
Abstract
Background:
Vitamin D deficiency has been proposed to have a role in the development and course of Graves' disease (GD). Muscle weakness and quality of life (QoL) impairments are shared features of GD and vitamin D deficiency. We aimed at investigating whether vitamin D supplementation would improve restoration of muscle performance and thyroid-related QoL in GD and at describing the effect of anti-thyroid medication (ATD) on these outcomes.
Methods:
In a double-blinded clinical trial, hyperthyroid patients with a first-time diagnosis of GD were randomized to vitamin D 70 μg (2800 IU)/day or matching placebo as add-on to standard ATD. At baseline and after 3 and 9 months of intervention, we assessed isometric muscle strength, muscle function tests, postural stability, body composition, and QoL-impairment by using the ThyPRO questionnaire. Linear mixed modeling was used to analyze between-group differences. (The DAGMAR study
Results:
Nine months of vitamin D supplementation caused an attenuation of muscle strength increment in all muscle measures investigated, significant at knee extension 60° where the increase was 24% lower (p = 0.04) in the vitamin D group compared with placebo. Compared with placebo, vitamin D supplementation tended to reduce gain of lean body mass (−24%, p = 0.08). Vitamin D supplementation significantly impeded alleviation of Composite QoL and the same trend was observed for the Overall QoL-Impact and Impaired Daily Life scales. In response to ATD, all measures improved significantly. The increase in muscle strength ranged from 25% to 40% (p all < 0.001), and increment of lean body mass was 10% (p < 0.001). Large changes were observed in all QoL scales.
Conclusions:
Nine months of vitamin D supplementation caused unfavorable effects on restoration of muscle performance. In contrast, ATD treatment was associated with marked improvement in all measures of muscle performance and thyroid-related QoL. In patients with newly diagnosed GD, high-dose vitamin D supplementation should not be recommended to improve muscle function, but ATD is of major importance to alleviate muscle impairment.
Introduction
Among the numerous symptoms of Graves' disease (GD), muscle weakness and quality of life (QoL) impairments are prominent features (1). The reduction in muscle strength has been demonstrated in a number of studies and complaints of muscle symptoms are reported by the majority of patients (2,3). Due to the abundance of somatic as well as mental symptoms in GD, a negative effect on QoL is not surprising and a marked impairment of QoL at diagnosis is common (4). A recent large cross-sectional study suggested that QoL impairments are present even years after initial treatment (5).
Several lines of evidence support an effect of vitamin D on muscle tissue and function. In cross-sectional studies, lower levels of 25-hydroxyvitamin D [25(OH)D] were associated with lower muscle strength (6). In observational studies, vitamin D deficiency was associated with poor muscle strength and low physical performance and its decline (7,8). GD is associated with lower levels of 25(OH)D (9 –11). However, the effect of supplemental vitamin D on muscle strength and QoL in GD has not previously been investigated. We aimed at investigating whether vitamin D supplementation improves recovery of muscle performance and QoL in GD and secondarily at describing the change in these outcomes in response to anti-thyroid medication (ATD).
Methods
This study was a randomized, double-blinded, parallel-group trial on the effects of 9 months of cholecalciferol versus placebo given as add-on supplementation to standard ATD in patients newly diagnosed with GD. Participants were recruited from the outpatient clinics at Aarhus University Hospital and the regional hospitals of Central Denmark Region. Patients were enrolled in March 2015 through December 2016 and follow-up was completed by September 2017.
Inclusion criteria were age between 18 and 80, a first-time diagnose of GD, hyperthyroidism at first visit, and initiated or planned ATD as the treatment of choice. Hyperthyroidism was defined as thyrotropin (TSH) levels below the lower limit of the reference range with total or free levels of triiodothyronine (T3) and/or thyroxine above the upper limit of the reference range, and an elevated level of thyroid stimulating hormone receptor antibody (TRAb). Exclusion criteria were previous hyperthyroidism, and comorbidity of chronic granulomatous disease, hypercalcemia (ionized calcium >1.40 mmol/L), impaired kidney function (estimated glomerular filtration rate [eGFR] <45 mL/min), or presence of malignant disease. Further, we excluded patients who were pregnant, who were treated with immunomodulatory drugs, who had a daily intake of more than 10 μg of chole- or ergo-calciferol that could not be discontinued (no washout phase), or who were unable to read and speak Danish. All participants were enrolled in the DAGMAR study (Vitamin D And Graves' disease: Morbidity and Relapse Reduction) aiming at assessing the effects of vitamin D supplementation on the course of GD (
Intervention
Participants were randomly allocated (in a ratio of 1:1) to 9 months of treatment with 70 μg/day (2800 IU) cholecalciferol or matching placebo prescribed as one daily tablet at mealtime. Treatment allocation was performed by the Pharmacy Department Central Denmark Region by using a computer program (
Investigations
All participants received ATD treatment according to local standard practice. All participants underwent clinical examination at baseline, at 3 and at 9 months including blood sampling, isometric muscle strength examination, muscle function tests, and measuring of postural stability. At baseline and 9 months, measurement of body composition was performed. Physical activity was assessed by using the Physical Activity Scale (PAS) questionnaire at each study visit (13). Health-related QoL was evaluated by using the ThyPRO-39 questionnaire at baseline, at 6 weeks, and at 3, 6 and 9 months (14). Additional questions on socio-demographics, musculo-skeletal symptoms, comorbidity, and medication were included at baseline, 3 and 9 months. New questionnaires were sent to non-responders after 5 and 10 days (by email) or after 1 and 2 weeks (by mail).
Muscle strength
Muscle strength was measured by using an adjustable dynamometer chair (Good Strength; Metitur Ltd.) with high-performance reliability with correlation coefficients of 0.87–0.96 (15). The maximum voluntary isometric muscle strength (Newton) and maximum force production (N/s) were assessed by hand grip, by elbow extension and flexion at a fixed position of 90° flexion, and by knee extension and flexion at a fixed position of 60° and 90°. During all measurements, belts were used to support and position the trunk, ankle, thigh, and wrist. The measurements, performed by using the dominant hand's side, were recorded for 5 seconds and repeated three times separated by a 30-second break. The best performance was chosen for analysis. The chair adjustments and belt positions of ankle and wrist were recorded and repeated at follow-up visits.
Postural stability
Postural stability was assessed by using a stadiometer (Good Performance Platform System; Metitur Ltd.). The procedure has previously been described (3). Measurements were performed in four settings: (1) normal standing with parallel feet 20 cm apart and eyes open, (2) normal standing eyes closed, (3) semitandem during which the heel of the non-dominant hand's side foot is placed beside the big toe on the other foot and eyes are open, and (4) tandem standing during which the non-dominant hand's side foot is placed in front of the toes of the other foot and eyes are open. The recording time was 20 seconds, and each exercise was repeated three times. The best of three performances (the lowest velocity moment) was chosen for analysis.
Muscle function tests
Two muscle function tests were performed. In the Timed-Up-And-Go (TUG) test, the participants, seated in a chair with their feet flat on the ground and their arms crossed, were asked to stand up, walk three meters in a straight line, turn around, and return to their seat as quickly as possible (16). In the Repeated Chair Stand (RCS) test, the participants, seated as described earlier, were asked to rise and sit ten times in a row as quickly as possible without the use of their arms. The time spent on each test was recorded. Both tests were performed twice or until the results of two attempts differed with <1 second. For each of the tests, the average of two attempts was used for analysis.
Body composition
Body composition was calculated from whole body scans performed in the fasting condition by using a Hologic Discovery dual-energy X-ray absorptiometry scanner (Hologic, Inc., Waltham, MA). Subtotal lean body mass and fat mass estimates refer to the whole body minus the head.
Quality of life
Using the ThyPRO questionnaire, physical symptoms of hyperthyroidism were measured by the multi-item scales from the full ThyPRO; whereas mental and social domains of functioning and well-being were measured by the abbreviated multi-items scales Tiredness, Cognitive Complaints, Anxiety, Depression, Emotional Susceptibility, Impaired Social Life, Impaired Daily Life, and Overall QoL impact from the ThyPRO-39 (17). The ThyPRO-39 scales were summarized in the ThyPRO-39 Composite Scale. All scales were scored to the standard 0–100 ThyPRO-range (17), with higher scores indicating more symptoms or impairment.
Physical activity
The PAS questionnaire is validated in moderate active Danish adults and correlates well with physical activity diaries (13). Based on metabolic equivalents (MET, 1 kcal/kg/h) allocated to each level of physical activity, the self-reported time spent on different everyday activity is transformed into a total MET-score.
Biochemistry
Blood samples were collected in the fasting state in the morning at baseline and follow-up visits. TRAb, thyroid stimulating hormone, free T3, and thyroxin (T4) were measured by electrochemiluminescence imunoassays using the Cobas 6000 analyzer (Roche). Total plasma levels of 25(OH)D [25(OH)D2 + 25(OH)D3] were analyzed by isotope dilution liquid chromatography tandem mass spectrometry with intra-assay coefficients of variation of 5.4% (at 33 nmol/L) and 10% (at 113 nmol/L). Analyses of TRAb, free T3, free T4 (at 3 and 9 months), and 25(OH)D (all study visits) were performed in batches. Blood samples for batch analyses were centrifuged at 1800 g for 10 minutes and stored at −80°C until analysis after a maximum of 40 months.
Statistical analyses
The primary outcome measure was muscle strength at 9 months versus baseline in response to intervention. Sample size calculation was based on previous observations with a mean maximum voluntary isometric muscle force at knee extension 60° of 393 N and a standard deviation (SD) of repeated measurements of 53 N (18). To detect a 10% difference in change between groups, inclusion of 30 participants in each group was needed (power 0.80; level of statistical significance 0.05). To allow for dropouts, we aimed at including 40 participants in each group.
The secondary outcome measures were lean body mass, muscle function tests, postural stability, and health-related QoL in response to intervention. Also, the effect of ATD on all outcomes was analyzed. In a pre-specified sub-analysis, the effect of intervention in regard to baseline vitamin D insufficiency [25(OH)D <50 nmol/L] was investigated. In exploratory analyses, the effect of intervention in regard to 9-month TSH level below or above upper normal range was investigated. For all repeated outcomes, the effect of intervention was analyzed by using linear mixed modeling with time and randomization group and their interaction as fixed factors and participants as random effects. The unequal standard errors and correlations in the two groups were taken into account in the analysis when relevant. Model validation was performed by inspection of QQ-plots of the residuals. The between-group difference was assessed by comparing the difference in change from baseline to 9 months between groups. The relative difference in change between groups was calculated as the difference in relative change in the vitamin D group minus the placebo group divided by the relative change in the placebo group and given as a percentage.
In the analysis of the effect of ATD, linear mixed modeling was applied as described earlier and the main effect of time was reported. In the analysis of muscle strength, body composition, and QoL, the interaction term of time and group was kept in the model. In all other analyses, when the interaction term was not significant it was left out of the model. If the main effect of the group was not significant, this term was also left out of the model.
Interpretation of differences and changes in ThyPRO scores were based on previous studies: 4–10 points denote a “small” difference or change, 10–16 indicate a “moderate” change, and a difference or change >16 points on the 0–100 scale is interpreted as “large” (4).
The correlation between baseline QoL measures and muscle strength assessments was explored by using adjusted linear regression analysis [adjusted for age, 25(OH)D, free T3, and TRAb].
With the use of linear mixed modeling for analyses, all collected data were included in analysis despite drop out at a later time point. Imputation of missing data was not performed. p-Values <0.05 were considered significant. Data were analyzed by using STATA version 15 (STATA Corp LP, College Station, TX). Trial findings are reported in accordance with the CONSORT statement (19).
Ethical considerations
All participants gave written informed consent. The study was performed in accordance with the Declaration of Helsinki. The regional committee on Biomedical Research Ethics approved the study. The trial was prospectively registered (
Results
During the study period, 348 patients newly diagnosed with GD were screened. A flow chart and description of exclusions and dropouts have previously been published (12). In summary, 86 participants were included in the study and randomized to vitamin D (n = 44) or placebo (N = 42). In the vitamin D and the placebo group, 43 and 39 participants completed 3 months of follow-up and 37 and 37 participants completed 9 months of follow-up, respectively. All participants received the intended intervention, and all randomized participants were included in the main analysis.
Clinical characteristics and demographics at baseline are shown in Table 1. Randomization was balanced without significant differences between groups. Participants (86% females) were 41 (±14, SD) years of age. Complaints of muscle weakness (81% [confidence interval, CI 71–86]) and muscle pain (51% [CI 39–62]) were frequent in the study population with no differences between groups at baseline, p-values 0.11 and 0.32. Nine percent (CI 4–17) reported muscle pains as the primary reason for seeking medical assistance, and 19% (CI 11–28) reported use of analgesics. Baseline 25(OH)D level (67.3 ± 29.6 nmol/L) and the proportion of vitamin D insufficient participants (<50 nmol/L) did not differ between groups (Table 1). Only six participants had a baseline 25(OH)D level below 30 nmol/L. The prescribed dosage of ATD did not differ at baseline (Table 1) or at 9 months of follow-up (vitamin D group vs. placebo, median thiamazole dosage [interquartile range]: 5 [4.3–10] vs. 5 [3.8–7.5] mg, p-value 0.83).
Baseline Demographic and Clinical Characteristics
Numbers (n) with percentage (%), mean ± standard deviation, or median with IQR.
ATD: 93% of patients were prescribed thiamazole, and it is the median (IQR) dose for this drug that is reported.
Only for users of vitamin D supplementation.
Vitamin D insufficient: 25(OH)D <50 nmol/L.
Reference ranges: free triiodothyronine 3.9–6.8, free thyroxine 12–21, thyrotropin receptor antibody (TRAb) <1.75, albumin 36–48 (18–40 years) and 36–45 (40–70 years), 25(OH)D 50–160 nmol/L.
25(OH)D, 25-hydroxyvitamin D; ATD, anti-thyroid drug; IQR, interquartile range; MET, metabolic equivalents (please see Methods section for details); TRAb, thyroid stimulating hormone receptor antibody; VitD suppl, vitamin D supplementation.
Effect of intervention on 25(OH)D level
The level of 25(OH)D increased in the vitamin D group by 45 (CI 33–57) nmol/L and decreased in the placebo group by 14 (CI −24 to −4) nmol/L. Accordingly, the intervention resulted in a between-group difference of 59 (CI 44–74) nmol/L, p < 0.0001. The decrease in 25(OH)D levels in the placebo group reflects the seasonal drop in 25(OH)D as the majority of participants were enrolled during the summer time. All participants in the vitamin D group had a replete vitamin D status (>50 nmol/L) at 9 months of follow-up.
Muscle strength, muscle function tests, and postural stability
Effects of 9 months of vitamin D supplementation on muscle strength (primary outcome) are shown in Figure 1. Supplemental vitamin D did not improve muscle strength. Actually, vitamin D supplementation attenuated the increase in muscle strength at all sites investigated, although only significant at the knee extension 60°. The improvement of muscle strength in the vitamin D group versus the placebo group was 76 (CI 56–97) N versus 101 (CI 80–122) N, corresponding to a 24% smaller improvement in the vitamin D group, p = 0.04. The increase in muscle force at hand grip and elbow flexion was 23% (p = 0.18) and 25% (p = 0.07) smaller in the vitamin D group than in the placebo group. The effect of intervention was significantly different by sex (p-value for interaction 0.04). Therefore, we looked separately at the effect of intervention among female sex and found the same pattern of attenuation of muscle strength with vitamin D supplementation in all muscle groups, significant at hand grip and knee extension 60°. No significant effect could be demonstrated among males, which may be due to the small sample size (males n = 12). There were no significant effects of vitamin D supplementation on force production or muscle function tests (data not shown). The intervention did not affect postural stability (Fig. 2).
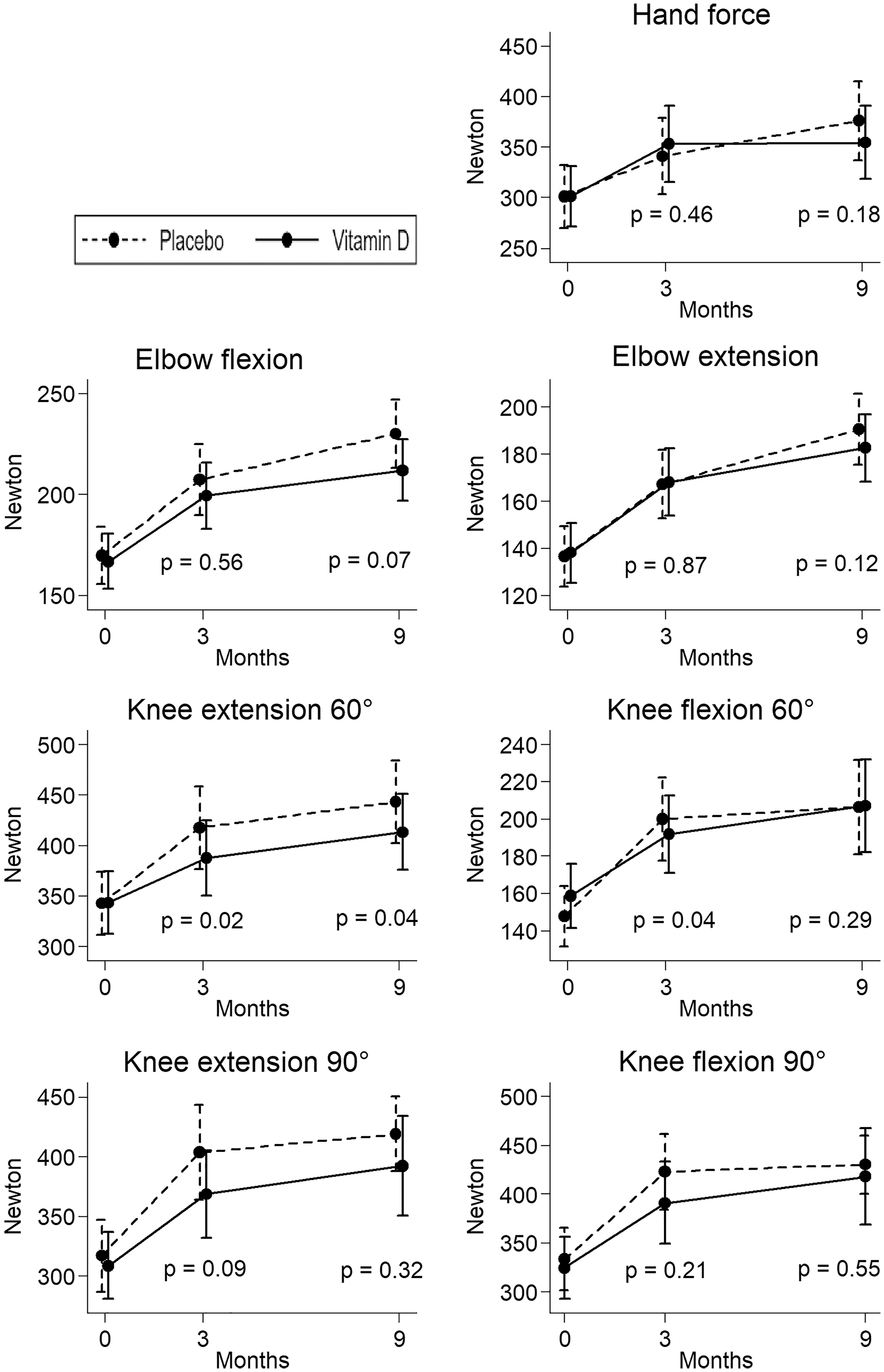
Effects of 9 months of vitamin D supplementation in Graves' disease given as add-on to standard antithyroid treatment of Graves' disease on maximum voluntary isometric muscle strength. Data shows group mean with standard deviation (error bars). p-Values refer to the test of between-group difference in change from baseline to 3 and 9 months of supplementation.
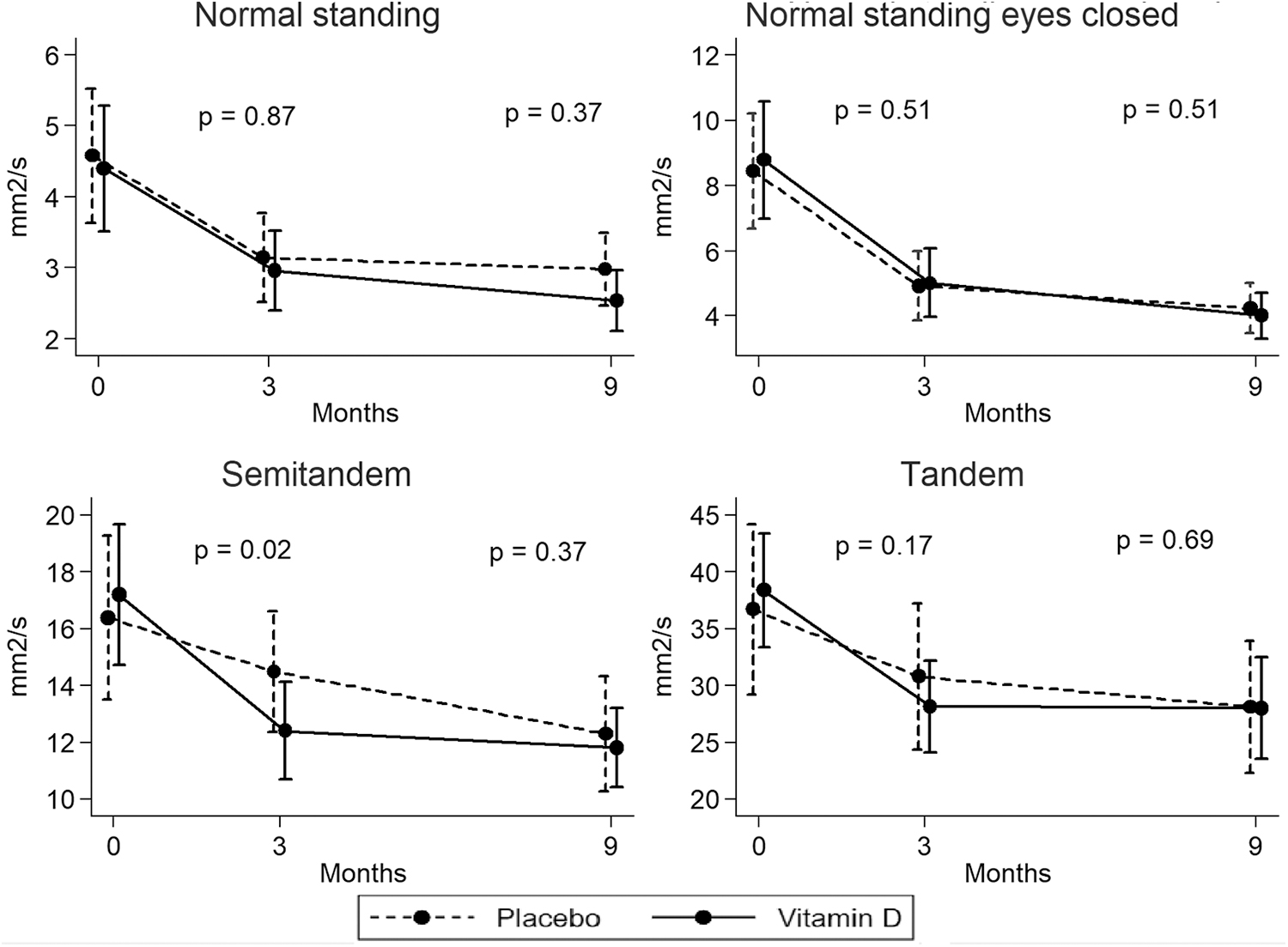
Effect of 9 months of vitamin D supplementation on postural stability in patients with Graves' disease. Data shows group mean with standard deviation (error bars). p-Values refer to tests of between-group difference in change from baseline to 3 and 9 months using linear mixed modeling. Higher values indicate lower postural stability (worse balance function).
In sub-analyses, the response to vitamin D in regard to baseline 25(OH)D level (above or below 50 nmol/L) was not statistically significant in any analyses of muscle strength, performance test, or postural stability (data not shown). Further, the effect of intervention was independent of achievement of euthyroidism at 9 months (data not shown).
In an exploratory analyses restricted to the vitamin D group, the effect of intervention was not statistically significant in those reaching a 25(OH)D level above (n = 11) versus below 120 nmol/L.
There was also no between-group differences in change of thyroid hormones or level of TRAb (12).
Physical activity and lean body mass
Physical activity was not statistically different at baseline (Table 1), 3 or 9 months, and there was no between-group change in MET score from baseline to 9 months (vitamin D vs. placebo: 2.2 ± 8.2 MET vs. 3.4 ± 9.1 MET, p = 0.56). Supplemental vitamin D did not improve the increase in lean body mass compared with placebo. In contrast, lean body mass tended to be lower at all sites in the vitamin D group as the increase in subtotal lean body mass was 24% lower than in the placebo group (p = 0.08). A similar non-significant effect on fat mass and body weight was observed. Changes in body composition are shown in Table 2.
Effect of 9 Months of Vitamin D Supplementation on Change in Body Composition
The difference in change at 9 months vs. baseline. Mean with CIs.
CIs, confidence intervals.
Symptoms and health-related QoL
The changes in the proportion of patients complaining of muscle weakness and reduced endurance of muscle force were not statistically different between groups (data not shown). Complaints of muscle weakness disappeared in 21 (50%) in the placebo group versus 15 (34%) in the vitamin D group, p = 0.14. Similarly, the proportion complaining of muscle pain was comparable, as was the proportion who initiated the use of analgesics due to muscle pain during the study period (vitamin D vs. placebo: 9% vs. 5%, p = 0.43).
Vitamin D supplementation did not improve QoL. In contrast, alleviation of the Composite QoL Scale was significantly lower in the vitamin D group (8 [CI 1–15] points, p = 0.001). Also, there was a trend toward reduced amelioration of QoL as assessed by the Overall QoL-Impact Scale and the Impaired Daily Life scale, although the differences in change in these measures were not statistically significant (Fig. 3). The difference in change of Composite QoL corresponded to a “small” clinical difference. Differences in change on the Hyperthyroid Symptoms Scale showed the same tendency of less improvement in the vitamin D group whereas improvement on the Tiredness Scale were comparable between groups (Fig. 3).

Changes of QoL scores as assessed by the ThyPRO Scales: Overall QoL-Impact, Composite QoL, Impaired Daily Life, Tiredness and Hyperthyroid Symptoms Scale in response to 9 months of vitamin D supplementation in Graves' disease. Data shows group mean with standard deviation (error bars). Higher scores indicate more symptoms or impairment. The p-values refer to tests of between-group difference in change from baseline to 9 months using linear mixed modeling. QoL, quality of life.
Correlations between QoL and muscle strength
For all assessments of muscle strength at baseline, we found a trend toward better QoL (lower QoL-impact score) with higher muscle strength. For muscle strength at elbow flexion and extension, the association with better QoL was statistically significant in terms of Impaired Daily Life, Tiredness, and ThyPRO Composite Scale. This was not different when adjusting for age, 25(OH)D levels, TRAb, and free T3 (Supplementary Table S1). For every 50 N increase in elbow extension and flexion, Impaired Daily Life score improved significantly by 9 (CI −15 to −2) and 8 (CI −14 to −2) points, respectively. Correlations at 9 months showed a similar, although non-significant, direction in all analyses (data not shown). The change in 25(OH)D level from baseline to nine 9 months did not significantly correlate with change in muscle strength or quality of lifeQoL measures.
Effects of ATD
During 9 months of ATD therapy, there were marked improvements in all aspects of muscle performance. Muscle strength increased by 34% (range: 25–40), muscle force production increased by 32% (range: 14–51), postural stability improved by 35% (range: 24–52), and the time spent performing muscle function tests decreased (Table 3). The increase in lean body mass was 14% (CI 11–17) in upper limbs, 11% (CI 8–13) in lower limbs, and 10% (CI 8–12) in subtotal lean body mass. Results were not changed by restricting analyses to only those receiving placebo during the trial (Supplementary Table S2).
Change in Physical Performance and Body Composition in Patients with Graves' Disease During 9 Months of Anti-Thyroid Medication
Estimates are relative difference at 3 or 9 months vs. baseline with CIs. Linear mixed modeling, please see the Methods section for details. The main effect of time is reported.
p < 0.001; b p < 0.05; c p < 0.01.
NA, not available (not measured).
The ATD led to marked improvements on all ThyPRO-related QoL scales (Fig. 4), with “large” changes for all scales. Change in QoL score from baseline to 9 months: Overall QoL-Impact Scale −39 (CI −50 to −28) points; Composite QoL Scale −21 (CI −25 to −18) points; Hyperthyroid Symptoms Scale −35 (CI −41 to −30) points; Tiredness Scale −25 (CI −30 to −19) points; and Impaired Daily Life Scale −36 (CI −49 to −27) points. A sensitivity analysis, only including participants randomized to placebo, showed similar results (data not shown). Compared with baseline, the proportions reporting complaints of muscle weakness and muscle pain at 9 months of follow-up were reduced from 81% (CI 71–86) to 14% (CI 6–25), (p < 0.0001) and from 51% (CI 39–62) to 29% (CI 18–43), p = 0.81, respectively.
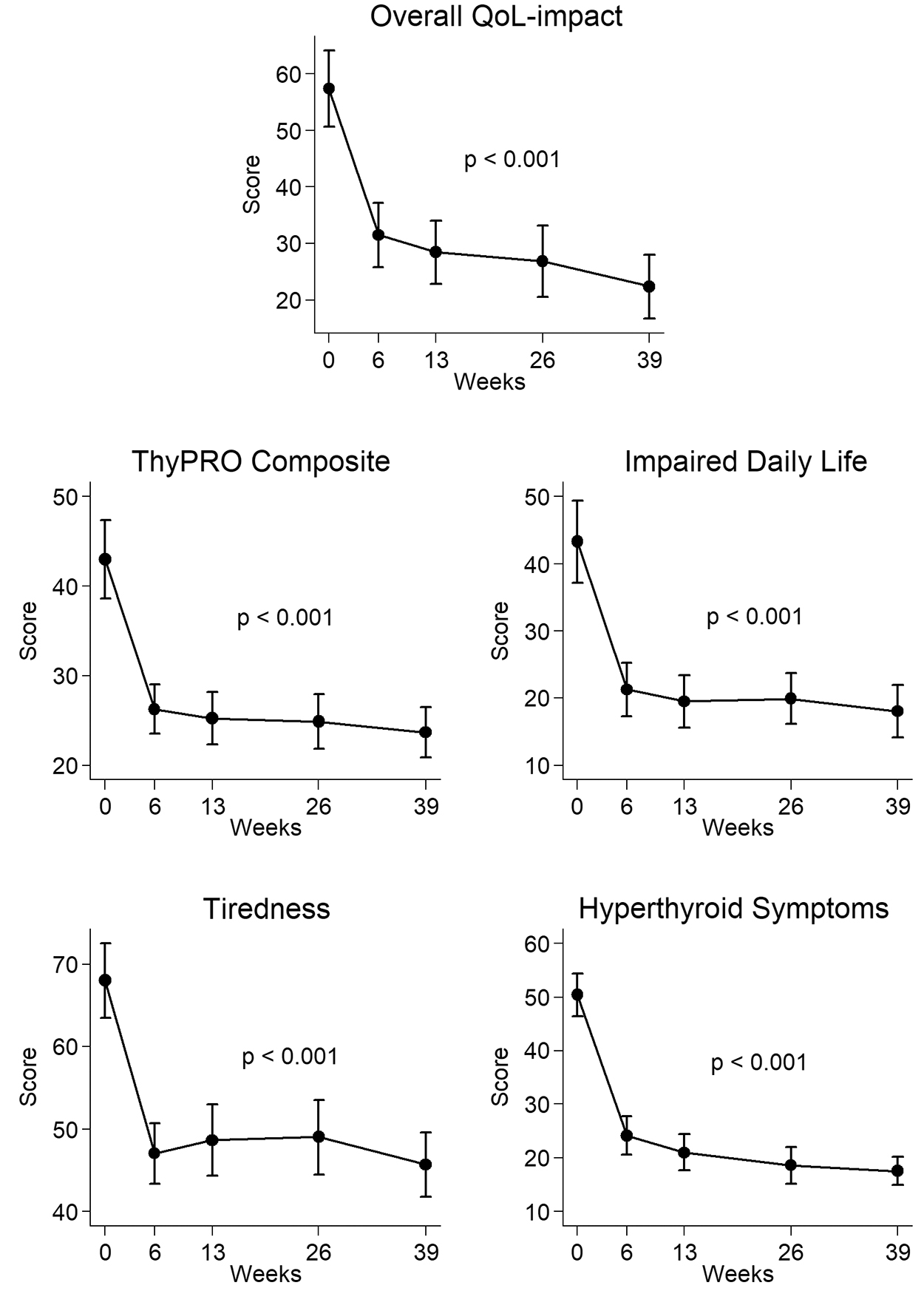
Changes in QoL scores as assessed by the ThyPRO Overall QoL-Impact, Composite QoL, Impaired Daily Life, Tiredness and Hyperthyroid Symptoms Scales in response to anti-thyroid medication in Graves' disease. Data show group mean with standard deviation (error bars). p-Values refers to every test of differences in scores from baseline to 6, 13, 26, and 39 weeks using linear mixed modeling. A higher score indicates more symptoms or impairment.
Discussion
In this randomized, double-blinded clinical trial, we investigated the effects of supplemental vitamin D versus placebo on muscle performance and QoL in patients with GD. We observed an adverse response in all muscle strength assessments (primary outcome). Increment of strength was less at both upper and lower extremities in the vitamin D group, although it was statistically significant only at knee extension 60°, 24% less improvement compared with the placebo group. We also found an adverse effect on QoL, as improvement was less pronounced in the vitamin D group. Muscle force production, muscle function tests, postural stability, and lean body mass were not significantly affected by intervention. In response to 9 months of ATD treatment, all outcomes showed significant and marked improvements in the entire cohort.
Despite a large number of randomized control trials, controversy surrounds the effects of supplemental vitamin D on muscle performance. Several systematic reviews and five meta-analyses (MAs) have been performed. Three MA found beneficial effects (20 –22) and two found neutral or divergent results (23,24). The studies included in the MAs show large heterogeneity and presumably several factors may impact the effect of vitamin D supplementation such as the form of vitamin D used, the dose and the dosing regimen applied, the baseline 25(OH)D level of participants, and the speed of 25(OH)D level increase in the subjects investigated.
An adverse effect of vitamin D has previously been shown in three other studies. Uusi-Rasi et al. (25) included home-dwelling elderly women at risk of falling (n = 409) and found prolonged TUG in response to 2 years of daily oral vitamin D3 20 μg a day (800 IU/day). Also, the improvement of muscle strength in response to exercise tended to be less in the vitamin D supplemented group. Mason et al. (26) included 218 obese or overweight, postmenopausal, women with 25(OH)D <80 nmol/L who were completing a lifestyle weight loss program. They found reduced leg strength in response to 12 months of daily oral vitamin D3 50 μg/day (2000 IU/day). Bislev et al. (27) investigated the effects of 3 months of daily oral D3 70 μg/day (2800 IU/day) in postmenopausal women (n = 81) with secondary hyperparathyroidism due to vitamin D insufficiency and observed reduced muscle strength and reduced physical performance as evaluated by the TUG test in response to intervention. No difference in lean body mass was observed.
The health condition, and hence the condition of the muscle tissue of the investigated population, may also be of importance in evaluating the effects of supplemental vitamin D. There are no previous studies on the muscle response to supplemental vitamin D in patients with GD or in hyperthyroidism due to other causes. With hyperthyroidism, protein synthesis as well as breakdown is increased, but muscle protein breakdown is dominant resulting in pronounced muscle wasting (28). As such, the condition of hyperthyroidism has some similarities to the condition of cachexia. In a study on rodents suffering from cancer cachexia, treatment with calcitriol in supra-physiological dosage leads to overexpression of vitamin D receptor and a negative regulation of myogenesis with inadequate differentiation. The authors suggested that caution should be given when supplementing patients with cancer cachexia or other causes of skeletal muscle atrophy to avoid disturbance of the regenerative process expected (29).
Impairment of muscle differentiation in response to vitamin D was also demonstrated in an in vitro study of injured human muscle cells, where muscle cell regeneration and differentiation was negatively affected in response to high-dose versus low-dose active vitamin D (calcitriol) or placebo (30). Gene expression differed in response to high-dose and low-dose calcitriol, which was also reflected in differing plasma creatinine activity levels. These findings suggest pathways for a potential harmful effect of high-dose vitamin D, interacting directly with the skeletal muscle tissue. Thus, a differential effect of high-dose and low-dose vitamin D seems possible and in accordance with this, none of the clinical studies using vitamin D dosages below 20 μg/day found harmful effects on muscle performance.
The effect of supplemental vitamin D on a lower gain of lean body mass was borderline significant (p = 0.08). We cannot exclude that such an effect is present and that the lack of significance is due to low statistical power. A reduced lean body mass is consistent with the adverse effect of high-dose vitamin D reported on muscular health in GD. Intriguingly, we observed the same tendency toward attenuated gain in fat mass with vitamin D supplementation.
In contrast to our findings, beneficial effects of vitamin D on balance have been reported in previous studies (31 –34). The study population consisted of all seniors and this may contribute to the difference in response to vitamin D. A beneficial effect on TUG as reported in two MA (21,24) could not be reproduced in our study, although the literature is inconsistent. Differences in the study population constitute a likely explanation.
In a 2016 review on health-related QoL outcomes of vitamin D therapy, Hoffmann et al. (35) concluded that quality evidence regarding QoL outcome is lacking due to poor methodologic quality of the 15 available studies (combined randomized control trials, cross-sectional and observational studies). A modest effect on QoL in affected populations over the short term (<6 months) was suggested. A more recently published study using a disease-specific questionnaire in patients with heart failure reported impairments of QoL (36). This is in line with our findings.
We found that QoL is related to muscle performance in hyperthyroid GD patients and that impairment of QoL is more pronounced (higher score) when muscle strength is lower (Supplementary Table S1). The association of Impaired Daily Life and muscle strength assessments showed the highest effect size for upper limb strength. This association highlights the importance of impaired muscle strength in the symptomatology of GD and suggests that the diminished recovery of muscle performance in the vitamin D group may contribute to the impaired improvement of QoL observed with this intervention. Thus, we speculate that the high-dose vitamin D supplementation caused disturbed muscle regeneration or differentiation leading to reduced gain of muscle mass, causing reduced increase in muscle strength, and negatively affecting QoL.
There is increasing interest in the role of vitamin D in autoimmune diseases, including the possible therapeutic effect (37). As suggested by Cianferotti and Marcocci (38), different tissues may require different 25(OH)D levels for optimal function. Hence, vitamin D treatment may be concomitantly beneficial in one tissue and have an adverse effect in another tissue. We believe that future studies on the effect of vitamin D should apply a broad assessment of possible differential effects in different tissues.
It is noteworthy that despite marked improvements with ATD treatment, complaints of muscle pain and muscle weakness were still frequent (29% [CI 18–43] and 14% [CI 6–25]) 9 months after initiation of treatment. This indicates that continued efforts to improve the treatment of GD are warranted.
To the best of our knowledge, this is the first randomized control trial on the effects of supplemental vitamin D in patients with GD. Randomization was well balanced. We performed extensive assessments of muscular performance combined with evaluation of QoL by using the validated disease-specific ThyPRO survey. Although the use of multiple testing may increase the risk of a chance occurrence, we find it unlikely that our results are due to chance occurrence given the consistency of our results showing possible adverse effects on body composition, muscle strength, and QoL. The use of different vitamin D dosages would have been advantageous, allowing evaluation of dose
Conclusion
At time of diagnosis, GD patients suffer from impairments of muscle function and QoL that improve markedly with ATD treatment. Contrary to our expectations, a relatively high dose of vitamin D supplementation given as add-on to standard ATD did not result in beneficial effects but caused a lower gain in muscle strength and QoL measures. Further, we observed borderline reduction in gain of lean body mass and we hypothesize that the primary cause of the unfavorable response to high-dose vitamin D in hyperthyroid GD patients may be due to this. Thus, in GD patients with adequate 25(OH)D levels, supplemental vitamin D should not be recommended for alleviation of muscular symptoms. Future studies on improving muscular function in GD are still needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study received support from the Toyota foundation, Denmark, The Novo Nordic foundation (NNF15OC0017792), and Orkla Health.
Supplementary Material
Supplementary Table S1
Supplementary Table S2