
Abstract
Purpose:
To systemically investigate the prognostic value of pre-ablation stimulated thyroglobulin (s-Tg) in children and adolescents with differentiated thyroid cancer.
Methods:
Clinical records from 118 children and adolescents were retrospectively reviewed.
Results:
The median age was 16 years, and the majority were female (79.7%). All children and adolescents underwent total thyroidectomy and received radioactive iodine therapy. After a median follow-up of 5.3 years, 68 (57.6%) patients were disease free, while 50 patients (42.4%) had persistent/recurrent disease. In multivariate analysis, pre-ablation s-Tg and M1 were the independent predictive factors for persistent/recurrent disease. According to the receiver operating curve analysis, the best pre-ablation s-Tg cutoff to predict disease-free status was 17.8 ng/mL with a negative predictive value of 96.8%. Integration of pre-ablation s-Tg into American Thyroid Association pediatric risk categories indicated that the presence of pre-ablation s-Tg ≤17.8 ng/mL was associated with a decreased chance of having persistent/recurrent disease in intermediate- and high-risk patients (22.6% to 2.6% in intermediate-risk patients, and 64.4% to 5.6% in high-risk patients).
Conclusions:
Our findings suggest that pre-ablation s-Tg has the capability of predicting the clinical outcomes in children and adolescents with thyroid cancer.
Introduction
Thyroid cancer is the most common endocrine malignancy in children and adolescents. An increased incidence of childhood thyroid cancer over the past decades has been reported worldwide (1). Children and adolescents with thyroid cancer generally present with more advanced disease at diagnosis with regional lymph node metastasis in 40–90% and distant metastasis in 20–30% of children and adolescents.
Typical therapy for children and adolescents with thyroid cancer is total thyroidectomy with adjuvant radioactive iodine-131 (131I) to ablate the residual thyroid cancer or its local or distant metastasis. The prognosis in children and adolescents with thyroid cancer is excellent, with a 10-year mortality of <10% and overall survival of 98%; at 20 years, overall survival is 95% (2,3). It is, therefore, important to identify independent biological parameters to predict clinical outcomes and to help tailor the initial therapy and follow-up intensity to avoid overtreatment.
Historically, serum stimulated thyroglobulin (s-Tg) is a reliable marker for detecting persistent and recurrent disease during the follow-up of thyroid cancer patients who have already been treated with 131I. Recent research has demonstrated the utility of postoperative pre-ablation s-Tg for predicting disease-free status in thyroid cancer patients. A low postoperative pre-ablation s-Tg has been proved to be a good predictor of long-term remission. In a meta-analysis involving nearly 4000 thyroid cancer patients, the overall negative predictive value (NPV) of pre-ablation s-Tg is reported to be as high as 94% with a cutoff value of 10 ng/mL (4). It should be emphasized that currently available evidence about NPV of pre-ablation s-Tg is predominately derived from studies of adult populations. In addition, there is emerging literature (5,6) that suggests a significant difference in pre-ablation s-Tg levels between children and adults, even with a similar disease burden.
The recently published American Thyroid Association (ATA) guidelines for the treatment of children and adolescents with thyroid cancer specifically recommend measurement of postoperative s-Tg for intermediate- and high-risk patients (7). However, the utilities of pre-ablation s-Tg in the postoperative management of children and adolescents with thyroid cancer are poorly studied. The aim of this study was to systematically determine the prognostic value of postoperative pre-ablation s-Tg in a contemporary differentiated thyroid cancer cohort of children and adolescents attending a referral center hospital in southwestern China.
Materials and Methods
Patients
This observational retrospective study was conducted to analyze the clinical, morphological, and biological data for children and adolescents with differentiated thyroid cancer in our tertiary center between January 2009 and December 2017; this cohort continues to be followed. The institution is a tertiary-care university teaching hospital in southwestern China and is a referral center for thyroid cancer treatment. The study was approved by the local Institutional Review Board of West China Hospital, Sichuan University and the requirement of written informed consent was waived.
At our thyroid center, thyroid cancer patients, except those with well-differentiated cancer measuring 1 cm or less confined to the thyroid gland, underwent total thyroidectomy with central or lateral neck dissection, depending on risk and intraoperative findings, and a subsequent 131I ablation. On the basis of clinical and surgical histopathological information, each patient was initially staged by using the 7th edition of the AJCC/UICC staging system. T (the extent of the primary tumor) and N (regional lymph node metastasis) were assessed on the basis of the histopathological description, while M (distant metastasis) was assessed according to the first post-therapy whole body 131I scintigraphy and other imaging methods if available. The assignment of ATA risk of recurrence category followed the ATA pediatric risk stratification system (7).
All children and adolescents had undergone a total thyroidectomy, followed by a complementary 131I ablation. All operations were performed by two experienced thyroid surgeons (both with 10 years of experience in thyroid surgeries). A detailed postoperative evaluation of the disease status with neck ultrasound and s-Tg measurements was systematically decided by a multidisciplinary thyroid cancer board. An empiric activity dosing protocol was utilized to determine the prescribed activity of 131I. For prepubertal patients, activity was administered on a weight basis (50–100 MBq/kg). Activity administered after puberty ranged from 3.7 to 7.4 GBq (3.7 GBq for simple remnant ablation, 5.5–7.4 GBq for postoperative residual neck lymph node metastasis or concurrent distant metastasis).
Pre-ablation s-Tg measurements
All pre-ablation s-Tg and anti-Tg autoantibody (TgAb) levels were measured with the same high-sensitive electrochemiluminescence immunoassay after thyroid hormone withdrawal and just before the adjuvant 131I administration at the same laboratory in our hospital. The assay used was the Roche Elecsys 2010 system (Roche Diagnostics GmbH, Mannheim, Germany), which was calibrated against the CRM-457 standard. This method provided a sensitivity of 0.04 ng/mL and a reference range of 0.5–55 ng/mL. Sera showing TgAb levels more than 40 IU/mL were excluded from the study (8). Quality control was ensured by assaying two levels of control sera in each series and by re-assessing all sera showing a coefficient of variation exceeding 10%. A full description of s-Tg and TgAb measurements and the quality control has been previously published (9).
Follow-up
All patients were usually followed every 6 months during the first year and at 6–12 month intervals thereafter at the discretion of the attending physician on the basis of the risk of the individual patient and the clinical course of the disease. When patients were not cured, further treatments (131I therapy, repeated surgery, or other therapies) were carried out.
Definitions of clinical outcomes
Patients were considered to have an excellent response to therapy or long-term remission at final follow-up if they had a suppressed Tg <1 ng/mL, no detectable TgAb, and no structural evidence of disease (10,11). Patients with s-Tg >10 ng/mL; suppressed Tg >1 ng/mL; or any evidence of disease on cross-sectional imaging (ultrasound, computed tomography scan, or magnetic resonance imaging), functional imaging (whole body 131I scintigraphy or 18-fluorodeoxyglucose-positron emission tomography scan), or biopsy-proven disease (cytology or histology) were considered as having persistent disease. Patients with persistent disease were further classified as having either biochemical evidence of disease (s-Tg >10 ng/mL, suppressed Tg >1 ng/mL, or rising TgAb without a structural correlate) or structural evidence of disease on imaging.
Patients were considered to have structural evidence of disease if any of the following conditions were met: (1) positive cytology/histology, (2) highly suspicious lymph nodes or thyroid bed nodules on the neck ultrasound (hypervascularity, heterogeneous content, cystic areas, rounded shape, or enlargement during the follow-up), or (3) findings on whole body 131I scintigraphy, 18-fluorodeoxyglucose-positron emission tomography scans, or other cross-sectional imaging highly suspicious for metastatic disease.
Any anomaly persisting during the initial evaluation was considered as disease persistence (incomplete biochemical and/or structural response). Disease recurrence was defined as the appearance of biochemical, structural, or functional evidence of disease in patients previously considered in remission (12). Recurrence-free survival (RFS) was defined as the interval of time between a patient's initial surgery and the detection of persistent/recurrent disease.
Statistical analysis
Qualitative parameters are expressed as frequencies and percentages and are analyzed by using chi-square or Fisher's exact test. Normally distributed quantitative parameters are expressed as means with standard deviation, whereas non-normally distributed parameters are expressed as median and interquartile ranges. Student t-test or the Mann–Whitney U test was used to identify the link between different quantitative parameters and disease remission. Receiver operating characteristic (ROC) curve analysis was used to define the best cutoff value for pre-ablation s-Tg. For the established cutoff value, we calculated sensitivity, specificity, positive predictive value (PPV), and NPV. The predictive value of pre-ablation Tg levels and other factors considered are assessed by using a univariate and a multivariate logistic regression model (enter method, all the variables are entered in the model in one single step). All variables significantly associated with persistent/recurrent disease are included in the multivariate analysis.
RFS plots were constructed by using the Kaplan–Meier method, and groups were compared by using log-rank tests. A p-value of <0.05 was considered statistically significant. Statistical analysis was performed by using the SPSS statistical software version 13.0 for Windows.
Results
Clinical characteristics
From January 2009 to December 2017, 172 children and adolescents with thyroid cancer were referred to our department for adjuvant 131I therapy after total thyroidectomy. After exclusion of patients with incomplete data for staging or recurrence risk (n = 5), those with thyrotropin (TSH) <30 μIU/mL (n = 4), and those with positive TgAb (n = 45), the remaining 118 children and adolescents constituted our study cohort (Fig. 1).
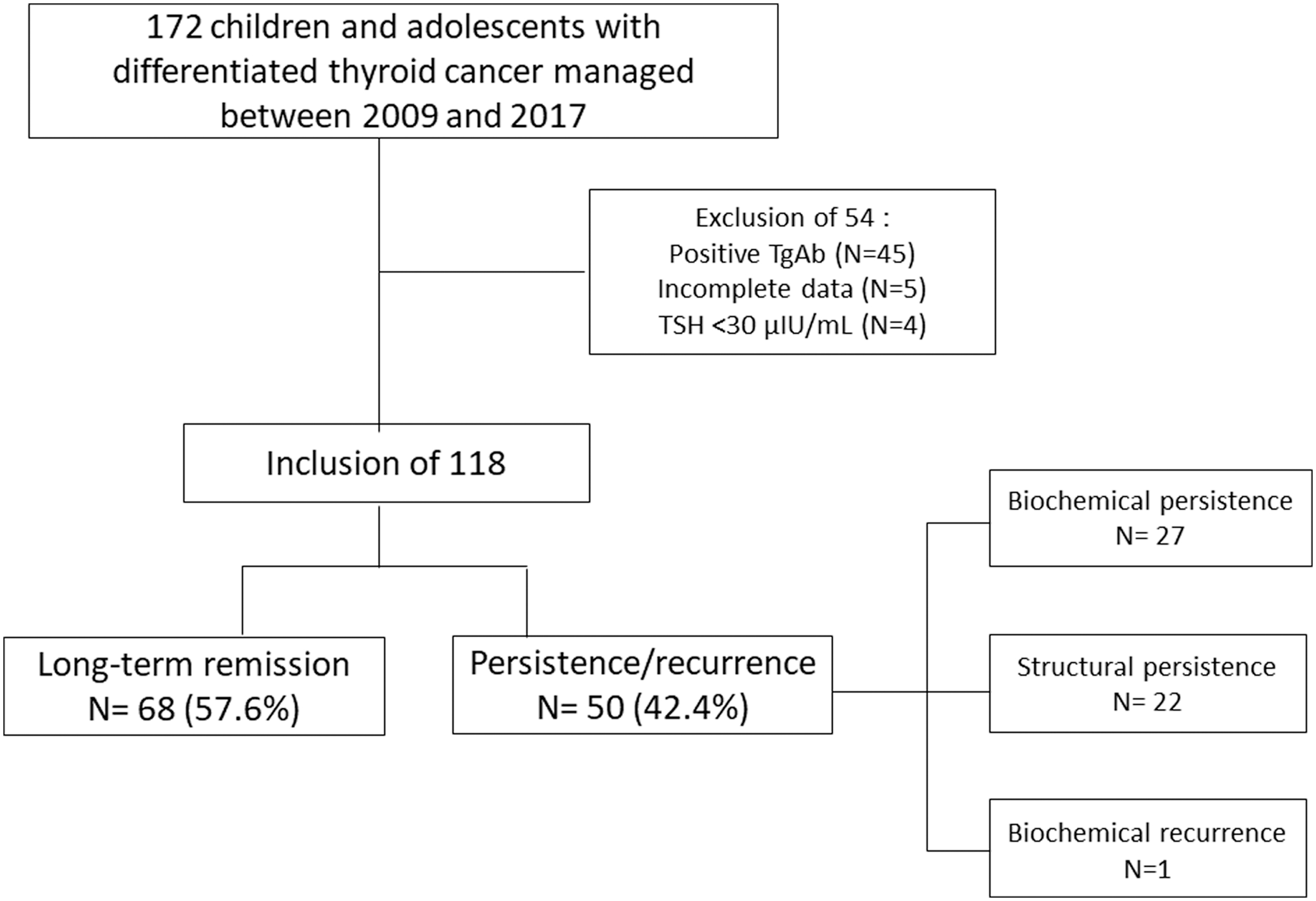
Initial children and adolescent selection, occurrence of recurrence during follow-up.
Total thyroidectomy was performed in all patients. Thirty-seven patients (31.4%) underwent central neck dissection, and 81 (68.6%) underwent central and lateral neck dissection. The median age was 16 years, 26.3% (31 patients) were less than 15 years old at diagnosis, and the majority were female (79.7%). There were 112 patients with classic papillary thyroid cancer, 3 with follicular variant of papillary thyroid cancer, 1 with diffuse sclerosing variant of papillary thyroid cancer, and 2 patients were diagnosed with follicular thyroid cancer.
The median tumor size was 3.0 cm (range, 0.1–8.0 cm). Cervical lymph node metastases were identified in 104 (88.1%) patients, and metastases confined to the lungs were identified in 32 (27.1%) patients. Regarding TNM staging, 86 (72.9%) were classified as stage I, and 32 (27.1%) as stage II. On ATA pediatric risk stratification, 6 (5.1%) were low risk, 53 (44.9%) were intermediate risk, and 59 (50.0%) were high risk. The relatively high proportion of patients classified as having high risk (50.0%) probably reflects the selection bias of patients referred to our tertiary care center. The main characteristics of the study cohort are described in Table 1.
Baseline Characteristics of Children with Differentiated Thyroid Cancer
TNM staging is determined by the 7th American Joint Cancer Committee TNM stage system.
Indicates that information about that characteristic was not available.
DSV-PTC, diffuse sclerosing variant PTC; FTC, follicular thyroid cancer; FV-PTC, follicular variant PTC; LN, lymph node; LND, lymph node dissection; PTC, papillary thyroid cancer; s-Tg, stimulated thyroglobulin; SD, standard deviation; TSH, thyrotropin; TT, total thyroidectomy.
Clinical outcomes
After a median follow-up of 5.3 years (range, 1.0–10.1 years), 68 children and adolescents (57.6%) had achieved long-term remission or excellent response to therapy. A total of 50 children and adolescents (42.4%) had persistent/recurrent disease at final follow-up, the majority had a biochemical incomplete response (n = 27; 22.9%), 18.6% (n = 22) had a structural incomplete response, and only 0.8% (n = 1) had a biochemical recurrence (Fig. 1). Of the 22 children and adolescents with structural incomplete response, diseases persisted in cervical lymph nodes (n = 4), in the lungs (n = 12), and in both (n = 6). There were no deaths related to this cancer during follow-up.
Predictors of persistent/recurrent disease after initial therapy at univariate and multivariate analyses
To investigate factors associated with persistent/recurrent disease at follow-up, children and adolescents were grouped into disease-free or persistent/recurrent disease categories. Applying univariate analysis, age, tumor size, TNM staging, the ATA pediatric risk stratification system, cumulative 131I-administered activity, and pre-ablation s-Tg levels were identified as predictors of persistent/recurrent disease (Table 2).
Univariate Analysis of Predictors of Persistent/Recurrent Disease
ATA, American Thyroid Association.
On multivariate analysis, both pre-ablation s-Tg and M1 were patient features independently predicting persistent/recurrent disease (odds ratio [OR] = 28.62 and 17.13, respectively, p < 0.05 for both) (Table 3).
Multivariate Analysis of Predictors of Persistent/Recurrent Disease
CI, confidence interval; OR, odds ratio.
Prognostic value of pre-ablation s-Tg
The time interval between surgery and pre-ablation s-Tg measurements was a median of 1.9 months (range, 1.1–4.5 months). All pre-ablation s-Tg measurements were obtained after thyroid hormone withdrawal. Serum TSH levels were greater than 30 μIU/mL in all patients at the time of pre-ablation s-Tg measurements with a median of 96 μIU/mL. The median value of pre-ablation s-Tg was 15.1 ng/mL (range, 0.04–4589.00), with a median of 4.82 ng/mL for patients classified as disease free, and 184.1 ng/mL for patients with persistent/recurrent disease (p < 0.001). Spearman correlation test demonstrated that there was no significant relationship between TSH and pre-ablation s-Tg levels (data not shown).
To better understand the capacity of pre-ablation s-Tg in predicting persistent/recurrent disease versus long-term remission, an ROC curve was employed, which resulted in an area under the curve of 0.94 [confidence interval (CI) 0.89–0.99]. When a cutoff value of 17.8 ng/mL was applied, we obtained a sensitivity of 88.2%, a specificity of 96.0%, a PPV of 85.7%, and an NPV of 96.8%. The same cutoff was appropriate for both intermediate-risk (NPV = 97.4%) and high-risk children and adolescents (NPV = 92.7%) (data not shown).
Integrating pre-ablation s-Tg with ATA pediatric risk categories
When we stratified children and adolescents according to ATA pediatric initial risk stratification, persistent/recurrent disease was found in 0 (0%) of 6 low-risk patients, in 12 (22.6%) of 53 intermediate-risk patients, and in 38 (64.4%) of 59 high-risk patients during follow-up. The impact of low pre-ablation s-Tg on clinical outcomes was most prominent in children and adolescents initially classified as high risk of recurrence (Table 4). In these patients, the presence of pre-ablation s-Tg ≤17.8 ng/mL resulted in a significant decrease from a 64.4% to 5.6% likelihood of having persistent/recurrent disease. By contrast, the presence of a pre-ablation s-Tg >17.8 ng/mL was associated with an increased risk of having persistent/recurrence disease in intermediate- and high-risk patients (22.6% to 73.3% in intermediate-risk patients, and 64.4% to 90.2% in high-risk patients).
Re-stratification of American Thyroid Association Pediatric Risk Category According to the Pre-Ablation s-Tg Levels
As shown in Kaplan–Meier curves for RFS, RFS rates were 100% in the low-risk group, 72.8% in the indeterminate-risk group, and 33.2% in the high-risk group (Fig. 2A). When we integrated pre-ablation s-Tg with ATA pediatric risk categories (Fig. 2B), both intermediate- and high-risk patients with pre-ablation s-Tg ≤17.8 ng/mL had excellent RFS (97.4% and 94.1%, respectively). However, intermediate-risk patients with pre-ablation s-Tg >17.8 ng/mL had a poorer RFS at 22.2%, and high-risk patients had the worst RFS at 9.2% (p < 0.001).
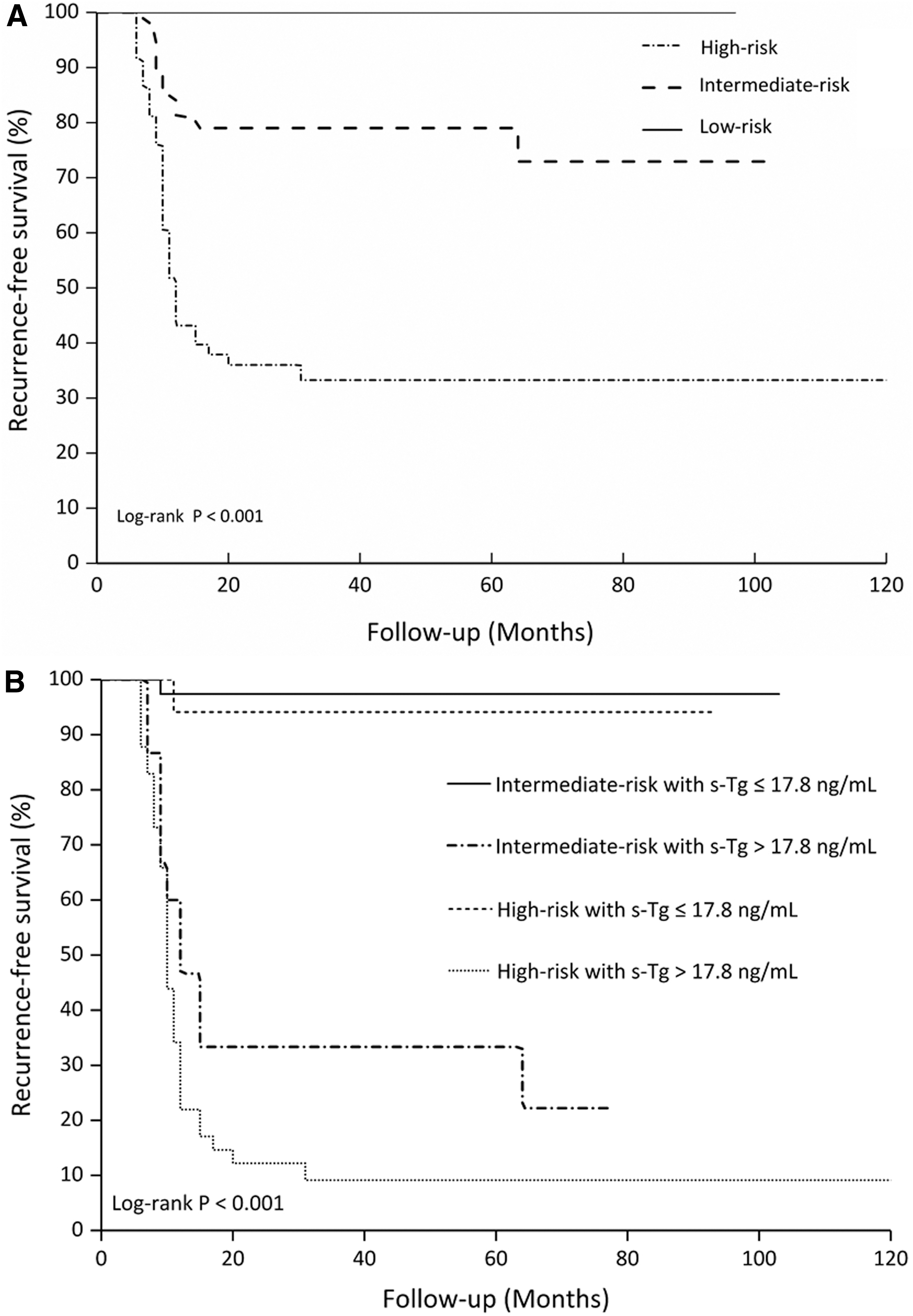
Kaplan–Meier curves for persistent/recurrent disease in children and adolescents with thyroid cancer according to (
Discussion
A few studies (5,6,13,14) have examined the utilities of pre-ablation s-Tg in the postoperative management of children and adolescents with thyroid cancer. Two studies investigated the value of pre-ablation s-Tg in identifying distant metastasis at the time of 131I ablation. The reported cutoff value of pre-ablation s-Tg was quite similar between the two studies, ∼156 ng/mL (5,6). In a study on parameters influencing success of postoperative 131I ablation in a population of young Belarusian patients with advanced thyroid cancer, pre-ablation s-Tg was identified to be an independent and significant variable. Recently, Zanella et al. (14) reported on 17 children and adolescents with thyroid cancer and evaluated the potential prognostic value of pre-ablation s-Tg. Both the sensitivity and specificity of pre-ablation s-Tg to predict disease-free status were demonstrated to be 100% with a cutoff value of 31.5 ng/mL.
In this study, we systematically investigated the prognostic implications of postoperative pre-ablation s-Tg that was obtained as early as a few weeks after surgery in a cohort of 118 consecutive children and adolescents with thyroid cancer who had been treated with total thyroidectomy and 131I ablation. Our results show that the pre-ablation s-Tg was an independent predictor of disease long-term remission in children and adolescents with thyroid cancer. At a cutoff value of 17.8 ng/mL, an NPV of pre-ablation s-Tg arrived at 96.8%. This holds true whether the patient was initially classified as intermediate- or high risk.
The ATA pediatric risk categories (low, intermediate, and high) use well-established and validated criteria to identify thyroid cancer patients who are likely to have better or worse clinical outcomes (10,15). Nevertheless, the risk of persistent/recurrent disease is a continuum that ranges from very low to very high, even within the three primary risk categories. Our study demonstrates that integration of pre-ablation s-Tg into ATA pediatric initial risk categories provides a more individualized estimate of clinical outcomes in children and adolescents with thyroid cancer. In our cohort, persistent/recurrent disease was found in 12 (22.6%) of 53 intermediate-risk children and adolescents, and in 38 (64.4%) of 59 high-risk children and adolescents during follow-up. However, this frequency was reduced to 2.6% and 5.6%, respectively, among intermediate- and high-risk children and adolescents with a postoperative pre-ablation s-Tg ≤17.8 ng/mL. Interestingly, similar phenomena were noted in studies of adult patients with thyroid cancer. Rosario et al. (8) studied the frequency of tumor recurrence in 181 thyroid cancer patients initially classified as intermediate risk with postoperative pre-ablation s-Tg <2 ng/mL. During the 5-year period of follow-up after 131I ablation, persistent/recurrent disease occurred in only 3.3% of cases. In a cohort of 69 high-risk thyroid cancer patients with pre-ablation s-Tg <1 ng/mL who had received total thyroidectomy and 131I ablation, Tian et al. (16) found that only two patients (2.9%) experienced disease recurrence at a median follow-up of 5.6 years. Taken together, these results, in combination with this study, suggest that thyroid cancer patients with low or undetectable postoperative pre-ablation s-Tg generally have a good prognosis irrespective of age, initial staging, and risk stratification.
On the basis of high NPV of pre-ablation s-Tg, several authors (17 –23) have proposed appropriate reduction in the intensity of therapy and follow-up in thyroid cancer patients with low or undetectable postoperative pre-ablation Tg. Orlov et al. (17) were the first to propose an innovative approach to the selection of 131I ablation on the basis of the postoperative pre-ablation s-Tg and neck ultrasound. The protocol was tested in a prospectively studied cohort of 116 low- and intermediate-risk thyroid cancer patients with postoperative pre-ablation s-Tg <5 ng/mL and negative neck ultrasound who were not referred for 131I therapy. They did not see any evidence of recurrent disease over the 6-year follow-up period. Rosario et al. (19) have prospectively studied the long-term efficacy of low activity 131I therapy in intermediate-risk thyroid cancer patients with higher risk features and postoperative non-stimulated Tg <0.3 ng/mL. On the basis of a recurrence rate of 4%, the authors concluded that low postoperative non-stimulated Tg could be used as a criterion for the indication of low 131I activity in intermediate-risk thyroid cancer patients even harboring higher risk features. Conventionally, TSH suppression therapy has been the mainstay in the postoperative management of thyroid cancer. Our recent study demonstrated that TSH suppression before the first response to treatment assessment did not influence the rate of disease recurrence in intermediate- and high-risk thyroid cancer patients with pre-ablation s-Tg <1 ng/mL (23). However, the studies mentioned earlier involved mostly adult patients (average age ranging from 44 to 51 years). Whether this finding could be applicable to pediatric patients has not yet been validated. There is a need for additional research that examines the feasibility to select children and adolescents with thyroid cancer for remnant ablation, tailor the activity of 131I administered, and the intensity of follow-up surveillance on the basis of pre-ablation s-Tg (24).
Since the low-risk thyroid cancer patients are generally not referred for 131I ablation, 95% (112/118) of our cohort were classified as being at intermediate- and high risk, in whom 131I therapy was considered essential. Regarding the clinical presentation, in this study, there was a high incidence of lymph node metastases (88.1%) and distant metastases (27.1%). Previous data (10) corroborate this finding of our study and demonstrate a high proportion of lymph node and distant metastases in children and adolescents with thyroid cancer classified as intermediate- and high risk. The intensity of initial therapy, including the extent of surgery and 131I ablation, also significantly affects the prognosis of children and adolescents with thyroid cancer. In this study, we relied on the homogeneous treatment and follow-up protocols with uniform diagnostic methods, risk assessment, and dynamic risk stratification criteria. The time of follow-up of our children and adolescents might not be considered as long enough. Nevertheless, the persistent/recurrent diseases observed in the study (∼42.4%) were comparable to previous reports (3,10,14,25) and, thus, unlikely to result in an underestimate.
Nevertheless, the study has several limitations. First, the single institution study design lends itself to selection biases that are difficult to control. Second, the included patients form a historical cohort study with a relatively small number of patients. This limitation reflects the rarity of thyroid cancer in the pediatric population. Further multicenter or larger cohort-based studies are required to examine the reliability and validity of the postoperative pre-ablation s-Tg as a predictor of clinical outcomes in children and adolescents with thyroid cancer.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.