a lower FR in women with TAI), 13.8% of women with TAI had an increased TSH level, which was only observed in 2.4% of women with TAI, but the authors mention that TSH levels were not determined for all patients, an important study limitation (35).
Finally, we assessed EQ in 1168 embryos and classified them as of good/moderate or poor quality according to expansion, inner cell mass, and trophectoderm criteria (20). No difference was observed in relation to thyroid parameters nor in the continuous or categorical analysis. Also in three other studies, EQ was not associated with TAI (7,17,23). However, in as many other studies, a negative impact of TAI (corrected for age and thyroid function) on the number of top embryos compared with that in women without TAI has been reported (6,12,15). Monteleone et al. suggested using ICSI in infertile women with TAI since it requires no interaction between the sperm cell and the zona pellucida (6). However, in the study by Weghofer et al., an impaired EQ in women with TAI was independent from the use of ICSI (12). In that study, serum TSH levels in the whole range (0.45–4.5 mIU/L) were not correlated with EQ, but in women with TSH levels >2.5 mIU/L, a higher rate of poor EQ was present (12). Scoccia et al. showed that hypothyroid women who were optimally treated with LT4 had a similar EQ with that in euthyroid women, and in a study by Kim et al., including women with SCH (TSH levels >4.0 mIU/L), LT4 treatment increased the number of top-quality embryos compared with that in the placebo group (33,37).
Differences in results on the EQ may have been due to heterogeneity in the definition of poor EQ. In our study and that by Weghofer et al., poor EQ included arrested and degenerated embryos, while in the study by Andrisani et al., arrested and degenerated embryos were excluded (12,15). Finally, it is also possible that the impact of thyroid antibodies/hormones on the EQ is erased due to the replacement of the FF after the pickup by a standard growth medium.
Overt hypothyroidism or severe SCH (TSH >4.0 mIU/L) can lead to infertility via different pathways such as hyperprolactinemia, menstrual irregularity, and others (22,28). Therefore, the American Society for Reproductive Medicine recommends screening infertile women for serum TSH and for TPO-Abs if the TSH is >2.5 mIU/L (41). The American Thyroid Association guidelines on thyroid disorders and pregnancy state that there is insufficient evidence to recommend for or against universal screening for altered TSH concentrations before conception, except in women planning ART (42). However, no position was taken on the testing of thyroid antibodies as such. Based on our in vitro study results, we do not add evidence that strengthens the systematic screening of TSH/TPO-Abs in infertile women (42 –44). However, screening may be important for the later phase of the ART procedure, since TPO-Abs are associated with the development of (subclinical) hypothyroidism after OS, and indicate which women treated with LT4 should adapt their dosage before OS (42 –44).
Indeed, Busnelli et al. showed that 80% of hypothyroid women pregnant after OS and with TAI had to increase their dosage of LT4 within the first seven weeks of pregnancy, compared with 40% without TAI (44). Women with TAI are also more prone to develop SCH during pregnancy, even when they were euthyroid in the first trimester of pregnancy (28,42). Moreover, it is known that the prevalence of women with the polycystic ovarian syndrome and idiopathic infertility have a higher prevalence of TAI compared with fertile women (22,28).
One minor study result was the lower and higher prevalence of TSH levels >2.5 mIU/L in women with a sub-Saharan background and in a group composed of women with different backgrounds (Hispanic, Turkish, and Asian).
In a previous study in pregnant women, we have shown that women with a sub-Saharan background have a lower prevalence of TAI, what might explain their lower prevalence of TSH levels >2.5 mIU/L (45). It is difficult to give a precise explanation why the prevalence of TSH levels >2.5 mIU/L was higher compared with that of TSH levels ≤2.5 mIU/L in the group of women including different backgrounds (Hispanic, Turkish, and Asian). Differences in the thyroid/pituitary set point may play a role, as it was shown in blood spots performed for birth screening that mean TSH levels differed according to the ethnicity of the babies (46).
Strengths of our study are the real-world setting, including women with different causes of infertility, treated with different ART types and with different ethnicities. Inclusion criteria were strict, women with alternative indications of ART, or treated with LT4, were excluded. The time frame in which thyroid function and autoimmunity was determined in relation to the day of pickup was limited to three months before OS; in other studies this time frame was not always mentioned, and when thyroid function is determined after OS, it might have changed (43,44). Our analysis of thyroid parameters in relation to the study outcomes was done in a continuous and categorical way, and data were collected in a prospective way.
Our study has also some limitations. The numbers of patients with TAI and SCH (TSH levels >4.2 mIU/L) is rather low, in part, due to the exclusion of women treated with LT4. Semen parameters were expressed in a semiquantitative way as male infertility or not.
The diagnosis of TAI was based on the presence of TPO-Abs only, and not testing for Tg-Abs may have led to misclassification, since isolated positivity for Tg-Abs may occur in 5% of infertile women (47). We did not measure TH, TPO-Abs, or other hormones such as steroids, estrogens, and progesterone in the FF, and we did not characterize ovarian reserve and quality.
In our study, the absence of any impact of thyroid parameters on the in vitro parameters might have been due to methodological issues. However, we believe that the effectiveness of the ART procedure in its totality, starting with the pituitary downregulation and ovarian hyperstimulation, the oocyte recruitment and cultivation in a special growth medium, and the ART techniques (IVF and ICSI) for the fertilization are all very efficient and as such may overcome the potential impact of thyroid disorders on NOR, FR, and EQ.
Finally, the importance of thyroid disorders might appear only once women are pregnant, and therefore, clinical pregnancy outcome data of this cohort of women need to be investigated further.
In conclusion, no impact of TAI or (dys)function was observed on the number of oocytes retrieved, FRs, and EQ in women undergoing ART.
Footnotes
Acknowledgments
The authors thank Bénédicte Beckers (biologist PhD) and Siham Benallal (MD) for their help on the collection of the data.
Author Disclosure Statement
K.P. received lecture fees from the IBSA Institut Biochimique SA (satellite meeting of the European Thyroid Association) in 2016 and the Berlin-Chemie AG company (ETA educational thyroid meeting) in 2017, 2018, and 2019.
Funding Information
No specific grant/fellowship from any funding agency in the public, commercial, or not-for-profit sector.