
Abstract
Background:
The Afirma gene expression classifier (GEC) has been used to aid in the diagnosis and management of thyroid nodules having Bethesda category III fine-needle aspiration cytologic diagnosis (B3 nodules). The American Thyroid Association sonographic risk stratification system for thyroid nodules (ATA-US) may stratify B3 nodules and aid in the decision to order a molecular test. The aim of this study was to assess the association between ATA-US and GEC as well as to determine their individual and combined diagnostic performances when applied to B3 nodules.
Methods:
A retrospective single-center study included B3 nodules that had undergone evaluation by GEC. Each ultrasound was reviewed by three radiologists, and nodules were classified using the 2015 ATA sonographic risk categories. Nodules were determined to be benign or malignant based on surgical pathology or minimum 11 months of follow-up. Positive predictive values (PPV) and negative predictive values (NPV) were calculated for GEC, ATA-US, and GEC across all ATA-US categories.
Results:
One hundred twenty-six B3 nodules with GEC results were included and deemed benign or malignant based on final pathology or follow-up. Prevalence of malignancy was 32%. The rate of malignancy was similar in the ATA-US high suspicion (HS) and intermediate suspicion (IS) categories at 42% and 38%, respectively; and lower in nodules with low suspicion sonography (LS) and very low suspicion sonography (VLS) at 23% and 11%, respectively. The PPV and NPV of ATA-US was calculated by designating HS or IS sonography as a “positive” test and the lower risk categories as “negative.” ATA-US had a PPV of 40% and NPV of 79%. The GEC PPV was 40% and NPV was 83%. The PPV of GEC was 50% in nodules with HS or IS ATA-US and lower at 28% and 20%, respectively, in LS and VLS nodules. The NPV of GEC was 80% in HS, 77% in IS, 84% in LS, and 100% in VLS sonography categories.
Conclusions:
In B3 nodules, ATA-US and GEC have similar diagnostic performance. The PPV of GEC varies across ATA-US categories, while the NPV remains similar. These data support the need for future prospective studies.
Introduction
Thyroid nodules are very common in the general population and are frequently encountered in clinical practice. While the majority of thyroid nodules are benign and not clinically significant, a minority may harbor malignancy (1,2). Thyroid ultrasound and fine-needle aspiration cytology (FNA-C) are often performed during the diagnostic evaluation.
Despite advances in diagnostic methods, ∼20–25% of thyroid nodules will be classified as indeterminate (ITNs) by FNA-C. According to the Bethesda System for Reporting Thyroid Cytopathology, thyroid nodules with indeterminate cytology are grouped as Bethesda category III (Atypia of undetermined significance or Follicular lesion of undetermined significance [AUS/FLUS]), Bethesda category IV (Follicular neoplasm [FN]), or Bethesda category V (suspicious for malignancy) (3). The rate of malignancy (ROM) among nodules with Bethesda category III cytologic diagnosis (B3) varies between 6% and 48% often necessitating surgical diagnosis (2).
In recent years, several molecular tests, including Afirma gene expression classifier (GEC) (Veracyte), have been utilized to risk stratify ITNs and to aid in the decision to perform diagnostic thyroid surgery versus surveillance (4 –7). It has been proposed that the use of GEC has resulted in an ∼50% decrease in diagnostic thyroid surgeries in cases of ITNs (8 –10). GEC classifies ITNs as either “benign” (95% negative predictive value [NPV] for aspirates classified as AUS/FLUS and 94% for aspirates classified as FN) or “suspicious” for malignancy (positive predictive value [PPV] ∼40% for malignancy) (4). While this test performance has been reported in an initial validation study, a meta-analysis of more recent studies has brought into question whether the cohort of the initial validation study was representative of the populations in which the GEC has been used due to a wide difference in the NPV results (11). While few studies have assessed the impact of individual sonographic features on GEC test performance (12,13), it is not known whether the reported NPV and PPV would be different when GEC is applied in nodules of differing American Thyroid Association (ATA) sonographic risk category.
Several studies have reported that individual ultrasound features of ITNs as well as ultrasound-based classification systems may be able to assist clinicians in predicting malignancy among ITNs and to aid in the decision to order a molecular test before triaging the patient to either clinical follow-up or surgical intervention (14 –20).
The 2015 ATA management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer recommend classification of thyroid nodules into one of five sonographic patterns (ATA-US). According to these guidelines, the ATA sonographic classification scheme's primary use should be for determining the size cutoff threshold to perform FNA. The ATA sonographic risk classification system is also promoted by the guidelines authors as potentially useful in determining the optimal monitoring strategy for follow-up of thyroid nodules with benign FNA-C and for those nodules that do not meet criteria for FNA. Regarding management strategies for B3 nodules, the 2015 ATA guidelines recommend “consideration for worrisome clinical and sonographic features”; however, to date, few studies have addressed whether there could be a role of ATA-US in risk stratifying and decision-making in management of B3 nodules (14 –20).
Given the considerable cost and limited availability of molecular testing, some authors have recommended to further risk stratifying ITNs based on sonographic features, triaging higher risk ultrasound patterns to surgery, lower risk ultrasound patterns to observation, and offering molecular tests, where available, on the remainder (1,14,21). To the best of our knowledge, there are currently no published studies of ITNs assessing the association of sonographic findings to GEC, comparing the performance of ultrasound-based risk prediction with that of GEC, or reporting the performance of GEC within the various ATA sonographic risk categories.
The objective of this study was to assess the correlation between ATA-US categories and GEC results as well as to assess individual diagnostic performances of ATA-US and GEC and that of ATA-US and GEC combined when applied to B3 nodules.
Materials and Methods
Following approval by the Institutional Review Board of the University of Miami Miller School of Medicine, retrospective chart review of patients who had FNA-C reported as Bethesda category III (AUS/FLUS) from January 1, 2012, to December 31, 2017, was performed. Patients were included if aged 18 years or older, presence of one or more thyroid nodules confirmed by ultrasound results, and GEC result of suspicious or benign. One hundred seventeen patients with 126 nodules met the inclusion criteria and were included in the analysis of GEC and ultrasound results. One hundred twenty-six nodules either had surgical histopathologic diagnosis (n = 85) or had long-term follow-up after FNA-C (n = 41) and were included in the analysis of test performance of GEC and ATA-US (Fig. 1). Informed consent was waived as the study was retrospective in nature.
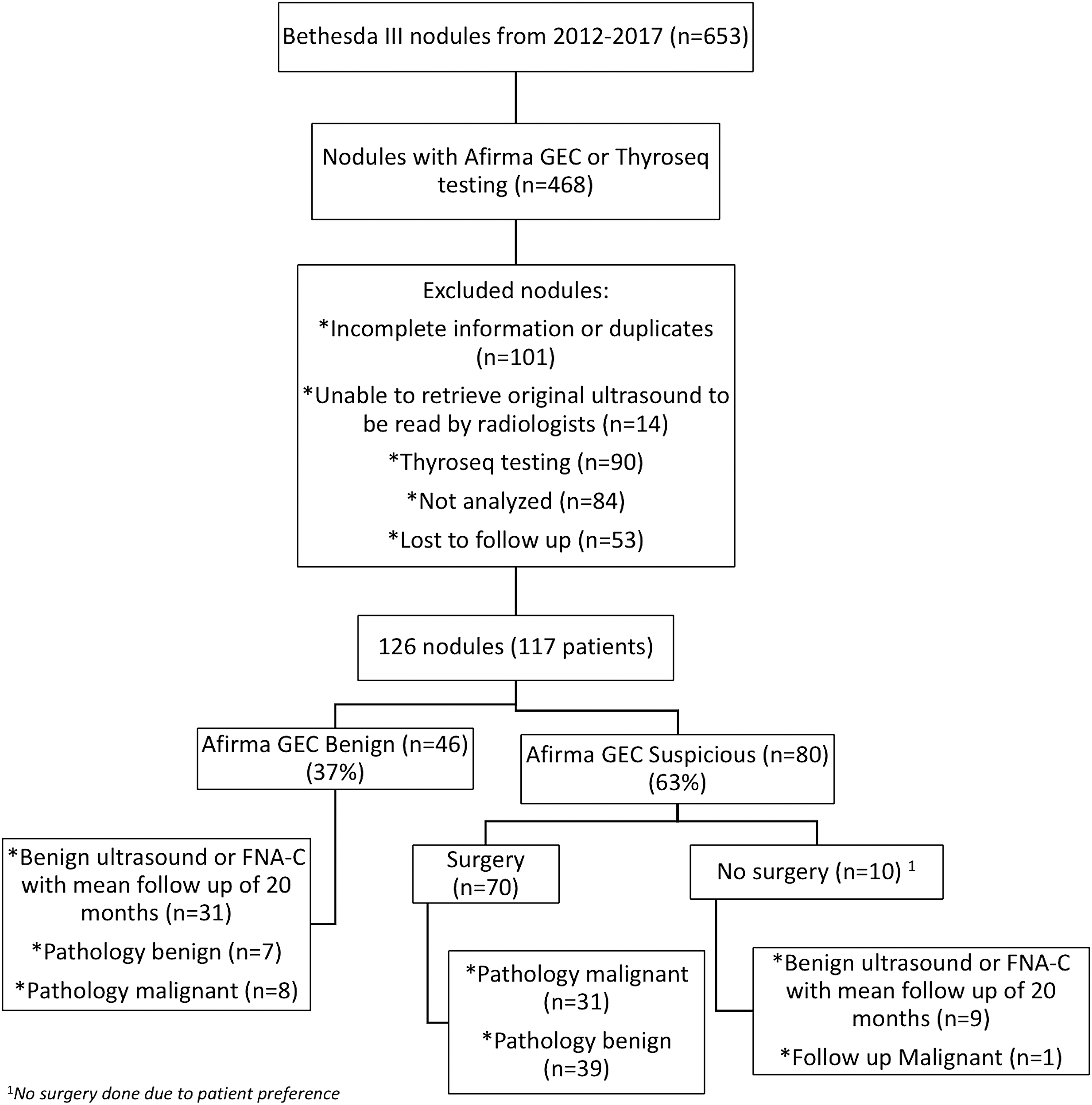
Bethesda III cytology nodules included in the study. Flow diagram showing nodules included in the study cohort. Afirma GEC, Afirma gene expression classifier; FNA-C, fine-needle aspiration cytology; n, number of nodules.
Ultrasound evaluation
Ultrasound images were independently reviewed by three radiologists who were blinded to clinical data, pathology results, and to each other's assessments. Radiologists completed a checklist for each nodule including the nodule location, size, composition, shape, echogenicity, margins, calcifications, and presence of suspicious lymph nodes. Echogenicity was classified into three categories: hypoechoic, isoechoic, or hyperechoic with respect to the normal thyroid parenchyma. Composition was classified into five categories: solid, mixed cystic-solid with >50% solid, mixed cystic-solid with >50% cystic, cystic, or spongiform. Nodule margins were classified into four categories: regular, irregular spiculated, irregular microlobulated, and irregular infiltrative. Calcifications were classified into three groups: none, microcalcifications, and macrocalcifications. Suspicious lymph nodes were classified into two groups: present or absent. The shape of the nodule was classified as taller than wide or wider than tall in the transverse view.
Nodules were classified into the 2015 ATA sonographic patterns as follows. Purely cystic nodules were classified as benign (B). Spongiform or partly cystic nodules without eccentric solid areas or other suspicious features were classified as very low suspicion sonography (VLS). Isoechoic or hyperechoic solid or partly cystic nodules with eccentric solid areas were classified as low suspicion sonography (LS). Hypoechoic solid nodules without other suspicious features were classified as intermediate suspicion (IS) pattern. Solid hypoechoic nodules manifesting at least one suspicious feature (microcalcifications, irregular margins, shape taller than wide, presence of suspicious lymph nodes) were classified as high suspicion (HS) pattern. Radiologist also had the option to select “Non-ATA” as one of the group categories. Non-ATA was recommended to be chosen in the scenarios not described in the 2015 ATA classification; these scenarios included heteroechoic nodules with or without other suspicious features; and isoechoic or hyperechoic nodules with at least one suspicious feature.
Pathology evaluation
All cytology and histopathology results were obtained from chart review and reported at our institution by board-certified pathologists experienced in thyroid cytology and histopathology. Cytology was reported using the Bethesda System for Reporting Thyroid Cytopathology (3). Bethesda III results were reported as either AUS or FLUS. Malignant histopathology results were classified as papillary thyroid cancer, follicular thyroid cancer, or “noninvasive follicular thyroid neoplasms with papillary-like nuclear features”. Afirma GEC results were categorized as “suspicious” or “benign.”
Statistical analysis
Statistical analysis was performed using software Astatsa, Statistical Analysis System version 9.3, and Excel for Mac 2016 with an alpha set to 5%. Demographic characteristics such as age, sex, race/ethnicity, and weight were recorded as well as clinical characteristics such as family history of thyroid cancer, thyrotropin (TSH) level, history of hypothyroidism, cytology (classified as AUS, FLUS, or Hürthle cell neoplasm), GEC result, and surgical histopathology were recorded. In cases in which diagnostic surgery was not performed, data from a minimum 11 months of follow-up with ultrasound were obtained. In accordance with the procedures recommended by a systematic review of studies of Afirma GEC diagnostic performance, we decided to use a cutoff of a minimum 11 months of follow-up of those patients who did not have a surgical histologic diagnosis (22). For these nodules with available long-term follow-up data, those nodules not demonstrating enlargement greater than 3 mm in two dimensions on ultrasound, and those not being subsequently diagnosed as Bethesda category VI on repeat FNA-C were considered as true negative.
Continuous variables are reported with mean ± standard deviation, and categorical data are described with numbers and percentages. Simple t-test was used for continuous data and chi-square test for categorical data. Odds ratios (OR) and associated 95% confidence intervals [CI] were calculated from the contingency tables. Association between ATA sonographic risk category and Bethesda cytology and correlation between ATA sonographic risk category and GEC results were evaluated. Diagnostic performance including NPV and PPV were calculated for GEC overall and when applied within each ATA-US category. Overall PPV and NPV for ATA classification were calculated using HS and IS nodules as a positive test and LS and VLS nodules as a negative test. We used Fleiss k for assessing the reliability of the inter-reader agreement.
Results
Study cohort
One hundred seventeen patients with 126 nodules with Bethesda III cytology were included. Mean age was 58 years at the time of FNA. Eighty percent of patients were female and 46.1% of patients were Hispanic. 3.4% of patients had a history of thyroid cancer, and 11.1% had a history of hypothyroidism. The mean TSH was 1.78 mU/L. Table 1 lists the patient demographics of our study population. Patient age, sex, race/ethnicity, nodule size and location, history of thyroid cancer, and TSH level were not found to be associated with risk of thyroid cancer. Overall malignancy rate was 31.7%. Only ATA-US and GEC were predictive of malignancy.
Demographic and Clinical Characteristics of Study Cohort
SD, standard deviation; TSH, thyrotropin.
Ultrasound
All 126 nodules were able to be classified into an ATA-US category by all readers, and majority consensus was achieved for all nodules as follows: 9 (7%) VL, 48 (38%) LS, 37 (29%) IS, 32 (25%) HS, and 0 (0%) Non-ATA. The mean follow-up was 20 ± 8.85 months (SD 11.2–28.9).
Inter-reader agreement for ATA-US was almost perfect, with Fleiss k of 0.82 [CI 0.77–0.87]. Inter-reader correlation for individual ultrasound features demonstrated substantial to near-perfect agreement: echogenicity k 0.71 [CI 0.65–0.77], composition k 0.87 [CI 0.81–0.93], margins 0.72 [CI 0.63–0.81], and calcifications k 0.85 [CI 0.77–0.94].
Of 126 nodules, 85 had final surgical histopathologic confirmation of diagnosis and 41 had long-term follow-up data (Fig. 1) and were included in the analysis of diagnostic performance of ATA-US and GEC. ROM of HS and IS ATA-US category was 38–44% compared with LS and VLS that had a lower ROM between 11% and 23%. The OR for malignancy for HS/IS versus LS/VLS was 6.66 [CI 1.28–11.44] (Supplementary Tables S1 and S2). Overall PPV and NPV of ATA-US was 40% [CI 0.13–0.32] and 79% [CI 0.64–0.86], respectively.
Among individual ultrasound characteristics, absence of calcifications (OR 0.24 [CI 0.07–0.79]) and irregular margins (OR 2.73 [CI 1.19–6.27]) were associated negatively and positively, respectively, to malignancy risk. All nodules with irregular margins were more likely to be malignant than those with regular margins (OR 2.73 [CI 1.19–6.27]). Predominantly solid nodules (>50% solid) were more often malignant (ROM 35%) compared with cystic and spongiform (ROM 7%), although not statistically significant (Supplementary Table S3). Of the isoechoic nodules, those with irregular margins had a ROM of 47%, while those with regular margins had a ROM of 10% (OR 8.44 [CI 1.48–48.14]) (Supplementary Table S4). Of the cases lost to follow-up (n = 53), 18 (34%) were HS, 13 (25%) were IS, 21 (38%) were LS, and 1 (2%) was VLS.
Afirma GEC
Among all 126 nodules, 37% had benign GEC and 63% had suspicious GEC. The rate of suspicious GEC was highest in the ATA-US high suspicion nodules (69%) and lower among the other sonographic categories (IS 65%, LS 60%, and VLS 56%) (Table 2).
Rates of Suspicious Afirma Gene Expression Classifier by ATA-US Category
ATA-US, American Thyroid Association sonographic risk stratification system for thyroid nodules; Afirma GEC, Afirma gene expression classifier.
Overall PPV and NPV for malignancy of GEC was 40% [CI 0.34–0.55] and 83% [CI 0.70–0.91], respectively, a test performance similar to, yet slightly better than that of ATA-US. The PPV of GEC was higher in the higher risk ATA-US categories and lower in the lower risk sonographic nodules (HS 50%, IS 50%, LS 23%, and VLS 20%). The NPV of GEC was similar across all ATA-US categories and lowest in the very low suspicion sonographic pattern nodules (HS 80%, IS 77%, LS 84%, and VLS 100%). The likelihood of malignancy in the group of nodules with both higher sonographic risk patterns (HS or IS) and suspicious Afirma was significantly greater than in the group of nodules having both low suspicion ultrasound pattern (LS or VLS) with negative Afirma (OR 6.66 [CI 1.7–25]).
Cytology
There was no difference in the ROM, rate of GEC suspicious, and distribution of ATA-US risk categories between nodules with AUS (n = 70) and FLUS (n = 46) cytology. Ten nodules had cytology consistent with Hürthle cell lesions, of which eight were GEC suspicious, while seven were malignant on final pathology. As a group, nodules with Hürthle cell cytology were more likely to have higher suspicion sonographic patterns compared with nodules in the other cytology categories (HS 3, IS 5, LS 1, VLS 1). Supplementary Tables S5 and S6 show the pathology results in benign and malignant nodules per each ATA-US.
Discussion
The results of this study highlight many relevant findings regarding the utility of ATA-US and GEC in the diagnostic evaluation and management of B3 nodules. First, our results demonstrate that B3 nodules were able to be categorized into an ATA-US category with a high level of inter-reader agreement. As there is no consensus definition of what the “Non-ATA” sonography pattern encompasses, it was not chosen often by the radiologists and none of the nodules received a consensus designation of Non-ATA. This is in contrast to prior reports concluding that 20–37% of ITNs could not be easily categorized into one of the five ATA sonographic risk patterns (14,19,23) and the conflicting results of the few studies of inter-reader agreement among sonographers using ATA-US in ITNs (24 –26).
A second major finding of this study is the association between higher risk ATA-US patterns and suspicious GEC. Over two thirds of nodules with high suspicion sonography were found to be suspicious on GEC, and GEC suspicious nodules were more likely than GEC benign nodules to be categorized into one of the higher sonographic risk patterns.
The most important and clinically relevant findings garnered from this study regarding GEC and ATA-US as diagnostic tests in B3 nodules are (i) The diagnostic performance of ATA-US is similar to and only slightly inferior to that of GEC, (ii) Certain individual sonographic features such as border characteristics or microcalcifications may perform as well or better than ATA-US in predicting malignancy or benignity, (iii) The PPV of GEC varies across ATA-US categories, while the NPV remains fairly constant except for in the very low suspicion sonographic pattern nodules in which the NPV of a benign GEC result was 100%, and (iv) In isoechoic B3 nodules, which by definition are low suspicion ATA-US, the presence of infiltrative margins is a predictor of malignancy.
The optimal approach to management of thyroid nodules with Bethesda category III cytology remains controversial. While molecular tests including GEC have been widely used to risk stratify such nodules these tests are relatively expensive and may not be available for all patients in all settings. It has been proposed that ATA-US can be used to risk stratify ITNs and to select which nodules should undergo molecular testing, with some authors advocating for performing molecular tests only in ITNs with LS or IS ATA-US category and others suggesting that all ITNs with high suspicion ATA-US undergo surgical management while the remainder be submitted for molecular tests (3,21). Furthermore, no studies to date have assessed the diagnostic performance of molecular tests including GEC within each ATA-US category and whether GEC test performance is different when applied to nodules of varying sonographic risk patterns. Based on the findings of our study in which the ROM in ATA-US HS pattern nodules was only 41% and in which GEC retained its NPV in this category, we suggest that GEC could be utilized in B3 nodules across all ATA-US categories, while perhaps given their low overall ROM consideration to forego molecular testing in lieu of a strategy of close surveillance could be appropriate for B3 nodules with very low sonographic risk patterns.
To the best of our knowledge, this study is first to demonstrate that the PPV of GEC varies with ATA-US category, while the NPV remains similar across the higher risk sonographic categories and low ATA risk sonographic risk B3 nodules with a 100% NPV when applied to ATA very low suspicion nodules. These findings require further validation in larger multicenter trials.
Recent reports have brought into question the applicability of the diagnostic test performance of Afirma GEC as shown in the initial validation study to real-world practice, and some have suggested that the NPV of GEC may be lower in many of the populations it is currently applied in (11). Consistent with this idea, we have found an overall NPV of GEC of 83% following a methodology outlined in a consensus article outlining a strategy for calculating test performance for Afirma GEC (22). Even if we were to assume that all GEC test negatives were true negatives, we found 8 malignancies among our total cohort of 74 negative GEC cases which would provide an NPV of 89%, lower than the 95% NPV reported in the original validation study (4). We recommend that B3 nodules with benign GEC results not having very low risk sonographic features be surveilled more closely than thyroid nodules with benign cytology. In recent years, the Afirma GEC has been replaced by Afirma Gene Sequencing Classifier with improved diagnostic performance (27). Based on findings of our study regarding GEC, we suggest that further studies be performed to assess the test performance of GSC within each ATA-US category.
Limitations of our study include that this was a single-center study and that not all patients underwent final surgical histopathologic confirmation of diagnosis or had long-term follow-up. Strengths of our study include the blinded nature of sonographic data collection and the high-inter-reader agreement among three radiologists.
Our findings suggest that ATA-US may have similar to slightly inferior diagnostic performance compared with GEC and that the combination of information from ultrasound and GEC may alter the performance of GEC for the diagnosis of B3 nodules. We propose that in circumstances in which molecular testing is not available sonographic risk assessment may be used to risk stratify B3 nodules. Similar to prior reports, we have found that the NPV of GEC may be lower than previously reported and perhaps too low to reliably avoid the need for diagnostic surgery for most B3 nodules. Further research is needed regarding the use of ultrasound risk stratification systems to inform the performance and interpretation of molecular tests commonly utilized in the diagnosis of ITNs. Large multicenter prospective studies are needed to more definitively assess whether performance of molecular tests are altered by sonographic risk category in thyroid nodules with indeterminate FNA cytology.
Footnotes
Acknowledgments
We thank Dr. Jay Sosenko, Dr. Hua Li, and the University of Miami Biostatistics Collaboration and Consulting Core (BCCC).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6