
Abstract
Background:
While aspirin use is known to be associated with reduced incidence of various cancer types, it is unclear whether this benefit extends to thyroid cancer. We aimed to evaluate the association between aspirin use and thyroid cancer development.
Methods:
This nested case–control study used nationwide data from the Korean National Health Insurance Service-National Sample Cohort 2002–2015. In total, 4547 individuals with newly developed thyroid cancer were matched with 13,641 controls based on age, sex, and follow-up period. Odds ratios (ORs) and 95% confidence intervals (CIs) for thyroid cancer development according to aspirin use were analyzed using a multivariable conditional logistic regression model.
Results:
The number of days for which patients with thyroid cancer used aspirin (the proportions of no use, <30 days/year, 30–90 days/year, and ≥90 days/year were 93.03%, 6.51%, 0.31%, and 0.15%, respectively) was comparable with that of the controls (p = 0.371, chi-squared test). The risk of thyroid cancer development was not associated with the duration of aspirin use (ORs [CI] for aspirin use <30 days/year, 30–90 days/year, and ≥90 days/year were 1.11 [0.96–1.28], 1.01 [0.54–1.88], and 1.23 [0.50–3.06], respectively, compared with no use) after adjusting for body mass index, smoking status, hypertension, Charlson comorbidity index, and number of outpatient visits per year. In addition, subgroup analyses stratified by age, sex, and follow-up duration did not reveal any significant association between aspirin use and thyroid cancer.
Conclusions:
Our findings suggest that even extended aspirin use may not impact the prevention or onset of thyroid cancer.
Introduction
Aspirin use was reported to have anticancer effects, especially in colorectal cancer, for which consistent evidence has been reported (1 –5). Moreover, recent epidemiological studies showed a potential antitumorigenic activity of aspirin in hepatocellular, ovarian, and lung carcinomas (6 –9). Several preclinical pieces of evidence also support the anticancer effect of aspirin, and cyclooxygenase-2 (COX-2) inhibition was suggested as an important mechanism of cancer chemoprevention (10 –12).
Worldwide incidence and treatment costs of thyroid cancer have increased sharply over the past two decades (13 –15). Given its large health burden, it would be meaningful to explore the role of aspirin and thyroid cancer incidence. COX-2 is overexpressed in thyroid cancer, especially in more aggressive forms (16 –19). Moreover, anticancer effects of COX-2 inhibition were reported in thyroid cancer cell lines (20,21). However, no direct evidence of the chemopreventive role of aspirin for thyroid cancer in population-based studies is currently available. Because only limited studies with small sample sizes have addressed this topic (22,23), we chose to evaluate the association between aspirin use and thyroid cancer development using a large scale nationwide longitudinal nested case–control study.
Materials and Methods
Data sources
We employed a nested case–control design to investigate the association between aspirin use and newly developed thyroid cancer using the Korean National Health Insurance Service-National Sample Cohort (NHIS-NSC) version 2.0, a population-based retrospective cohort of Korean citizens (24).
In brief, NHIS-NSC included the main and two minor cohort groups. The main group comprised one million nationally representative cohorts who were sampled from across 2142 stratified subsets, by sex, age group, residential area, insurance type, and income level in 2006. They were followed up retrospectively and prospectively for 14 years (2002–2015) from 2006. The two minor groups comprised newborn babies since 2006 (n = 96,731) and cohorts with missing insurance information (n = 11,638). The NHIS-NSC database contains extensive information, including data on age and sex, diagnosis, medical service use, and detailed information on drug prescriptions.
Case identification and data selection
The main cohorts of the NHIS-NSC (n = 1,000,000) were selected for this study (Fig. 1). Next, health care beneficiaries (n = 66,415) were excluded because some information on their medical treatment before 2006 was missing. To ensure sufficient washout periods for defining cases, and utilization of information regarding covariates from the National Health Screening (NHS) database, we further excluded those who were newly registered in the National Health Insurance (NHI) since 2003 and those who had never participated in the NHS program since 2006. This resulted in 620,189 individuals who had registered in the NHI in 2002 and had participated in the NHS program at least once since 2006.
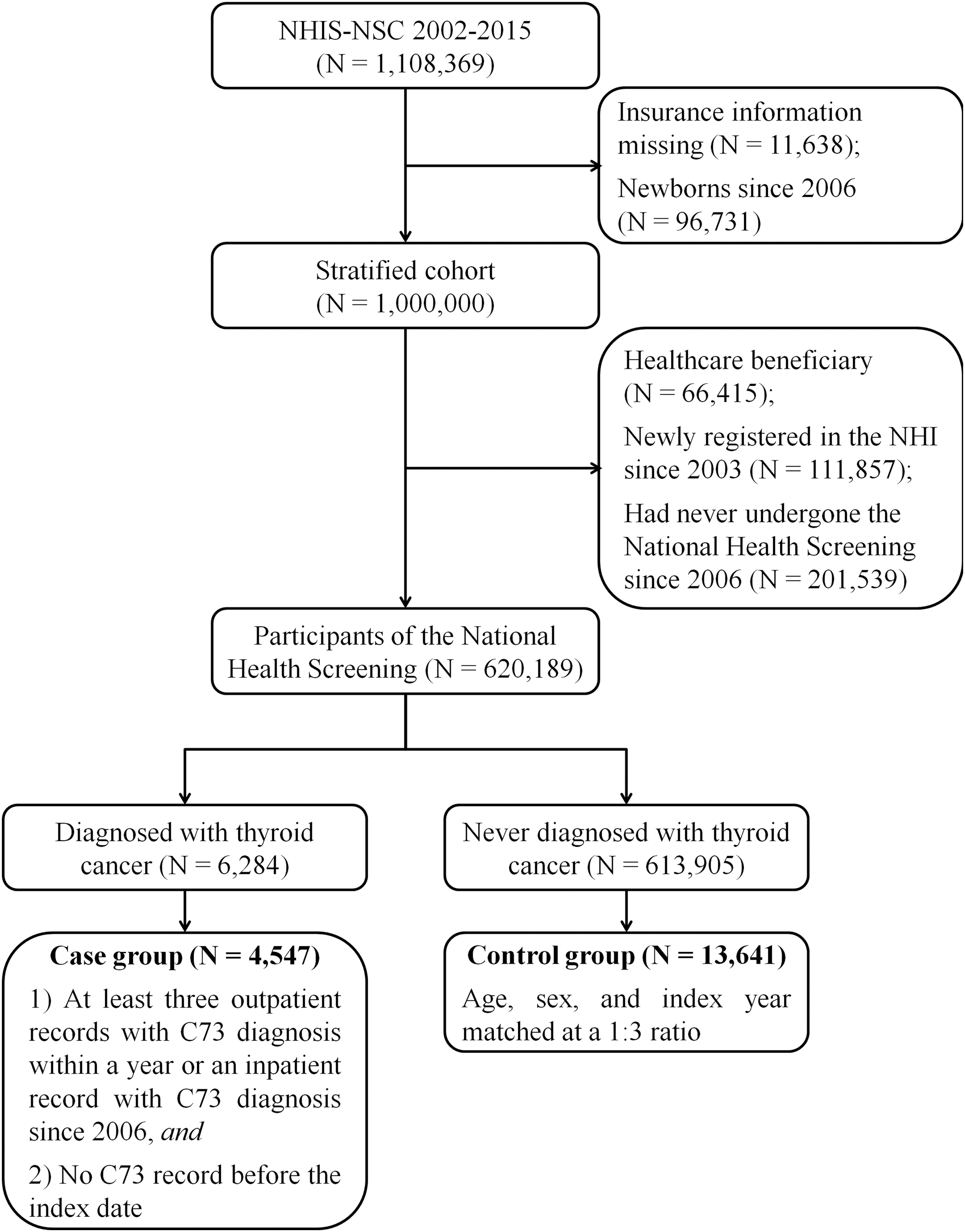
Flow chart of case and control group selection. NHI, National Health Insurance; NHIS-NSC, National Health Insurance Service-National Sample Cohort.
The case group included patients diagnosed with thyroid cancer since 2006 and with a minimum four-year follow-up. To identify case patients, we used the International Classification of Diseases 10th revision (ICD-10) code for thyroid cancer (C73). Based on our previous definition of cancer (25), we identified case group patients according to the following criteria: (i) presence of at least three outpatient records within a year with C73 as the main diagnosis, or at least one inpatient record with thyroid cancer as the main diagnosis since 2006; and (ii) absence of a C73 record before the defined event. Thus, the definition of the index date for the event was the first date of at least three thyroid cancer records with an outpatient code within a year, or of one thyroid cancer record with an inpatient code.
The final number of cases was 4547 and the median follow-up period was 9.52 years (interquartile range: 7.36–11.35). The control group comprised 13,641 individuals without a thyroid cancer diagnosis during the study period. Patients in both groups underwent 1:3 matching based on age (5 years intervals), sex, and follow-up period at the index date of each case. The study protocol was approved by the Institutional Review Board of National Cancer Center, Goyang, Korea (IRB: NCC2016–0142), and the requirement for informed consent was waived.
Assessment of aspirin use
We collected all aspirin prescription records before the index date and determined the daily aspirin intake (mg), excluding records with daily aspirin doses <75 mg due to potentially impaired biological responses associated with inadequate dosing. In addition, we excluded records of aspirin use within 180 days of the index date (lag period), considering the potential lag time between the actual onset of thyroid cancer and diagnosis.
Then, we counted the number of days of aspirin use, and calculated the average number of days of aspirin use per year (days/year) by dividing the cumulative number of days of aspirin use by the number of days from the first day of 2002 to 180 days before the index date and multiplied the value by 365 (number of days of aspirin use per year = cumulative number of days of aspirin use × 365/number of days from the first day of 2002 to 180 days before the index date). The number of days of aspirin use was categorized into four groups: no aspirin use, <30 days/year, 30–90 days/year, and ≥90 days/year. The average daily dose of aspirin for each aspirin user was also obtained by dividing the cumulative dose of aspirin by the cumulative number of days of aspirin use.
To minimize the potential bias related to the length of the lag period, we calculated the average number of days of aspirin use per year using two other lag periods (365 and 730 days). Furthermore, to minimize the potential bias due to the unit used to assess aspirin use, aspirin use was additionally evaluated by the cumulative dose of aspirin per year (mg/year) and the cumulative days of aspirin use (days).
Covariate information
Body mass index (BMI), smoking status, and history of diseases, including hypertension, heart disease, stroke, and diabetes mellitus, were extracted from the results of the NHS conducted on the date closest to the index date. The NHS questionnaire up to 2008 did not specify the type of heart disease, but the questionnaire from 2009 asked about the history of “heart disease (myocardial infarction, angina).” Missing BMI values (n = 6, all in controls) were imputed with mean BMI values of controls with the same age and sex.
The annual average number of outpatient records before the index date was obtained and categorized into quartiles to indicate the levels of individual health care utilization. The history of radiation therapy was obtained from the first day of 2002 to 180 days before the index date. In addition, the overall severity of baseline comorbidities was reported using the Charlson comorbidity index based on the ICD-10 code in inpatient and outpatient records in 2002. In this study, age was not included in the calculation of the Charlson comorbidity index.
Statistical analysis
Descriptive analyses were performed to show the distribution of each variable in the case and control groups; distributions were compared by chi-squared test and two-sample t-test.
Univariable conditional logistic regression analysis was performed to investigate the unadjusted association between thyroid cancer and each variable. Multivariable conditional logistic regression analysis was performed to investigate the association between the number of days of aspirin use and thyroid cancer development, after adjusting for the variables that were statistically significant in the preceding univariable analysis. The odds ratios (ORs) for thyroid cancer development are presented with their 95% confidence intervals (CIs). Any association was also explored in multiple subsets of variables, such as age (<55 and ≥55 years), sex (male and female), and follow-up period (<7, 7–11, and ≥11 years).
Statistical significance was set at p < 0.05. All analyses were performed using SAS 9.4 software (SAS Institute, Cary, NC).
Results
Baseline characteristics
The characteristics of the 4547 cases and 13,641 controls are given in Table 1. In total, 18.2% of the population comprised men, and 69.4% were younger than 55 years. Overall, 6.97% of the cases (n = 317) and 5.67% of the controls (n = 773) were prescribed aspirin during the follow-up period. There were no significant differences between the cases and the controls in the number of days of aspirin use per year (p = 0.371). The median average daily dose of aspirin for each patient who received aspirin for >30 days per year was 100 mg in both groups (Supplementary Table S1).
Baseline Characteristics of Included Cases and Controls
Values are presented as n (%), or mean ± standard deviation.
BMI, body mass index; NA, not applicable; Q, quartile.
The cases had higher average BMI than the controls (p < 0.001). Smoking status differed between the groups (p < 0.001), and the proportions of current smokers were lower in the case group than in the control group (6.22% vs. 10.60%). Charlson comorbidity index and the proportions of subjects with hypertension were higher in the case group (both p < 0.001) than in the control group, whereas the proportions of individuals with heart disease, stroke, diabetes mellitus, and history of radiation therapy were comparable between the groups (all p > 0.050). The number of outpatient visits per year was higher in the case group (p < 0.001).
Aspirin use and thyroid cancer development
The associations between thyroid cancer and variables, including aspirin use, were evaluated using conditional logistic models (Table 2). In the univariable analysis, short-term aspirin use (<30 days/year) was associated with higher odds for thyroid cancer (OR [CI], 1.23 [1.07–1.42]), compared with no use, whereas aspirin use for extended periods (OR [CI], 1.17 [0.63–2.16] for 30–90 days/year and 1.54 [0.62–3.81] for ≥90 days/year) did not show this association. In addition, BMI, smoking status, hypertension, Charlson comorbidity index, and the number of outpatient visits per year were associated with thyroid cancer in the univariable analysis.
Relationship Between Aspirin Use and Thyroid Cancer
The relationship between each variable and thyroid cancer is presented as ORs and their CIs.
Assessed based on responses to questionnaires asking about “history of heart disease” (until 2008) or “history of heart disease (myocardial infarction, angina)” (from 2009).
CI, 95% confidence interval; OR, odds ratio.
In the multivariable analysis, aspirin use was not associated with thyroid cancer development (adjusted OR [CI], 1.11 [0.96–1.28] for <30 days/year, 1.01 [0.54–1.88] for 30–90 days/year, and 1.23 [0.50–3.06] for ≥90 days/year) after adjusting for BMI, smoking status, hypertension, Charlson comorbidity index, and the number of outpatient visits per year. However, BMI (adjusted OR [CI], 1.03 [1.02–1.04] per 1 kg/m2) and smoking status (adjusted OR [CI], 0.49 [0.42–0.58] for current smoker) were associated with thyroid cancer. In addition, the OR for thyroid cancer increased as the number of outpatient visits increased (adjusted OR [CI], 1.34 [1.19–1.51] for the second quartile, 1.64 [1.45–1.86] for the third quartile, and 2.08 [1.85–2.34] for the fourth quartile compared with the first quartile).
The multivariable analyses using two other lag periods (365 and 730 days, instead of 180 days) between aspirin use and index date did not show an association between aspirin use and thyroid cancer development (Supplementary Table S2). In addition, neither the cumulative dose of aspirin per year nor the cumulative days of aspirin use was associated with thyroid cancer development after adjusting for potential confounding factors (Supplementary Table S3), consistent with the results using the number of days of aspirin use per year.
Subgroup analyses
The associations between aspirin use and thyroid cancer in the subgroups, represented as ORs and CIs, were plotted using a forest plot (Fig. 2). Aspirin use did not show any protective effects against thyroid cancer development regardless of age, sex, and follow-up period. While short-term aspirin use (<30 days/year) was associated with higher ORs for thyroid cancer development in patients aged ≥55 years (adjusted OR [CI], 1.33 [1.09–1.62]), aspirin use for extended periods (30–90 days/year and ≥90 days/year) was not associated with patients aged ≥55 years, or any other subgroup.
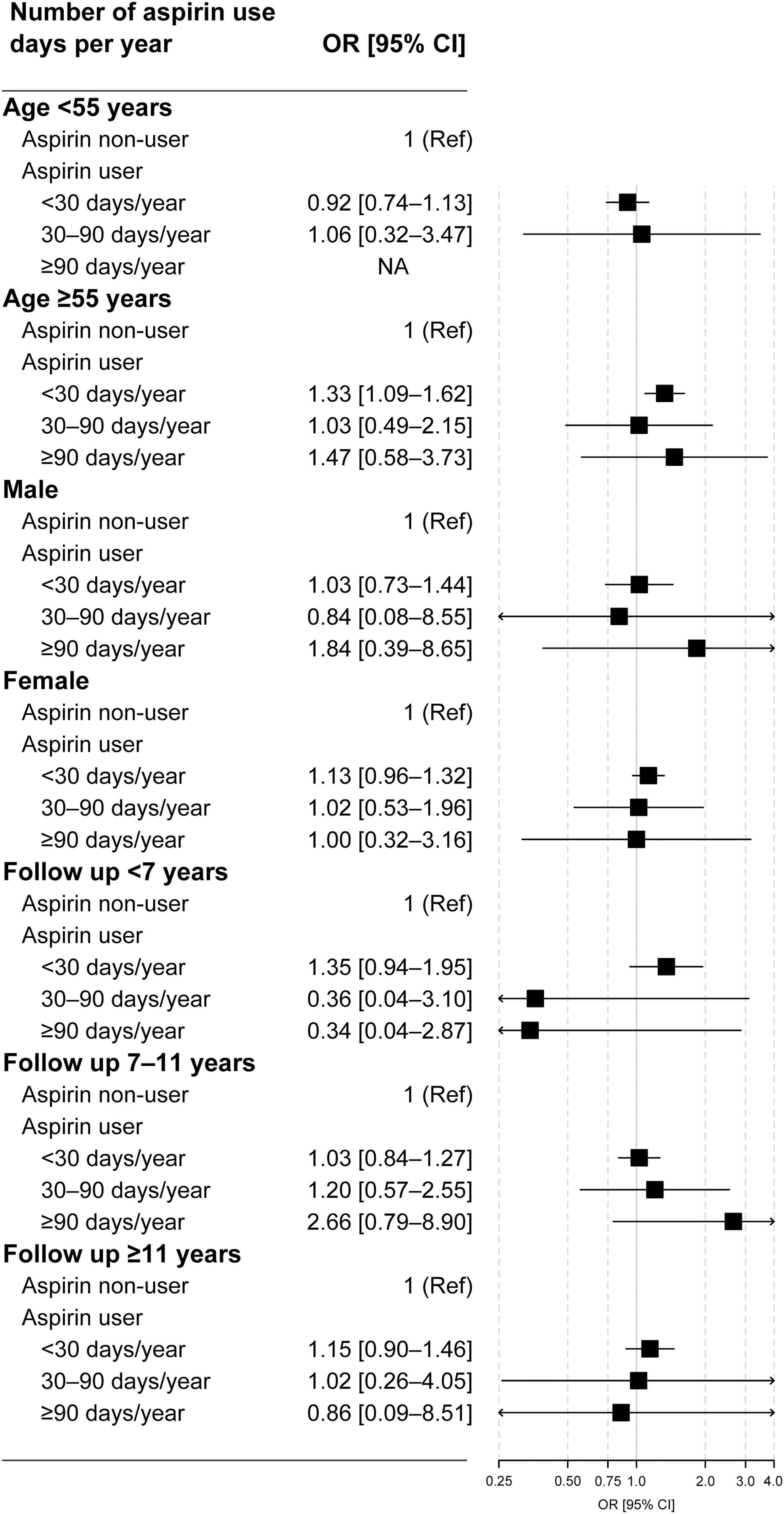
Forest plot of the ORs for thyroid cancer according to the number of days of aspirin use per year, separated by subgroups of age (<55 and ≥55 years), sex (male and female), and follow-up period (<7, 7–11, and ≥11 years). All ORs were adjusted for body mass index, smoking status, hypertension, Charlson comorbidity index, and the number of outpatient visits per year. CI, confidence interval; OR, odds ratio.
Discussion
In this study, we did not observe any association between thyroid cancer development and aspirin use, as well as in subgroup analyses conducted according to age, sex, and follow-up period.
The chemopreventive role of aspirin has been repeatedly demonstrated in various types of cancer (3,4,10). In one randomized controlled trial (RCT), aspirin use reduced by 63% the relative risk (RR) of colon cancer in individuals at risk for hereditary colorectal cancer (2). Furthermore, aspirin use was associated with a low OR (0.85) for overall cancer in a secondary analysis of 51 RCTs of aspirin for the prevention of cardiovascular events (5), and these findings were also observed in a study using two large long-term cohorts (RR = 0.97 for overall cancer and 0.81 for colorectal cancer) (1).
Moreover, recent extensive observational studies showed that aspirin use reduced hepatocellular carcinoma risk in the general population (6) and in patients with chronic hepatitis B (7). Aspirin use also reduced lung (9) and ovarian cancer risk (8), suggesting a role for aspirin beyond colorectal cancer, possibly as a chemopreventive agent in patients at a high risk for cancer.
Some preclinical evidence suggested that aspirin may also have an anticancer effect on thyroid cancer. COX-2 inhibition is presumed to be the major mechanism of inhibition of cancer development induced by aspirin, based on the observation that COX-2 and COX-mediated prostaglandin E2 (PGE2) synthesis promote cancer cell survival, proliferation, and metastasis (10,26). Thyroid cancer tissue overexpresses COX-2 (16 –19), which is associated with more aggressive features, such as lymph node metastasis and advanced stage (18,19). Moreover, in vitro studies showed that COX-2 inhibition might reduce proliferation, migration, and invasion rates of thyroid cancer cell lines (20,21). In addition, COX-mediated PGE2 expression is increased in thyroid cancer cells, and blocking PGE2 production restores natural killer cell-mediated cytotoxicity against thyroid cancer cells (27).
Nevertheless, two observational studies did not reveal any association between the use of aspirin and thyroid cancer incidence (Table 3) (22,23). Brasky et al. followed 129,013 women for 9.7 years and reported that the consistent use of aspirin did not reduce thyroid cancer risk (adjusted hazard ratio, HR [CI], 0.90 [0.53–1.53]) (22). Similarly, Patel et al. followed 388,577 participants and reported no significant association between aspirin use and thyroid cancer incidence (adjusted HR [CI], 1.06 [0.82–1.39] for daily aspirin use) (23).
Comparison of the Association of Aspirin Use with Thyroid Cancer Risk Between the Existing Literature and Current Study
HR, hazard ratio; ICD, International Classification of Disease.
However, in both studies, aspirin use was assessed based on self-administered questionnaires, and the number of patients with thyroid cancer was small (n = 208 and n = 481, respectively) (22,23). Therefore, we conducted a nested case–control study from a nationwide cohort to include a large number of patients with thyroid cancer with reliable prescription data. Our findings, which revealed no protective role of aspirin in thyroid cancer development, are consistent with the aforementioned study results (22,23).
The null association between aspirin use and thyroid cancer development may be attributed to the indolent nature of thyroid cancer. Most small papillary thyroid cancers grow slowly or remain stable without intervention (28,29). Thus, even if aspirin is chemopreventive, its additional protective effect may not reach clinically meaningful levels in thyroid cancer. In a recent meta-analysis, aspirin-induced cancer risk-reduction effects were weaker in cancers with a relatively indolent nature, such as breast (RR = 0.92) and prostate cancer (RR = 0.94), than in overall cancer (RR = 0.89), which may indirectly support the theory of a weaker anticancer effect of aspirin in indolent cancers (4).
In addition, since early thyroid cancer is often asymptomatic, there may be a long lag time between the actual onset and diagnosis of thyroid cancer that would require a longer follow-up time to detect a difference. In such cases, past long-term aspirin use may have a higher impact on the current incidence of thyroid cancer than recent aspirin use. However, we did not find significant differences based on follow-up periods in the subgroup analyses, but our follow-up time period may be too short.
This study reaffirmed the previously known association of BMI and smoking status with thyroid cancer development (30 –32). The underlying mechanisms have not been fully delineated and may be multifactorial, but changes in thyrotropin levels according to BMI and smoking status were proposed as one potential mediator (30 –32).
This study also confirmed the relationship between health care utilization and thyroid cancer. The screening effect has been suggested as a cause of the increased incidence of thyroid cancer (12,33 –35), and patients with higher health care utilization may have a greater likelihood of undergoing thyroid cancer screening. In this study, we identified the number of annual outpatient visits as a means of assessing overall health care utilization and found that patients with thyroid cancer had a higher frequency of outpatient visits.
However, in this study, thyroid cancer cases were defined as those involving multiple outpatient visits with the ICD-10 code C73 or admission with ICD-10 code C73. Thus, patients who were diagnosed with thyroid cancer but who had neither regular outpatient visits nor surgery due to their low levels of access to health care might be missing from the case group. As this might serve as a bias for the association between the number of annual outpatient visits and thyroid cancer, this association should be further validated before generalization.
Our study has several strengths. First, we used a nested case–control study design using a well-established and validated large national longitudinal data source from the NHIS-NSC. The database stores all aspirin prescriptions in clinical practice, due to which recall bias was avoided; this is a major advantage over data collected using questionnaires. Second, it included the largest number of patients with thyroid cancer compared with similar studies. Third, adjustments for various potential confounders, including the frequency of outpatient visits, were adopted to provide reliable results. Finally, we performed several subgroup analyses to explore the potential subgroup-specific association between aspirin use and thyroid cancer development.
Case–control studies, in general, have limitations owing to selection bias and observational design. However, both groups in our study were selected from a large population-based cohort, and, may be more representative of the population, thereby minimizing selection bias compared with traditional case–control studies (36). Since prescription data from before 2002 were unavailable, effects from >14 years before the study could not be evaluated. However, considering the risks of aspirin use such as major bleeding, the beneficial chemopreventive effect after >14 years of exposure may not be clinically significant, even if present. As most thyroid cancers in Korea are papillary type carcinomas (35), our findings should be interpreted with caution when applied to other types of thyroid cancer or populations with different genetic or racial backgrounds.
In conclusion, our analysis showed that aspirin use is not associated with thyroid cancer development in a Korean general population; therefore, aspirin may not be useful as a chemopreventive agent for thyroid cancer.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from the Korean Ministry of Health and Welfare (Grant No. 1520240) and the National Cancer Center, Korea (Grant No. 1810153). The funding sources had no involvement in study design, data collection, analysis, interpretation of data, or the decision to submit the article for publication.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3