
Abstract
Background:
Fibrotic diseases have an unclear etiology and poor prognosis. Fluctuations in thyroid function may play a role in the development of fibrosis, but evidence is fragmented and inconclusive. This systematic review and meta-analysis aimed to investigate the association of thyroid function with fibrotic diseases of the liver, heart, and lung in humans.
Methods:
We searched PubMed, Medline Ovid, Embase Ovid, and Web-of-Science for studies published from inception to 14 June 2019, to identify observational studies that investigated the association of thyroid function with fibrosis of the liver, heart, and lung in humans. Study quality was evaluated by the Newcastle–Ottawa Scale. The Mantel–Haenszel method was used to pool the odds ratios (ORs) of studies investigating the association of hypothyroidism with liver fibrosis.
Results:
Of the 2196 identified articles, 18 studies were included in the systematic review, of which 11 studies reported on liver fibrosis, 4 on myocardial fibrosis, and 3 on pulmonary fibrosis. The population sample size ranged from 36 to 7259 subjects, with median mean age 51 years (range, 36–69) and median percentage of women 53 (range, 17–100). The risk of bias of studies was low to moderate to high. Higher serum thyrotropin and lower thyroid hormone levels were generally associated with higher likelihood of fibrosis. Compared with euthyroidism, overt and subclinical hypothyroidism was associated with a higher likelihood of fibrosis in the liver (six of seven studies), heart (three of three studies), and lung (three of three studies). Based on the results of the seven studies included in the meta-analysis, overt and subclinical hypothyroidism was associated with an increased risk of liver fibrosis (pooled OR, 2.81; 95% confidence interval [CI], 1.74–4.53; heterogeneity, I 2 31.4%; pooled OR, 2.12; CI, 1.45–3.12; heterogeneity, I 2 0%; respectively), without evidence of publication bias.
Conclusions:
This study suggests that low thyroid function is associated with increased likelihood of chronic fibrotic diseases of the liver, heart, and lung. However, the evidence is mainly based on cross-sectional data. Prospective studies and randomized clinical trials are needed to investigate the potential efficacy of thyroid hormone and its analogs on the occurrence and progression of fibrosis.
Introduction
Fibrotic diseases, including liver cirrhosis, hypertrophic cardiomyopathy, and idiopathic pulmonary fibrosis, represent a significant cause of disability and mortality (1 –4). The development of fibrosis is attributable to a maladaptive response characterized by the accumulation of extracellular matrix proteins such as collagen and fibronectin (5). Fibrotic elements progressively remodel and destroy the normal tissue architecture, ultimately resulting in organ failure. Hence, nonalcoholic steatohepatitis can progress to decompensated cirrhosis (6); and myocardial fibrosis leads to ventricular diastolic dysfunction (7); whereas pulmonary fibrosis contributes to a decline in the lung function (8).
To date, the prognosis of fibrotic diseases remains poor, owing to the poor understanding of its pathogenesis and the lack of effective therapeutic options. Therefore, current research is focused on the identification of novel determinants of fibrosis, which could be further translated into the development of effective treatments (9 –11). Among other factors, hypothyroidism has been implicated in the etiology of fibrosis (12 –15). Pronounced hypothyroidism is typically characterized by an increased production of mucopolysaccharides, resulting in interstitial fibrosis and extracellular water retention, also known as myxedema (16). Yet, the exact role of thyroid hormones in the development of fibrosis remains unclear as well as controversial. A number of animal studies have reported profibrotic effects of hypothyroidism (13,17 –21); and beneficial effects of thyroid hormone supplementation on fibrosis of the liver (22,23), heart (24 –26), and lung (27). In contrast, other animal studies have observed an attenuation of fibrosis in experimental hypothyroidism (28,29), and have shown profibrotic effects of thyroid hormone administration (30 –34). Similar to animal studies, the results of epidemiological studies are also inconsistent. Some studies suggest a link between thyroid function and the risk of fibrosis of the liver, heart, and lung (12,14,15), whereas others report no such association (35,36).
To date, there is a critical lack of literature synthesis concerning the impact of thyroid function on the occurrence and progression of organ fibrosis. Therefore, we aimed to summarize the current evidence regarding the association of thyroid function with fibrosis of the liver, heart, and lung in humans.
Materials and Methods
Data sources and search strategy
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines for transparent reporting (37). The checklist is provided in Supplementary Appendix SA1. Four electronic databases, including PubMed, Medline Ovid, Embase Ovid, and Web-of-Science, were searched without language restrictions from inception to 14 June 2019, with the help of expert librarians. From the date of the last search, we received monthly updates by the medical library to avoid missing new relevant references. The computer-based searches combined terms related to: (I) thyroid function (e.g., thyroid gland, thyroid disease, thyroid function, thyroid hormone, thyrotropin [TSH], thyroxine [T4], triiodothyronine [T3], thyronine, hyperthyroidism, thyrotoxicosis, Graves', hypothyroidism, Hashimoto, myxedema, deiodinase); (II) fibrosis of the liver, heart, and lung (e.g., liver fibrosis, nonalcoholic steatohepatitis, lung fibrosis, fibrosing alveolitis, fibrosing interstitial pneumonia, heart fibrosis); and (III) article type (i.e., editorials, letters to the editor, erratum, conference articles were excluded). Details of the search strategy are provided in Supplementary Appendix SA2.
Study selection and data extraction
The studies that fulfilled the following criteria were eligible: (I) observational studies, including cross-sectional studies, prospective studies, case/control studies, nested case/control studies, and nested case/cohort studies; (II) studies that investigated the association of hypothyroidism, hyperthyroidism, or thyroid parameters (i.e., TSH, free T4 [fT4], free T3 [fT3]) with fibrosis of the liver, heart, or lung in humans; (III) studies reporting effect estimates (risk ratio, odds ratio [OR], or hazard ratio) with 95% confidence intervals (CIs), or correlation coefficients (p-values) used to correlate thyroid function with fibrosis, or mean differences (with standard deviations; p-values) in thyroid function between cases and controls, or mean differences (with standard deviations; p-values) in fibrotic scores between thyroid status categories, or prevalence differences (p-values). Case reports, letters to the editor, proceedings, conference abstracts, reviews, systematic reviews, meta-analyses, and animal studies were excluded. The studies that focused exclusively on the role of thyroid function-altering medications on fibrotic diseases were also excluded. There were no restrictions on publication year or language.
Two independent reviewers (A.B. and S.R.) screened the titles and abstracts of the citations. The full texts of relevant articles were further obtained and independently evaluated. Any disagreement between the two reviewers regarding inclusion was resolved through consensus or with the help of a third independent reviewer. Full texts and reference lists of the selected articles were hand-searched to identify additional studies. A predesigned data collection form was used to extract relevant information from the selected studies, including article source, sample size, demographics of study participants, methods of assessing thyroid function and fibrosis, study results, and conclusions.
Quality assessment
The quality of the included studies was assessed separately by two reviewers (A.B. and S.R.) using the Newcastle–Ottawa Scale (NOS) for nonrandomized studies in meta-analyses (Supplementary Appendix SA3a) (38,39). The quality of cross-sectional studies was assessed using an adapted NOS version (Supplementary Appendix SA3b). NOS evaluates the study quality based on three domains, namely selection of participants, comparability of study groups, and ascertainment of the exposure or outcome of interest. Each study could have a maximum of nine stars. Based on the Agency for Healthcare Research and Quality standards, the quality of the studies was categorized as poor, fair, and good, corresponding to high, moderate, and low risk of bias, respectively (Table 4) (38,40).
Statistical analyses
For continuous outcomes, summary measures were presented as mean differences. To enhance the comparability among studies, we converted the units of measurements where appropriate. We used ORs with their CIs as provided by the included articles, or calculated them manually using available information. Fixed-effects Mantel–Haenszel models were used to obtain pooled ORs with CIs for the association of hypothyroidism, overt and subclinical hypothyroidism, with liver fibrosis (41). We constructed forest plots, and assessed heterogeneity using the I 2 statistic, with I 2 ≤25% considered low, 25% < I 2 <75% moderate, and I 2 ≥75% high (42). The possibility of publication bias was assessed using funnel plots and Egger regression symmetry tests (43). Statistical analyses were performed in Stata version 15.1 (StataCorp LLC, TX).
Sensitivity analyses
The following sensitivity analyses were performed: (I) we used random-effects models to account for heterogeneity. (II) We excluded the studies that provided unadjusted estimates, thus limiting the meta-analysis to studies that accounted for relevant potential confounders. (III) To assess the impact of individual studies on the overall results, we calculated the pooled risk estimates after removing one by one the studies from the analyses. (IV) To account for a possible influence of thyroid medications on our results, the studies on hypothyroidism were stratified in studies including or excluding the thyroid medication users. (V) We performed subgroup analyses by stage of hypothyroidism (i.e., overt or subclinical hypothyroidism). (VI) The studies were stratified based on the source population (nonhospitalized versus hospitalized patients). (VII) We performed subgroup analyses by study design (i.e., cross-sectional or longitudinal studies).
Results
Literature search
The results of the search strategy are presented in Figure 1. After excluding duplicates, we identified 2196 relevant citations; and after further screening of abstracts, 63 potentially relevant articles were identified. Once the full texts of these articles were examined, 18 eligible unique studies were selected (12,14,15,35,36,44 –56).
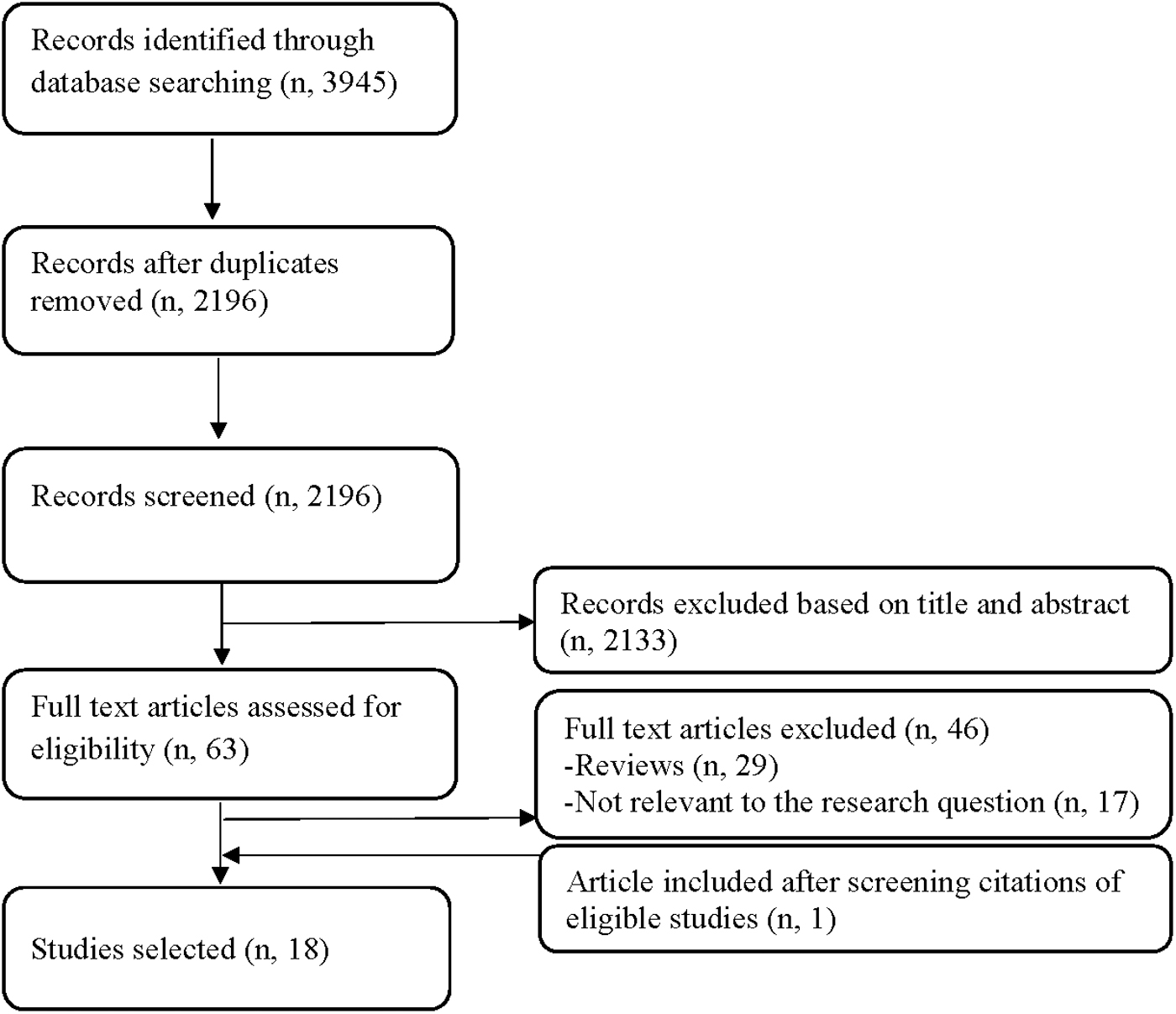
Flowchart for study inclusion, adapted from the PRISMA statement.
Thyroid function and fibrosis of the liver, lung, and heart
Table 1 summarizes the main characteristics of the 18 included studies reporting on the association of thyroid function with fibrosis of the liver, lung, and heart. The population sample size ranged from 36 to 7259 subjects (Table 1). The median mean age was 51 years (range, 36–69), and the median percentage of women was 53 (range, 17–100) (Table 1). Of the 18 included studies, 7 studies were performed in Asia (15,44,49,50,53 –55), 6 in the United States (14,35,45,46,48,51), 3 in Europe (12,47,52), 1 in Africa (56) and 1 in South America (36) (Table 1). Seventeen studies had a cross-sectional or case/control design, and 1 study had a prospective design (Table 1). Ten studies (14,15,35,45,47 –50,55,56) included hospitalized patients, 5 studies recruited participants from outpatient clinics (36,44,46,52,53), and 3 studies included participants from the general population (12,51,54) (Table 1). All studies controlled for confounders, except for 2 studies that reported unadjusted estimates (35,36) (Table 1).
Description of Included Studies on the Association of Thyroid Function with Fibrosis of the Liver, Heart, and Lung a
Information is related to the analyses of interest for our particular research question.
Stepwise strategy: statistically significant predictors were kept in the model.
T1-mapping of the myocardium assesses diffuse myocardial fibrosis. Increased T1-values reflect a longer relaxation time and a more advanced stage of diffuse fibrosis.
LGE imaging is used to assess myocardial fibrosis.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; chol, total cholesterol; CHPP, chronic hypersensitivity pneumonitis; COPD, chronic obstructive pulmonary disease; CS, corticosteroid; CT, computed tomography; HOMAIR, insulin resistance; IDCM, idiopathic dilated cardiomyopathy; IPF, idiopathic pulmonary fibrosis; LGE, late gadolinium enhancement; MRI, magnetic resonance imaging; n, total number; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; NR, not reported; OH, patients with overt hypothyroidism; SCH, patients with subclinical hypothyroidism; Tg, triglycerides.
The studies reported on blood measurements of thyroid function (TSH, fT4, fT3) (12,35,47,49,50,52,54 –56), overt hypothyroidism (12,14,15,36,45,46,48,53,55), subclinical hypothyroidism (12,44,50,51,55,56), and subclinical hyperthyroidism (12) (Tables 2 and 3). Of the 13 studies investigating hypothyroidism, 10 studies did not specify the cause of hypothyroidism and 3 studies defined hypothyroidism as Hashimoto's thyroiditis (Table 2). Several definitions of hypothyroidism were used. In six studies, the diagnosis of hypothyroidism was based on a self-reported disease history and use of thyroid hormone replacement therapy (14,36,45,46,48,53) (Table 2). Seven studies diagnosed overt and subclinical hypothyroidism based on the serum TSH and fT4 measurements, after excluding the thyroid medication users (12,15,44,50,51,55,56) (Table 2). Nine studies excluded patients with past thyroid surgery (Table 2).
Description of Studies Reporting on the Association of Hypothyroidism with Fibrosis of the Liver, Heart, and Lung
Bold values indicate presence of statistical significance.
Thyroid status categories were defined based on TSH and fT4 measurements. Subclinical hypothyroidism was diagnosed as increased serum TSH levels and normal serum fT4 levels. Clinical hypothyroidism was diagnosed as increased serum TSH levels and decreased serum fT4 levels.
Thyroid function was categorized into strict-normal (TSH 0.4–2.5 mIU/L) (reference), low-normal (TSH 2.5–4.5 mIU/L), and subclinical hypothyroidism (TSH >4.5 mIU/L).
Indicates mean difference (CI) in T1 values between hypothyroid patients and euthyroid subjects. T1-mapping of the myocardium assesses diffuse myocardial fibrosis. Increased T1-values reflect a longer relaxation time and a more advanced stage of diffuse fibrosis.
Cases had positive thyroid peroxidase antibodies.
Cases had positive thyroid peroxidase antibodies and positive antithyroglobulin antibodies.
CI, 95% confidence interval; fT4, free thyroxine; NS, not specified; OR, odds ratio; T1, myocardial longitudinal relaxation time; T1-IVS, T1-interventricular septum; T1-LVAW, T1-left ventricular anterior wall; T1-LVIW, T1-left ventricular inferior wall; T1-LVLW, T1-left ventricular lateral wall; T1-LV, left ventricular myocardial T1; THR, thyroid hormone replacement therapy; TSH, thyrotropin.
Description of Studies Reporting on the Association of Thyroid Parameters (TSH, fT4, fT3) with Fibrosis of the Liver, Heart, and Lung a
Bold values indicate presence of statistical significance.
The effect estimates in this table are presented as follows: (I) OR for the association of thyroid parameters with fibrosis; (II) mean difference in thyroid parameters between cases and controls; (III) correlation coefficient used to correlate thyroid parameters with T1-mapping; and (IV) prevalence of fibrotic disease throughout the range of thyroid parameters.
The reported estimates correspond to the euthyroid range or the full range of thyroid function.
Thyroid function was categorized into strict-normal (TSH 0.4–2.5 mIU/L) (reference), low-normal (TSH 2.5–4.5 mIU/L), and subclinical hypothyroidism (TSH >4.5 mIU/L).
T1-mapping of the myocardium assesses diffuse myocardial fibrosis. Increased T1-values reflect a longer relaxation time and a more advanced stage of diffuse fibrosis.
LGE imaging is used to assess myocardial fibrosis.
Converted from pg/mL.
Converted from pmol/L.
Converted from ng/L.
fT3, free triiodothyronine; MD, mean difference; r, correlation coefficient.
Quality Assessment Scale
The thresholds for converting the Newcastle–Ottawa Scale scores into the Agency for Healthcare Research and Quality standards were as follows: (I) good quality: 3 or 4 stars in the selection domain, and 1 or 2 stars in the comparability domain, and 2 or 3 stars in the exposure/outcome domain. (II) Fair quality: 2 stars in the selection domain, and 1 or 2 stars in the comparability domain, and 2 or 3 stars in the exposure/outcome domain. (III) Poor quality: 0 or 1 star in the selection domain, or 0 star in the comparability domain, or 0 or 1 stars in the exposure/outcome domain.
The outcomes were liver fibrosis (11 studies), myocardial fibrosis (4 studies), and fibrotic pulmonary diseases (3 studies) (Table 1). Of the studies assessing liver fibrosis, seven studies used liver biopsy (35,36,44 –47,53), three studies used fibrosis scores (51,52,54), and two studies used liver elastography (12,52) (Table 1). Myocardial fibrosis was assessed by cardiac magnetic resonance imaging, using measurements of myocardial longitudinal relaxation time T1-mapping (three studies) (15,50,55), or measurements of late gadolinium enhancement (one study) (49) (Table 1). The fibrotic pulmonary diseases included IPF (idiopathic pulmonary fibrosis) (two studies) (14,56) and chronic hypersensitivity pneumonitis (CHPP) (one study) (48) (Table 1). IPF and CHPP were diagnosed based on lung biopsy and computed tomography, according to the American Thoracic Society criteria (14,48,56) (Table 1).
The results of studies investigating the association of hypothyroidism with liver fibrosis were combined in a meta-analysis. The studies that were included in the meta-analysis used logistic regression to evaluate ORs. Due to the heterogeneity in methodology or differences in the assessment of fibrotic diseases, we could not perform quantitative meta-analyses for the following: (I) studies investigating the association of thyroid parameters with liver fibrosis; (II) studies on myocardial fibrosis; and (III) studies on pulmonary fibrosis.
Liver fibrosis
Eleven studies investigated the association of thyroid status and/or thyroid parameters with liver fibrosis (Table 1). Of these, we identified seven studies investigating the association of thyroid parameters (TSH, fT4, fT3) with liver fibrosis (12,35,44,47,51,52,54) (Table 3). In the general population, increasing TSH levels were associated with higher odds of liver fibrosis (OR, 1.49; CI, 1.04–2.15 per 1 log TSH) (12) (Table 3). In euthyroid subjects, some studies reported no association of thyroid function with liver fibrosis (12,35,44,54) and others reported an association of increasing TSH levels with liver fibrosis (47,51) (Table 3). We also identified one study investigating subclinical hyperthyroidism and liver fibrosis, but without finding an association (OR, 0.80; CI, 0.04–3.91) (12). Furthermore, we identified studies investigating the association of overt hypothyroidism (five studies) (12,36,45,46,53), and subclinical hypothyroidism (three studies) (12,44,51) with liver fibrosis (Table 2).
Based on the results of the meta-analysis, the presence of hypothyroidism was associated with a higher risk of liver fibrosis compared with euthyroidism (pooled OR, 2.48; CI, 1.87–3.29; heterogeneity I 2 = 0%) (Fig. 2A). In particular, clinical and subclinical hypothyroidism was associated with a higher risk of liver fibrosis compared with euthyroidism (pooled OR, 2.82; CI, 1.95–4.07; heterogeneity I 2 = 31.4%; pooled OR, 2.12; CI, 1.45–3.12; heterogeneity I 2 = 0%; respectively) (12,36,44 –46,51,53) (Fig. 2B, C).

Forest plots for the association of hypothyroidism with liver fibrosis. (

Sensitivity analyses using random-effects models provided similar estimates (pooled OR for overt hypothyroidism, 2.81; CI, 1.74–4.53; pooled OR for subclinical hypothyroidism, 2.12; CI, 1.45–3.12) (Fig. 2B, C). After sensitivity analyses removing one by one the studies from the analyses, the results did not change substantially (pooled OR for overt hypothyroidism varying from 2.40 [1.52–3.78] to 3.19 [2.16–4.70]; pooled OR for subclinical hypothyroidism varying from 2.10 [1.28–3.43] to 2.16 [1.37–3.41]). After removing the study reporting unadjusted estimates (36), the association of overt hypothyroidism with liver fibrosis became stronger and the heterogeneity was eliminated (pooled OR, 3.19; CI, 2.16–4.70; heterogeneity I 2 = 0%). The studies that included patients with overt hypothyroidism being treated with thyroid hormones (36,45,46,53) reported smaller ORs (pooled OR, 2.68; CI, 1.84–3.92) compared with the study that excluded thyroid medication users (OR, 6.64; CI, 1.04–23.95) (12). The association of overt hypothyroidism with liver fibrosis was stronger in the studies recruiting participants from the outpatient clinic or general population (pooled OR, 3.06; CI, 1.56–6.0) (12,36,46,53) compared with the study that included hospitalized patients (OR, 2.30; CI, 1.20–4.0) (45). The exclusion of the prospective study (12) from the analyses resulted in slightly smaller estimates for overt hypothyroidism (pooled OR, 2.68; CI, 1.84–3.92) and subclinical hypothyroidism (pooled OR, 2.12; CI, 1.17–4.01).
Myocardial fibrosis
Four studies investigated the association of hypothyroidism and/or thyroid parameters with myocardial fibrosis (15,49,50,55) (Table 1). Of these, three studies consistently showed that overt and subclinical hypothyroidism is associated with a higher degree of diffuse fibrosis than euthyroidism (Table 2) (15,50,55). Two studies showed a positive correlation of TSH (correlation coefficients varying from 0.49 to 0.52) and a negative correlation of fT4 (correlation coefficients −0.48 for both studies) with myocardial fibrosis (50,55), whereas another study did not find an association (49) (Table 3). Three studies showed a negative correlation of fT3 with myocardial fibrosis (15,49,55) (Table 3).
Pulmonary fibrosis
Three case/control studies investigated the association of hypothyroidism with fibrotic diseases of the lung (14,48,56) (Table 2). Overt hypothyroidism was associated with a 2.70 and 2.39 times higher odds of IPF and CHPP than euthyroidism, respectively, after adjusting for potential confounders such as body mass index, smoking, diabetes, and corticosteroid use (14,48) (Table 2). Subclinical hypothyroidism was associated with a 8.58 times higher odds of IPF than euthyroidism, but the estimate was unadjusted for potential confounders (56) (Table 2).
Quality assessment
Study bias assessment scores are shown in Table 4. A total of 5 studies scored 5/9 stars, 6 studies scored 6/9 stars, 5 studies scored 7/9 stars, and 2 studies scored 8/9 stars (Table 4). Of the 18 included studies, 8 studies were rated as “poor quality,” 6 studies were rated as “fair quality,” and 4 studies were rated as “good quality” (Table 4).
Assessment of publication bias
The funnel plots for the association of hypothyroidism, overt hypothyroidism, and subclinical hypothyroidism with liver fibrosis are shown in Supplementary Figure S1. The Egger test did not indicate significant funnel plot asymmetry (p-values, 0.9, 0.5, and 0.3, respectively) and thus provided no evidence of publication bias, although it should be noted that a maximum of seven studies were included.
Discussion
This systematic review and meta-analysis summarize the current evidence regarding the role of thyroid function on fibrosis of the liver, heart, and lung in humans. Overall, low thyroid function was associated with increased likelihood of fibrosis of the liver, heart, and lung. The association was consistent, irrespective of the diverse study populations, methodologies, and fibrosis locations. The risk of bias of included studies was low to moderate to high.
Overt hypothyroidism was generally associated with higher likelihood of fibrosis compared with subclinical hypothyroidism, suggesting a dose/response relationship. The magnitudes of the associations differed across studies, which may be attributable to the differences in population characteristics, fibrosis locations, fibrosis assessment, and definitions of hypothyroidism used across studies. In general, studies that excluded thyroid medication users (12,44) reported larger effect estimates compared with the studies that included hypothyroid patients treated with thyroid hormone replacement therapy (14,45,46,48). In the latter group, it is possible that levothyroxine treatment may have reduced the risk of fibrosis, further resulting in an underestimation of the observed associations. The heterogeneity among studies examining the association of overt hypothyroidism with liver fibrosis was eliminated after removing the study by Mazo et al. (36). In this study, the lack of adjustment for confounders and the administration of levothyroxine may have led to an underestimation of the observed associations (36). Studies examining thyroid parameters generally concluded that increasing TSH levels were associated with higher likelihood of fibrosis (12,47,50). Even in euthyroid subjects, low-normal thyroid function tended to be associated with increased likelihood of fibrosis, although sometimes not statistically significant (12,44,47). This could be explained by insufficient sample sizes or by a lesser fibrotic response of low-normal thyroid function compared with low thyroid function.
The results of this systematic review of observational studies in humans are also supported by previous case reports and experimental studies (57 –61). Case series and case reports in humans have indicated a co-occurrence of hypothyroidism and fibrotic diseases of the liver, heart, and lung (57 –59). The diffuse myocardial injuries among patients with overt hypothyroidism were reversed by restoring euthyroidism with short-term levothyroxine treatment (60). In patients with severe hypothyroidism, the radiologic abnormalities suggestive of lung fibrosis were also reversed after receiving thyroid hormone replacement therapy (61). Furthermore, several animal studies suggested that fibrosis of the liver, heart, and lung can be promoted by hypothyroidism and can be reversed by the administration of thyroid hormones (17,18,20,24,27,62).
Several mechanisms can explain the association of thyroid function with fibrotic diseases, including alterations in collagen gene expression, collagen deposition, activity of fibrogenic cytokines, and redox balance (13,19 –25,63). Fibrotic diseases of the liver, heart, and lung share the common histological feature of extracellular matrix accumulation (64). Experimental hypothyroidism can lead to fibrosis via upregulation of the collagen type I gene expression (13,19,20), whereas thyroid hormone administration reduces collagen type I gene expression (22,24,25). Thyroid hormones also enhance the matrix metalloproteinase activity, further resulting in a collagen breakdown (65). The transforming growth factor beta (TGFβ), a potent fibrogenic cytokine, is additionally involved in the development of hepatic, myocardial, and pulmonary fibrosis (21,23,66,67). In hypothyroid patients, TGFβ triggers intracellular changes in SMAD proteins, which enter the nucleus, promoting collagen transcription and fibrosis (23). Thyroid hormones, on the contrary, antagonize the progression of fibrosis via inhibiting the TGFβ/SMAD-dependent transcriptional activation (23). Thyroid hormone receptors may play a key role in mediating the aforementioned effects of thyroid hormones on hepatic, myocardial, and pulmonary fibrosis (13,23,27). In experimental studies, thyromimetic compounds selective for thyroid hormone receptors have shown antifibrotic properties, whereas genetically ablated thyroid hormone receptors resulted in the development of fibrosis (13,23,27). Mitochondrial dysfunction is another mechanism that can explain the link between thyroid function and fibrosis (68,69). Hypothyroidism has been associated with mitochondrial dysfunction and increased production of reactive oxygen species, which contribute to cell apoptosis and fibrosis (68,69). This can be opposed by thyroid hormones, which improve mitochondrial function and attenuate oxidative stress (68 –70). Furthermore, it may be speculated that autoimmune processes underlying hypothyroidism contribute to the development of fibrosis in the liver, heart, and lung. Several studies in this systematic review reported that hypothyroid patients with Hashimoto's thyroiditis had a higher likelihood of fibrotic diseases compared with euthyroid subjects (15,50,55). However, none of the studies addressed whether the link between hypothyroidism and fibrotic diseases is independent of thyroid peroxidase antibodies or antithyroglobulin antibodies. Besides the shared pathways linking thyroid function to fibrosis of the liver, heart, and lung, underlying organ-specific mechanisms can play an additional role. For example, a hypothyroid state is associated with dyslipidemia, insulin resistance, and obesity, which in turn promote the development of liver steatosis that can eventually progress to cirrhosis (71 –73). Moreover, hypothyroidism-associated lung fibrosis could be due to hypoxia, which improves when hypothyroidism is treated (27).
One could also hypothesize that health-related problems underlying fibrotic diseases affect thyroid parameters. Severe illnesses (e.g., sepsis, hypoxia, chronic illnesses) may result in “nonthyroidal illness,” a condition that is characterized by normal or low-normal serum TSH, low serum fT3, and low serum fT4 levels (74). Although the exact mechanisms underlying nonthyroidal illness remain unclear, poor health states can stimulate a dysregulation of the hypothalamus/pituitary/thyroid axis and alterations in the expression of thyroid hormone receptors, transporters, or deiodinases, which can eventually lead to changes in thyroid hormone levels. The results of this systematic review, however, are not likely explained by nonthyroidal illness, because the included studies were not performed in critically ill populations. The studies that were performed in hospitalized populations usually excluded the patients with chronic and decompensated conditions. The other studies were conducted in relatively healthy participants from the general population or outpatient clinics.
To the best of our knowledge, this is the first systematic review, which combines the literature regarding the role of thyroid function on fibrosis of the liver, heart, and lung in humans. In accordance with the NOS, we used strict criteria for the quality assessment of the risk of bias. Most of the included studies adjusted for potential confounders, including age and sex. Another strength is the consistency of the results in the setting of diverse study populations. The wide range of ages (mean age ranging from 36 to 69) and ethnicities of participants may increase the generalizability of our conclusions. Furthermore, we were able to perform summary statistics and combine the available evidence on hypothyroidism and liver fibrosis in a meta-analysis. Sensitivity analyses provided consistent estimates. No evidence of publication bias was observed.
Several limitations of this systematic review warrant consideration. Most of the included studies were characterized by a cross-sectional design; therefore, we cannot exclude the possibility of reverse causation or bidirectional associations. The results of cross-sectional studies in this systematic review, however, were in line with the results of the prospective study (12), suggesting a temporal association between low thyroid function and fibrosis risk. Additional evidence from experimental studies supports more strongly an effect of hypothyroidism on fibrotic diseases rather than vice versa (17,18,20,24,27). Another limitation of this systematic review is that the included studies used several definitions of thyroid dysfunction and different measures of fibrotic outcomes. Nevertheless, results were overall consistent. The studies defining thyroid status based on thyroid function measurements did not have data available with regard to variations in thyroid function over time. Furthermore, the limited number of identified studies illustrates the scarcity of evidence on this topic, especially for myocardial and pulmonary fibrosis.
Future population-based studies examining the association of thyroid dysfunction (i.e., hypothyroidism and hyperthyroidism) with the risk of fibrotic diseases should preferably be characterized by a prospective design and a long-term follow-up period. Adequately powered studies are also needed to clarify whether the risk of fibrosis is affected by the fluctuations within the reference range of thyroid function. Of importance, future randomized clinical trials are warranted to simultaneously examine the potential beneficial effects of thyroid hormone supplementation on fibrosis of the liver, heart, and lung. These investigations could eventually promote the development of new therapies against fibrotic diseases. In addition, thyroid disease may also play a role in the development of other fibrotic processes, including idiopathic retroperitoneal fibrosis, primary biliary cirrhosis, and skin fibrosis; but the amount of current evidence is very limited and further research is needed (23,75,76). Given the systemic effects of thyroid hormones, future studies may also consider investigating the association of thyroid function with the risk of concomitant fibrotic processes in multiple organs. Finally, future observational and experimental studies need to provide additional insights on the shared and organ-specific mechanisms linking thyroid function to fibrosis of the liver, heart, and lung, using mediation analyses and interventional approaches. In particular, it remains uncertain whether the link between thyroid function and fibrotic diseases is independent of thyroid autoimmunity, hypoxia, and chronic illnesses. Given the complexity of the mechanisms underlying fibrosis, future studies may need to unravel the interplay of thyroid hormones with inflammatory, hormonal, metabolic, immune, environmental, genetic, and other putative risk factors of fibrotic diseases.
In conclusion, our findings suggest that low thyroid function is associated with an increased likelihood of chronic fibrotic diseases of the liver, heart, and lung in humans. Results were consistent in the setting of diverse study populations. Given the limited amount of prospective evidence on this topic, our study highlights the need for future prospective studies and randomized clinical trials investigating the potential efficacy of thyroid hormone and its analogs on the development of fibrosis. This could eventually lead to the development of novel strategies for the prevention and treatment of fibrotic diseases.
Footnotes
Acknowledgments
We thank the librarians from the Walton Library of Newcastle University and the librarians from the Medical Library at the University of Bern for their assistance with the online literature search. A.B. was supported by an exchange fellowship from the European Thyroid Association.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
R.P.P. is supported by the Netherlands Organization for Health Research and Development Zon-MWTOP grant 91212044 and an Erasmus Medical Center Medical Research Advisory Committee grant. R.P.P. has received lecture fees from IBSA and Goodlife Fertility. The funding sources had no role in the selection, critical appraisal, or synthesis of evidence.
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
Supplementary Appendix Figure S1