
Abstract
Background:
Dementia is an increasing burden to the health care system. It is currently debated whether hyperthyroidism is associated with a risk of dementia. Our aim was to determine the risk of dementia in hyperthyroid individuals and whether this was associated with duration of hyperthyroidism.
Methods:
Risk of dementia in hyperthyroid individuals was evaluated in two cohorts and matched reference populations. The Danish National Patient Registry (DNPR) cohort is a registry-based Danish nationwide cohort followed for a median of 7.2 years (from 1995 to 2013), whereas the OPENTHYRO registry cohort comprises 235,547 individuals who had at least one serum thyrotropin (TSH) measurement in the period from 1995 to 2011 and was followed for a median of 7.3 years. Each hyperthyroid case was matched with four controls according to age and sex using density sampling. Hyperthyroidism was defined as either an International Classification of Diseases Version 10 (ICD-10) diagnosis of toxic nodular goiter (TNG) or Graves' disease (GD), or two measurements of a TSH below 0.3 mU/L in the DNPR and OPENTHYRO registry cohort, respectively. The primary outcome was all-cause dementia, defined as either an ICD-10 code of dementia or prescription of medicine for dementia, with subgroup analyses of vascular dementia and Alzheimer's disease.
Results:
The DNPR cohort had 56,128 patients with hyperthyroidism, 2689 of whom were registered with dementia. The reference population had 224,512 individuals, of whom 10,199 had dementia (hazard ratio 1.17; 95% confidence interval [CI]: 1.12–1.23). Risk of dementia, whether Alzheimer's or vascular, was higher in both GD and TNG. The OPENTHYRO registry cohort constituted 2688 hyperthyroid individuals and 10,752 euthyroid control individuals of whom 190 and 473 individuals, respectively, were subsequently diagnosed with dementia (HR 1.06; 95% CI: 0.89–1.26). For each 6 months of decreased TSH, the risk of all-cause dementia was significantly higher (HR 1.16; 95% CI: 1.12–1.22).
Conclusions:
Using large-scale registry-based data, we found increased risk of dementia in hyperthyroid individuals. Every 6 months of decreased TSH was associated with increased risk of dementia by 16%, compared with individuals with normal TSH. Our data support early diagnosis and intervention in patients with hyperthyroidism.
Introduction
Globally, dementia is an increasing burden to the health care system (1). In recent years, it has become evident that identifying modifiable risk factors, such as hypertension, diabetes, and smoking, is of importance. Whether hyperthyroidism could be such a modifiable risk factor for dementia is largely unknown.
Thyroid hormones are essential for optimal neurogenesis and neuronal differentiation, and play an important role in the maintenance of brain development and function throughout life (2,3). In a meta-analysis of five cohort studies, including 7895 individuals with subclinical hyperthyroidism (defined as decreased [low] serum thyrotropin [TSH] and normal levels of thyroid hormones) followed for a median of 34 months, the investigators found a decline in cognitive function based on a Mini-Mental State Examination (MMSE) (4). In a recent magnetic resonance imaging study of 2249 persons, higher serum concentration of free thyroxine (fT4) was associated with smaller total brain volume in the oldest participants, underscoring that thyroid function may influence brain morphology throughout life (5).
Two large cohort studies, the Rotterdam study (6) and the Framingham study (7), have found an inverse association between serum TSH level, even within the normal reference ranges, and the risk of dementia. Furthermore, the Framingham study demonstrated a direct association between the level of fT4 within the normal reference range and risk of dementia (7).
Both of these long-term follow-up studies were population based and included otherwise healthy residents. However, as a drawback, both studies had access to only a single measurement of TSH, fT4, or total thyroxine (T4) when categorizing the participants. This is problematic knowing that thyroid function may vary over time and that the cumulative period of thyroid dysfunction considerably affects mortality and the risk of cardiovascular disease (8,9). Moreover, the above studies did not include overtly hyperthyroid individuals thereby rendering any conclusions as to the risk of dementia in patients with hyperthyroidism impossible (6,7).
Patients with thyroid dysfunction, including both hyperthyroidism and hypothyroidism, have increased somatic (8,9) and psychiatric morbidity (10,11). Furthermore, hyperthyroidism has been linked to decreased quality of life and shortened life span compared with euthyroid individuals (12,13).
We hypothesized that patients with hyperthyroidism, compared with euthyroid individuals, also have increased risk of being diagnosed with dementia. Using the nationwide Danish health registries (14), and laboratory data from the OPENTHYRO registry cohort (15), we evaluated the risk of dementia in patients with hyperthyroidism. Moreover, we explored whether the association between hyperthyroidism and dementia was influenced by the cumulative exposure time to hyperthyroidism.
Methods
The unique personal identification number issued to all inhabitants in Denmark, at birth or immigration, enables individual-level record linkage between different government-based registries (16). The Danish National Patient Registry (DNPR) includes primary and supplementary diagnosis for all in-hospital contacts since 1977, and outpatient visits have been available since 1995 (17). DNPR has a coverage above 99%, and the overall positive predictive value of a diagnosis is above 95% (14). The Danish health care system is uniform, tax financed, and covers all residents. These conditions allow complete ascertainment and long-term follow-up of clinical conditions even with low base rates (14).
The DNPR cohort has been described in detail previously (18). In brief, it includes all adult patients in Denmark registered in the DNPR with hyperthyroidism either due to Graves' disease (GD) or toxic nodular goiter (TNG) (n = 55,656).
For each patient, four reference individuals (density sampled and matched for age and sex) were randomly selected from the Danish background population via the Danish civil registration system (19). Density sampling involves matching each hyperthyroid individual to reference individuals who are at risk (of hyperthyroidism) on the index date. Any of the reference individuals can during the follow-up period develop hyperthyroidism, and enter into the hyperthyroid group and be assigned their own reference individuals. This means controls could be sampled multiple times and cases could be sampled as controls before their date of being diagnosed with dementia. An important advantage of density sampling is that it ensures that the reference population is not too healthy when compared with the hyperthyroid group (20).
Table 1 summarizes all relevant data sources and International Classification of Diseases Version 10 (ICD-10) diagnoses used to identify hyperthyroid individuals and patients with dementia. The index date was defined as the date where the hyperthyroid diagnoses were entered into the DNPR.
Exposure Variables and Outcome Variables
The table shows the codes used to define diseases or conditions as used in the study, as well as which registries the data were extracted from and the variables used.
ATC, Anatomical Therapeutic Chemical Classification System; CCI, Charlson Comorbidity Index; DNPR, Danish National Patient Registry; DNPRr, Danish National Prescriptions Register, GD, Graves' disease; ICD-10, World Health Organization International Classification of Diseases version 10; TNG, toxic nodular goiter.
The OPENTHYRO registry cohort has been described in detail previously (9). In summary, this cohort consists of all individuals who had at least one TSH measurement done at the Odense University Hospital's Department of Clinical Biochemistry in the period of 1995–2012. The diagnosis of hyperthyroidism relied purely on biochemical data (TSH). Patients were classified as hyperthyroid if they had a minimum of two decreased TSH values (<0.3mIU/L) within a period of 6 months, with at least 14 days between measurements, thus limiting the risk of including patients with transiently low TSH levels (e.g., sick euthyroidism) into our hyperthyroid cohort.
For the current study, we matched hyperthyroid individuals with four euthyroid individuals for sex and age at first TSH measurement, using density sampling as described above. Euthyroidism was defined as previously done by our group as a TSH between 0.3 and 4.0 mIU/L, overt hyperthyroidism was defined as TSH <0.3 mIU/L and T4 > 135.0 nmol/L and/or triiodothyronine (T3) >2.2 nmol/L (above reference range), and subclinical hyperthyroidism was defined as TSH <0.3 mIU/L and T4 < 135 nmol/L and T3 < 2.2nmol/L (9). If we did not have data on thyroid hormone levels, the patient remained unclassified. The index date was defined as the date of the first TSH measurement in the hyperthyroid individuals.
For both cohorts, we used a one-year washout period before study entry (excluding all participants registered with hyperthyroidism between January 1 and December 31, 1995), thereby only including newly diagnosed cases (incident cases) of hyperthyroidism in the study.
We excluded all individuals (from both the DNPR cohort and the OPENTHYRO registry cohort and their relevant reference populations) with a dementia diagnosis entered into the DNPR, or starting a relevant drug to treat dementia before the index date. This implies that if any participants were registered with a dementia diagnosis before the index date, they would be excluded from the analysis. If a hyperthyroid individual was excluded, due to dementia before the index date, we also excluded all matched controls for this individual. If a reference individual was diagnosed before the index date, we only excluded that reference individual from the analysis.
Study outcome measures
For both the DNPR cohort and the OPENTHYRO registry cohort, all outcomes were defined in the same manner. The primary outcome in the study was all-cause dementia, and secondary outcomes were vascular dementia and Alzheimer's disease; definitions are outlined in Table 1. The date of dementia was defined as either the date of the first entry into DNPR or the first dispensed prescription of relevant medication (cholinesterase inhibitors; see Table 1), whichever occurred first.
The burden of pre-existing morbidity was evaluated by the Charlson Comorbidity Index (CCI) on the index date, as described by Christensen et al. (21).
Study bias
Bias due to pre-existing morbidity in patients with hyperthyroidism is an important limitation. Patients with hyperthyroidism more often than the reference population suffer from diseases, which are also associated with the development of dementia (22). It is difficult to adjust for these factors in a statistical analysis as this will result in adjusting the fitted model for the exposure, in this case hyperthyroidism (23).
In the DNPR cohort, the reference population is ascertained from the Danish background population. As a consequence, the reference population is “healthier” than the hyperthyroid individuals and any difference in risk of dementia between groups could be due to the varying distribution of risk factors for dementia, and not related to hyperthyroidism per se. We minimized this bias by using a density sampling method to select reference individuals allowing hyperthyroid individuals to be used as reference individuals until they developed hyperthyroidism (20). Another approach to account for such a bias is comparing results from two different cohorts.
In the OPENTHYRO registry cohort, all participants have had a blood test and thus at least one contact with a physician. Although the indication for testing thyroid function was unknown, it is reasonable to expect that euthyroid reference individuals from the OPENTHYRO registry cohort carry more morbidity than the general Danish background population. Accordingly, similar results in the two cohorts likely indicate that thyroid dysfunction per se influences the risk of dementia, while different results in the two cohorts suggest an effect of comorbidity.
Bias due to differences in baseline risk for dementia is also an important limitation in this study. Sex and age are major risk factors for dementia and hyperthyroidism (1,24). We have, by design, taken this into account and matched our reference populations by gender and birth year (DNPR cohort) or gender and age at first TSH measurement (OPENTHYRO registry cohort). While confounders such as alcohol and smoking habits were unknown to us, using the CCI our results are partly adjusted for liver disease and chronic obstructive pulmonary disease, to some extent a proxy for alcohol intake and smoking, respectively.
Statistical analyses
All statistical analyses were done using Stata® 14.2 (StataCorp) and SAS version 9.4. Data are presented as mean [ ± SD], median [interquartile range (IQR)], number of events, and percent of the population, as appropriate.
To evaluate the between-group hazard ratio (HR), we fitted a Cox proportional hazards model taking differences in pre-existing comorbidity into account, and a Fine and Gray (25) semiparametric competing risk regression model, taking the competing risk of death into account. The risk of all-cause dementia, Alzheimer's disease, and vascular dementia between all hyperthyroid patients, patients with TNG, and patients with GD was evaluated. Due to low incidence of vascular dementia and Alzheimer's disease, we only performed the adjusted analysis for all-cause dementia. HRs are presented as the HR between the hyperthyroid cohort and the reference population, accepting a significant HR if the 95% confidence interval (CI) did not include the value 1. The assumption of proportional hazards was evaluated by the log–log plot of survival for each group within each model used, accepting that the proportionality assumption held if the plots did not cross.
For the OPENTHYRO registry cohort, we furthermore used the TSH level as a time-dependent covariate using the array option in SAS®. The number of 6-month periods with TSH level <0.3 mIU/L was incorporated as a cumulative time-dependent covariate in a Cox proportional hazard regression model, thereby taking alterations in thyroid status over time into account. Any six-month period in which no TSH measurement had been performed was considered a period with normal TSH. Any six-month period in which more than one TSH measurement had been performed, we used the average TSH for all measurements within the window.
In a subgroup analysis of the OPENTHYRO registry cohort, we evaluated the risk of all-cause dementia in overt hyperthyroid and subclinical hyperthyroid individuals compared with the euthyroid reference population.
Ethical considerations and data sources
This study was approved by the Danish Data Protection Agency (reference no.: 704047).
Results
The DNPR cohort
Of a total population of 2,634,844 registered with an ICD-10 diagnosis, we identified 56,128 patients with hyperthyroidism, 2689 of whom were registered with dementia or had had a prescription for a drug used to treat dementia and was dispensed (Table 2). The reference population, matched 4:1 with the hyperthyroid group, comprised 224,512 individuals of whom 10,199 were classified as having dementia. We excluded 472 hyperthyroid individuals, and the corresponding 1888 reference individuals, because dementia was diagnosed before the hyperthyroid diagnosis. Furthermore, 2063 individuals from the reference population were excluded as they had been registered with a dementia diagnosis before the index date. This left 55,656 hyperthyroid individuals (35,522 with GD and 20,134 with TNG) and 220,561 reference individuals for analysis. The median follow-up time was 7.9 years [IQR 4.0–11.8], corresponding to 401,537 person-years of observation in the entire hyperthyroid cohort and 1,779,003 person-years of observation in the reference population. Participant characteristics are summarized in Table 2.
Characteristics of Study Cohort
The table shows participant characteristics for both hyperthyroid cohorts (DNPR and OPENTHYRO registry cohorts) and their reference population.
IQR, interquartile range; TSH, thyrotropin.
Risk of dementia in hyperthyroid individuals
The risk of dementia in the DNPR cohort is summarized in Table 3. The cumulative incidence function (risk of having the event at a certain time point, given that the participant has not met a competing event) is shown in Figure 1.
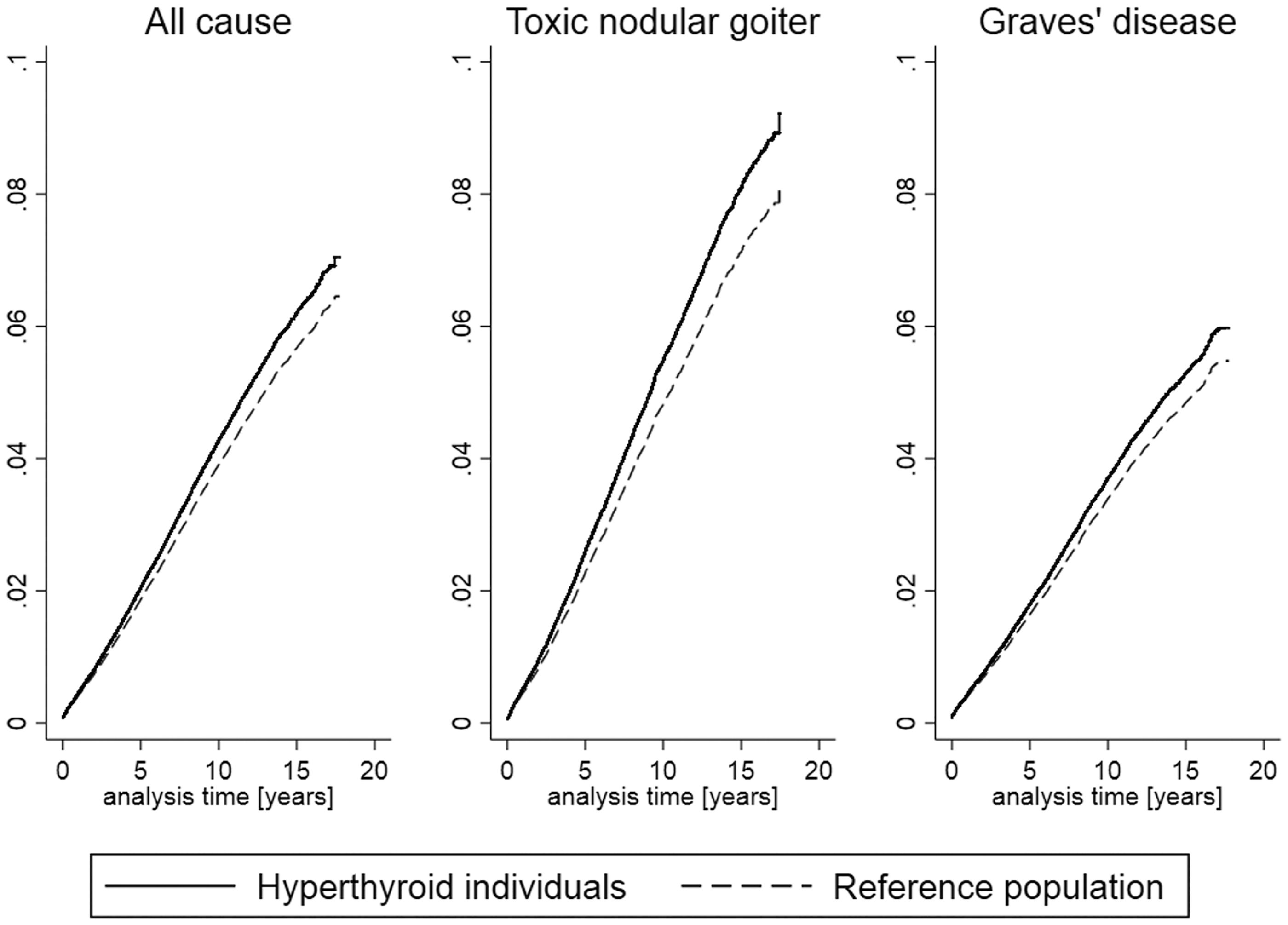
The cumulative incidence of dementia in all-cause hyperthyroid individuals, TNG, and GD patients compared with the reference population in the DNPR cohort. Cumulative incidence function, comparing the hyperthyroid individuals in the DNPR cohort with the reference population. The cumulative incidence function is the likelihood of having the event in question (dementia) at a given time—given that a competing event (death) has not yet been reached. The data arise from the Fine and Gray competing risk regression model and calculated from it. The y-axes indicate the probability of dementia (the cumulative incidence) at a given analysis time (x-axes). DNPR, Danish National Patient Registry; GD, Graves' disease; TNG, toxic nodular goiter.
Risk of Dementia in Hyperthyroid Individuals Identified Through the Danish Patient Register
Number of hyperthyroid patients and reference individuals registered with a dementia diagnosis, n (%); total number of events and percent of the total population. The crude model shows the HR comparing the hyperthyroid individuals to the reference population. The adjusted for CCI shows the HR comparing the hyperthyroid individuals to the reference population, but adjusting for differences in CCI. The competing risk regression shows the differences in HR between the hyperthyroid individuals and the reference population, taking the competing risk of death into account, in the hyperthyroid individuals. The cumulative exposure to decreased TSH was calculated based on windows of 6 months of TSH <0.3mU/L.
HR, hazard ratio; SHR, sub-hazard ratio.
In the DNPR cohort, a total of 2217 (4.9%) individuals were diagnosed with dementia, compared with 7907 (3.6%) in the reference population (HR 1.17; 95% CI: 1.12–1.23). After adjusting for pre-existing morbidity, the risk decreased but remained significant (HR 1.13; 95% CI: 1.07–1.19). The HR for dementia, after correcting for the competing risk of death, was 1.08 (95% CI: 1.03–1.14). When stratifying according to the cause of hyperthyroidism, both GD and TNG were associated with an increased risk of dementia (Table 3). The cumulative incidence of dementia was higher in hyperthyroid individuals than in the reference group, further underlining an increased risk of dementia in hyperthyroidism (Fig. 1).
Subanalysis by the type of dementia yielded essentially similar results. Two hundred eighteen individuals (0.4%) in the DNPR cohort were registered with a vascular dementia diagnosis, compared with 699 (0.3%) in the reference population (HR 1.33; 95% CI: 1.14–1.55). Four hundred eighty-six individuals (0.9%) of the hyperthyroid individuals and 1595 (0.7%) of the reference population were diagnosed with Alzheimer's disease (HR 1.29; 95% CI: 1.17–1.45).
The OPENTHYRO registry cohort
In the OPENTHYRO registry cohort, 235,547 individuals were eligible for inclusion in the analysis. After excluding patients with duplicate records and a dementia diagnosis before start of follow-up, 2688 (2077 females) hyperthyroid individuals were identified and matched with 10,752 individuals constituting the euthyroid reference population (1:4 match). The median follow-up time was 8.7 years (IQR: 5.1–11.9) in the hyperthyroid individuals and 5.2 years (IQR: 3.1–7.9) in the reference group, corresponding to 22,688 patient-years in the hyperthyroid group and 61,656 person-years in the reference group.
During follow-up, hyperthyroid individuals had a median of 12 [IQR 5–21] TSH measurements made, whereas the euthyroid reference group had a median of 2 [IQR 1–4] TSH measurements during follow-up. At baseline, the median TSH was 0.02IU/L [IQR <0.01–0.11] in the hyperthyroid cohort and 1.29IU/L [IQR 0.85–1.91] in the euthyroid reference individuals. The baseline T3 was 2.50 [IQR 2.07–3.30] (reference range 1.3–2.2 nmol/L) in the hyperthyroid individuals and 2.01 [IQR 1.75–2.37] in the euthyroid reference group. At baseline, the median T4 was 147 [IQR 122–189] (reference range 60–130 nmol/L) in hyperthyroid individuals and 118 [IQR 100–136] in the reference group. In the hyperthyroid group, 445 were classified as having subclinical hyperthyroid, 1793 as having overt hyperthyroid, and 341 could not be classified due to lack of information on baseline T3 and T4 levels. Participant characteristics are summarized in Table 2.
Risk of dementia in the OPENTHYRO registry cohort
The risk of dementia in the OPENTHYRO registry cohort is summarized in Table 1. The cumulative incidence function is shown in Figure 2. Risk of being diagnosed with dementia during follow-up was not significantly higher in the hyperthyroid individuals than in the reference population. One hundred ninety (7.1%) hyperthyroid individuals had been registered with dementia during follow-up, compared with 473 (4.4%) in the reference population (HR 1.06; 95% CI: 0.89–1.26), with no significant change after adjustment for differences in pre-existing morbidity (HR 1.06; 95% CI: 0.89–1.26) or when taking the competing risk of death into account (HR 1.12; 95% CI: 0.95–1.33). The cumulative incidence of dementia, however, was higher in the hyperthyroid individuals as illustrated by the cumulative incidence plot (Fig. 2). Similar results were found when evaluating the between-group differences in Alzheimer's disease and vascular dementia (Table 2).
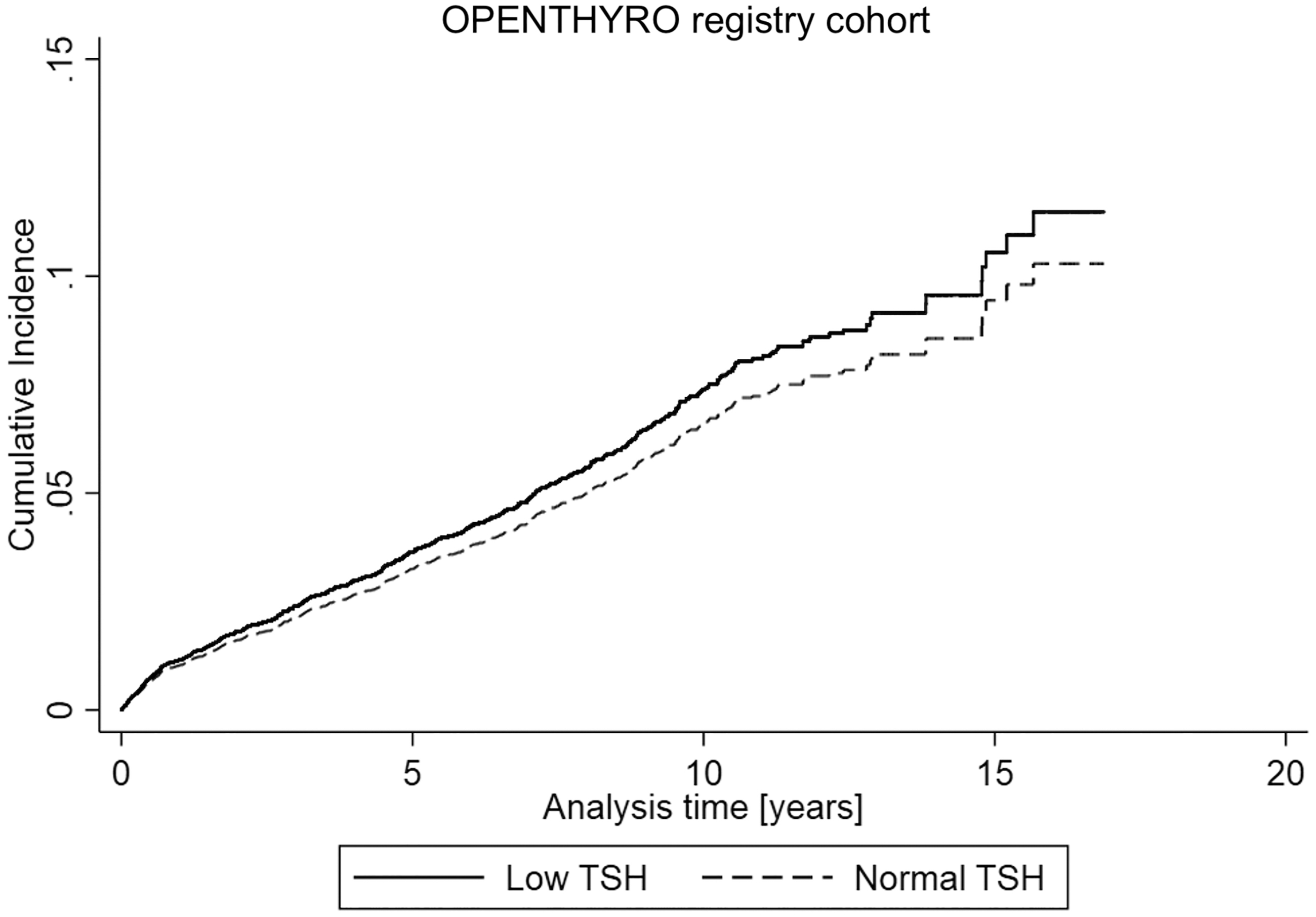
The cumulative incidence of dementia in hyperthyroid individuals compared with the reference population in the OPENTHYRO registry cohort. Cumulative incidence function comparing the hyperthyroid individuals in the OPENTHYRO registry cohort with the reference population. The cumulative incidence function is the likelihood of having the event in question (dementia) at a given time—given that a competing event (death) has not yet been reached. The data arise from the Fine and Gray competing risk regression model and calculated from it. The y-axis indicates the probability of dementia (the cumulative incidence) at a given analysis time (x-axis).
Risk of dementia based on cumulative decreased TSH
In hyperthyroid individuals, there was an increased risk of dementia compared with individuals with normal TSH (0.3–4.0 mIU/L) for each 6 months of decreased TSH (HR 1.16; 95% CI: 1.12–1.22). This corresponds to more than a 4.4 times increased risk of dementia over a 5-year period of lowered TSH, compared with individuals with a normal TSH.
Risk of dementia based on degree of hyperthyroidism
In the overt hyperthyroid group, 105 (5.5%) were diagnosed with dementia, whereas 46 (9.3%) in the subclinical hyperthyroid group were subsequently registered with dementia. There was no difference in the dementia risk between overt hyperthyroid individuals and the euthyroid reference group (HR 0.82 [95% CI 0.66–1.10]), whereas the risk of dementia was higher in the subclinical hyperthyroid group (HR 1.57 [95% CI 1.16–2.13]).
Discussion
Utilizing population-based Danish health registries, we have investigated two large patient cohorts with validated definitions of both hyperthyroidism (9,15,18) and dementia (26), thereby limiting some of the shortcomings of previous studies (4,6,7,27). Using this approach, we found an ∼20% relative increased risk of dementia in hyperthyroid individuals, which to some degree is explained by pre-existing morbidity. Novel is also the finding that each 6-month period of decreased TSH was associated with a higher relative risk of dementia by 16%, suggesting that the longer a patient has hyperthyroidism the greater the risk of developing dementia.
The observed association between hyperthyroidism and dementia is biologically plausible, since thyroid hormones are involved in the regulation of the amyloid-β and amyloid-β precursor genes (28) and amyloid-β disposition in the brain may contribute to the development of Alzheimer's disease (28). Furthermore, exposure to excess thyroid hormones has been shown to enhance neuronal death (29). In support of this finding, recent imaging studies have shown an inverse association between levels of T4 (within normal ranges) and brain volume in the elderly (5,29). Furthermore, thyroid hormone regulates hippocampal neurogenesis, and thyroid dysfunction may therefore negatively influence learning ability, cognitive performance, memory, and mood (30).
In a Danish study by Lillevang-Johansen et al. (27), utilizing data from 55 discordant twin pairs to control for genetic as well as early environmental factors, no clinically relevant negative impact of previous hyperthyroidism on cognitive function could be found. In a prospective study in 31 newly diagnosed patients with GD, and a euthyroid age-matched reference group, the cognitive impairment seen during hyperthyroidism normalized after euthyroidism (31), indicating that some of the cognitive impairment seen during hyperthyroidism may be transient. The increased risk of dementia found in our study therefore is possibly caused by other pathways, for example, increased somatic and psychiatric morbidity.
Hyperthyroidism is caused by autoimmunity in GD (32), or by one or more autonomously functioning thyroid nodules in TNG (24). Since these differ with respect to age at onset, duration, and severity of thyroid dysfunction (24,33), they may differ with respect to risk of dementia. Hypothetically, an increased risk of dementia could pertain to autoimmunity per se rather than the hyperthyroid state or vice versa. In line with this, a variety of autoimmune diseases, including autoimmune thyroid diseases, have been linked with increased risk of dementia (34). However, the fact that the risk estimates for being diagnosed with dementia did not differ between GD and TNG in our study support the notion that dementia is attributed to the hyperthyroid state rather than only to autoimmunity.
When interpreting the association between hyperthyroidism and dementia, it is important to note that hyperthyroidism is also associated with higher risk of cardiovascular and cerebrovascular disease (8,35), both associated with an increased risk of developing dementia. Thus, these comorbidities could, at least partly, explain the association between hyperthyroidism and dementia. Clearly our study, showing a decline in HRs, although still statistically significant when adjusting for comorbidity, supports this. On the contrary, our finding of a 16% increased risk of dementia for every 6 months of decreased TSH, in a sample where the hyperthyroid group and the reference individuals had equal frequency of cerebro- and cardiovascular diseases, suggests that hyperthyroidism is an independent and modifiable risk factor for dementia.
There are many risk factors for dementia some of which, such as smoking and alcohol consumption, obesity, hypertension, and education level (1), may be modifiable. Katon et al. (26) have shown that there is an additive effect of exposure to certain diseases on the risk of developing dementia over time. To minimize the effect of comorbidity, we adjusted our risk estimate analyses for pre-existing morbidity using the CCI. The reference population in the OPENTHYRO registry cohort had more pre-existing morbidity than the reference population in the DNPR cohort. This increased pre-existing morbidity in the OPENTHYRO registry cohort could, in part, explain why there was no significant difference in dementia risk between hyperthyroid and euthyroid individuals. Our registry-based data contain inadequate information about smoking and drinking habits. However, we adjusted our risk estimates for pre-existing lung and liver diseases and thereby, at least to some extent, adjusted for the effect of smoking and alcohol intake. Eliminating differences in the education level could reduce the risk of dementia by 8% (1). Lower education level in hyperthyroid individuals compared with a matched control group has been demonstrated (36). Since we do not have data on education level in our study cohorts, we cannot rule out that some of the increased risk of dementia is due to differences in education level.
The reason for the difference between overt and subclinical hyperthyroid individuals is most likely related to lack of treatment and longer duration of hyperthyroidism in patients with subclinical hyperthyroidism as shown by us previously (9). Patients with overt hyperthyroidism have significantly more pronounced thyroid dysfunction than patients classified as having subclinical hyperthyroidism. The consensus is to treat patients with overt hyperthyroidism, while many patients with subclinical hyperthyroidism do not receive treatment. Thus, a potential increased risk of dementia may have been offset because of treatment.
The lack of data on treatment and the effects of treatment in the participants included in the DNPR cohort is a limitation. Treatment of hyperthyroidism has a positive effect on mortality as well as on the risk of developing cardiovascular disease (8,9). It is likely, but at present unknown, whether treatment of hyperthyroidism also influences the risk of dementia in patients with hyperthyroidism. However, our finding of a 16% increase in risk of dementia per 6 months of decreased TSH, irrespective of treatment status, supports timely and effective treatment and careful monitoring. Any 6-month period with no TSH measurement was considered a euthyroid period. This implies that a hyperthyroid individual may have been considered euthyroid during a period of disease, which would lead to an underestimation rather than an inflation of dementia risk in hyperthyroid individuals.
Another limitation is the lack of insight into the basis on which the diagnoses were made. Registry-based studies are dependent on, and limited to, the decisions made by clinicians in their everyday clinical practice. However, several studies have shown that the positive predictive value of diagnoses registered in the DNPR is high (37,38). The current study was furthermore limited by the age at first TSH measurement being lower in the euthyroid individuals compared with the hyperthyroid individuals in the OPENTHYRO registry cohort (9). We, therefore, matched hyperthyroid individuals by age at first TSH rather than birth year. The window of observation was defined by the available data in calendar years, leaving the median observation time shorter in the OPENTHYRO reference group compared with the hyperthyroid individuals. Dementia is a disease of the elderly, and it is likely that the shorter observation time could cause the lower incidence of dementia in the reference group. However, the similar prevalence of dementia in the reference group in the DNPR cohort and the reference group in the OPENTHYRO registry cohort (3.6% and 4.4%, respectively) indicates that this was not the case in our study. Finally, due to the relatively low absolute risk of dementia found in the OPENTHYRO registry cohort, we cannot rule out that this cohort is underpowered.
There are several strengths to our study beyond including two cohorts with different ascertainment procedures. Using the DNPR cohort, we included all patients seen via the secondary health care system in Denmark. This offered a cohort of participants with high capture and a high number of participants with near complete follow-up, at the expense of having no information on biochemical variables or the effect of treatment. Therefore, we also included a cohort based on availability of laboratory data, including patients from the primary health care system (OPENTHYRO registry cohort). This meant lower capture rate and number of participants. A major strength lies in the utilization of two TSH measurements reducing risk of misclassification of hyperthyroidism because of transient thyrotoxicosis. In fact, ∼50% of patients with a decreased TSH have normal levels at repeat investigation (39). By including two different reference cohorts, one representing the general population and one representing a cohort of more ill patients, we limited the risk of comparing a morbid group to a healthy group, and as a consequence showing an increased risk of dementia not related to the thyroid disease but to the differences in morbidity between hyperthyroid individuals and the reference population.
Using nationwide registry-based data, and using two hyperthyroid cohorts, an ∼20% relative increased risk, which is partially explained by pre-existing nonthyroid morbidity, of being diagnosed with dementia is demonstrated. For every 6 months of decreased TSH, there is a 16% relative increased risk of dementia compared with individuals with normal TSH. Further studies regarding the association between the phenotypes of hyperthyroidism and the subtypes of dementia, as well as the effect of treatment of hyperthyroidism on the risk of dementia, are warranted.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.