
Abstract
Background:
Thyroid cancer (TC) incidence rates have been increasing in many countries, predominantly due to overdiagnosis. It is, however, not yet clear whether a true increase in exposure to risk factors might have also contributed to the TC epidemic. We assessed the TC mortality trends, which should not be affected by overdiagnosis, to disentangle the specific contribution of period and cohort effects.
Methods:
We analyzed long-term mortality data in 24 countries from 5 continents using age–period–cohort (APC) models. Nonidentifiability of the APC models was circumvented by integrating evidence of a consistent relationship between age and TC mortality, allowing to estimate period and cohort linear effects.
Results:
Substantial heterogeneity existed in the historical TC mortality rates across countries, but long-term rates declined over time in most of the countries, converging around a value of 0.5/100,000. The shape of the age–specific curves was consistently similar across countries and periods, resembling straight lines on the log–log scale, with the slopes ranging between 4.0 and 6.0. Both period and cohort effects showed long-term declines in most countries for both genders. In some countries, such as the United States, Canada, and Australia, substantial long-term declines by period were visible until the 1980s and 1990s, but then stabilized or increased slightly. Declining cohort effects were also seen in almost all countries, and were particularly pronounced in women from Switzerland, whereas stable cohort effects were recorded in South Africa. Although there were some indications of possible increasing risks of deaths among the youngest generations in some countries for both men and women, changes are too recent to be treated as unequivocal and estimates suffered from large statistical variability due to small numbers of deaths.
Conclusions:
Global long-term declines in TC mortality have been accompanied by downward trends in both period and cohort effects. Our results suggest lack of evidence of a possible major contribution of “real” risk factors in TC mortality, and indirectly confirm the main role of overdiagnosis in the epidemic of TC incidence.
Introduction
Thyroid cancer (TC) incidence rates have been rapidly increasing in many high- and middle-income countries (1,2), although with substantial variability between and within populations. In several countries, including the United States, France, and Italy, incidence rates in women have doubled or tripled within only a few decades, and in the Republic of Korea, incidence rates in 2012 were ninefold those in 1999, leading TC to be the most common female cancer currently diagnosed in that country (3). In contrast with the major increases observed for incidence, long-term TC mortality declined almost everywhere (2), or remained relatively stable at very low levels, even though possible small increases have been reported in the most recent period in the United States (4).
The steadily diverging gap between TC incidence and mortality rates suggests a major role for overdiagnosis, that is, the diagnosis of cancers that would not cause symptoms or death if left untreated. The progressive introduction of new diagnostic techniques and increased surveillance have likely led to a massive detection and diagnosis of a large reservoir of indolent lesions of the thyroid known to exist in the general population (5,6). It is, however, not yet clear whether a true increase in exposure to risk factors might have also contributed to the TC epidemic.
Age–period–cohort (APC) models can provide useful information when modeling cancer trends, allowing to account for processes occurring on the three interrelated timescales. Period effects are usually a surrogate for risk factors that similarly affect all age groups, whereas cohort effects can represent changes in risk factors occurring across different generations. Generally, cancer risk increases with age, but for TC incidence this relationship has been gradually distorted in the past decades due to the progressively stronger diagnostic pressure and overdiagnosis of middle-aged individuals. The shape of the age-specific incidence curves changed dramatically over time, from an approximately exponential-like, to an inverse U-shaped curve (1), thus making difficult to detect and interpret variations in TC incidence occurring over the two other timescales, that is, period and cohort.
A detailed assessment of TC mortality trends, which should not be affected by overdiagnosis, could therefore provide useful information to understand a possible impact of “real” risk factors. Of particular interest would be to clarify and disentangle the specific contribution of period and cohort effects on TC mortality trends. We have therefore carried out an international APC analysis by using the most up-to-date data spanning over at least three decades.
Materials and Methods
Data sources
TC mortality data by age group (ranging from 25 to 84 years), year of death, gender, and country were obtained from the World Health Organization (WHO) mortality database (7). TC deaths were extracted using International Classification of Diseases (ICD): ICD-7 (194), ICD-8 (193), ICD-9 (193), and ICD-10 (C73). Countries were included in our study if they could provide at least 30 years of available data and at least 5 million person-years of observation annually over the study period. This selection identified 22 eligible countries. Despite the shorter time span of data (20 years), we also included the Republic of Korea, given the exceptionally rapid increase and currently high level of TC incidence rates, and South Africa, to represent the African continent. Finally, 24 countries in 5 continents were included in our analyses. Denmark, Norway, Sweden, and Finland were grouped and analyzed together as Nordic countries.
Population coverage of the mortality database was nearly 100% in all selected countries, with the exception of South Africa (91%) (8). The time span of study periods for each country varied from 20 to 60 years, and analyses were restricted to ages 25–84 years. Data were aggregated and analyzed by 5-year period and age groups. When missing data for certain years were found in some countries, the mortality rate was replaced by the average value of the corresponding 5-year period.
Population data were obtained from the same sources, except for Canada, the United States, and South Africa for which the WHO data were incomplete for the study period and were therefore derived from the United Nations World Population Prospects (9).
Statistical analysis
Age-standardized mortality rates (ASMRs) of TC by gender and country were computed using the world standard population as a reference (10). ASMRs versus 5-year periods were plotted on a semilogarithmic scale (11) and smooth lines were added using LOESS, a nonparametric method that uses local weighted regression to fit smooth curves through points (12). We have estimated the average annual percent changes (AAPC) between 1986 and 2015 as
We calculated the mortality rates for each 5-year age group and 5-year period, and the corresponding birth cohort as the difference between midpoints of period and age group. The general form of the APC model is as follows:
where
TC mortality rates increased approximately exponentially with age, for each country, period, and gender, which implies that the relationship between
Results
ASMRs of TC
Table 1 shows the annual average number of TC deaths, person-years, and corresponding ASMRs for the period 2011–2015. ASMRs in 2011–2015 were always below 1/100,000 in all countries and both sexes. The highest rates were observed in Israel (0.89/100,000 and 0.79/100,000 for women and men, respectively); the lowest in France and Switzerland for women (0.38/100,000) and South Africa for men (0.29/100,000). The female-to-male ratios of ASMRs in 2011–2015 were close to 1 in most countries, with highest value found in South Africa (1.7) and the lowest in France and Switzerland (0.8).
Populations Included in the Analyses, Observation Periods, Number of Deaths, Person-Years, Age-Standardized Mortality Rates, with Corresponding Relative and Absolute Temporal Changes, and Sex Ratios of Thyroid Cancer, Age 25–84 Years
Average annual number of cases and person-years (expressed in million person-years at risk) obtained for the most recent 5-year period 2011–2015 for all countries, except for France, Switzerland, and Bulgaria, where the corresponding periods were 2011–2014.
AAPCs of ASMRs between 1986 and 2015, except for the Republic of Korea and South Africa (1996–2015); France, Switzerland, and Bulgaria (1986–2014).
The reference periods were 1986–1990 in most countries, except for the Republic of Korea and South Africa (1996–2000).
AAPC, average annual percent change; ASMR, age-standardized (world population) mortality rate; CI, 95% confidence interval; F/M ratio, female-to-male ratio of ASMRs.
Trends of TC mortality
Time trends of ASMRs over the study period were plotted (Fig. 1). The estimated relative and absolute changes between 1986–1990 (a time period not coinciding with the beginning of the study period) and 2011–2015, as well as absolute changes between 2006–2010 and 2011–2015, with corresponding 95% confidence intervals (CIs), are displayed in Table 1. Major long-term declines are observed in the majority of the countries. Substantial heterogeneity existed in the historical mortality rates, but declines were found in most countries, stabilizing and converging around a value of ∼0.5/100,000 in both sexes. In Canada, the United States, and Australia, the downward trends leveled off or slightly increased since around the 1990s in both sexes. A similar behavior was also seen in Greece and Portugal, although estimates for the latter suffered from a relatively large variability.
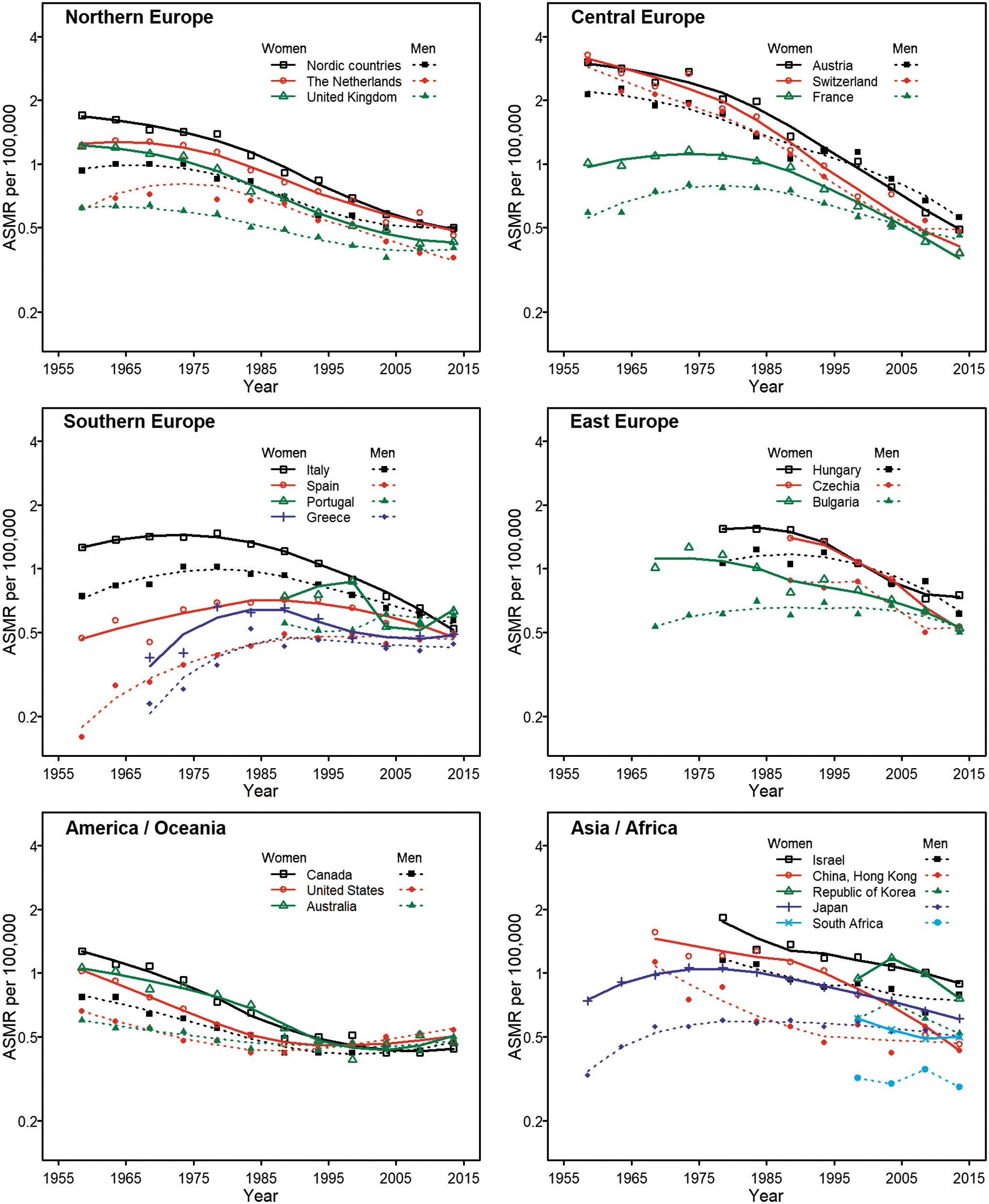
Temporal trends of ASMR per 100,000 of thyroid cancer by geographic region, on a semilogarithmic scale. ASMR, age-standardized mortality rate. Color images are available online.
Countries with the highest historical mortality levels and with the largest decrease in ASMRs were Switzerland and Austria, where ASMRs in women have declined from 3.28/100,000 and 3.03/100,000 in 1956–1960 to 0.38/100,000 and 0.49/100,000, respectively, in 2011–2015, and in men from 3.06/100,000 and 2.13/100,000 to 0.48/100,000 and 0.56/100,000, respectively, during the same period. The fastest annual declines from 1986–1990 to 2011–2015 were observed in women from Switzerland (−0.87%), Austria (−0.83%), Czechia (−0.82%), China-Hong Kong (−0.75%), France (−0.74%), Italy (−0.66%), and Hungary (−0.63%) (Table 1). In men, declines were generally slower than in women. The fastest declines in men from 1986–1990 to 2011–2015 were observed in Switzerland (−0.66%), Austria (−0.57%), Czechia (−0.48%), the Netherlands (−0.47%), and Hungary (−0.44%). Small, but statistically significant, annual increases from 1986 to 2015 were observed in the United States in both sexes (AAPC: 0.06%, CI: 0.01–0.12 in women and 0.21%, CI: 0.19–0.23 in men), and in Canada in men (AAPC: 0.08%, CI: 0.02–0.13). With respect to the most recent periods, ASMRs for 2011–2015 were lower than in 2006–2010 in most countries and no statistically significant increases were observed.
Evidence for a unique age-specific curve for TC mortality
The shape of the age-specific curves was consistently similar across countries and periods, approximately resembling a straight line on a log–log scale in most countries, even though some instability of the shape was observed in certain countries due to small numbers (<20 average annual TC deaths), such as in Switzerland and China-Hong Kong (Supplementary Figs. S1 and S2). The pooled slope across all periods ranged between 4.0 and 6.0 depending on the country. Similar results were found when data intervals for period and age were grouped by 10-year, instead of 5-year, intervals (Supplementary Table S1).
APC models: unique estimates of period and cohort effects
Figures 2 and 3 show the estimates of period and cohort effects on TC mortality as estimated by the APC analyses, in women and men, respectively. In women, particularly strong long-term period declines were observed in all the Northern, Central, and Eastern European countries, and in Italy, whereas in other Southern European countries, period effects have been rather stable or have slightly increased, such as in Spain, Portugal, and Greece. Moderate declines in period effects were seen in Asian countries. In the United States, Canada, and Australia, declines by period were strong up until the 1980s and 1990s, but then stabilized and eventually increased slightly in the most recent period. Hints of stabilizing trends by period were found after 2000s in the Nordic countries, the United Kingdom, the Netherlands, and Hungary.
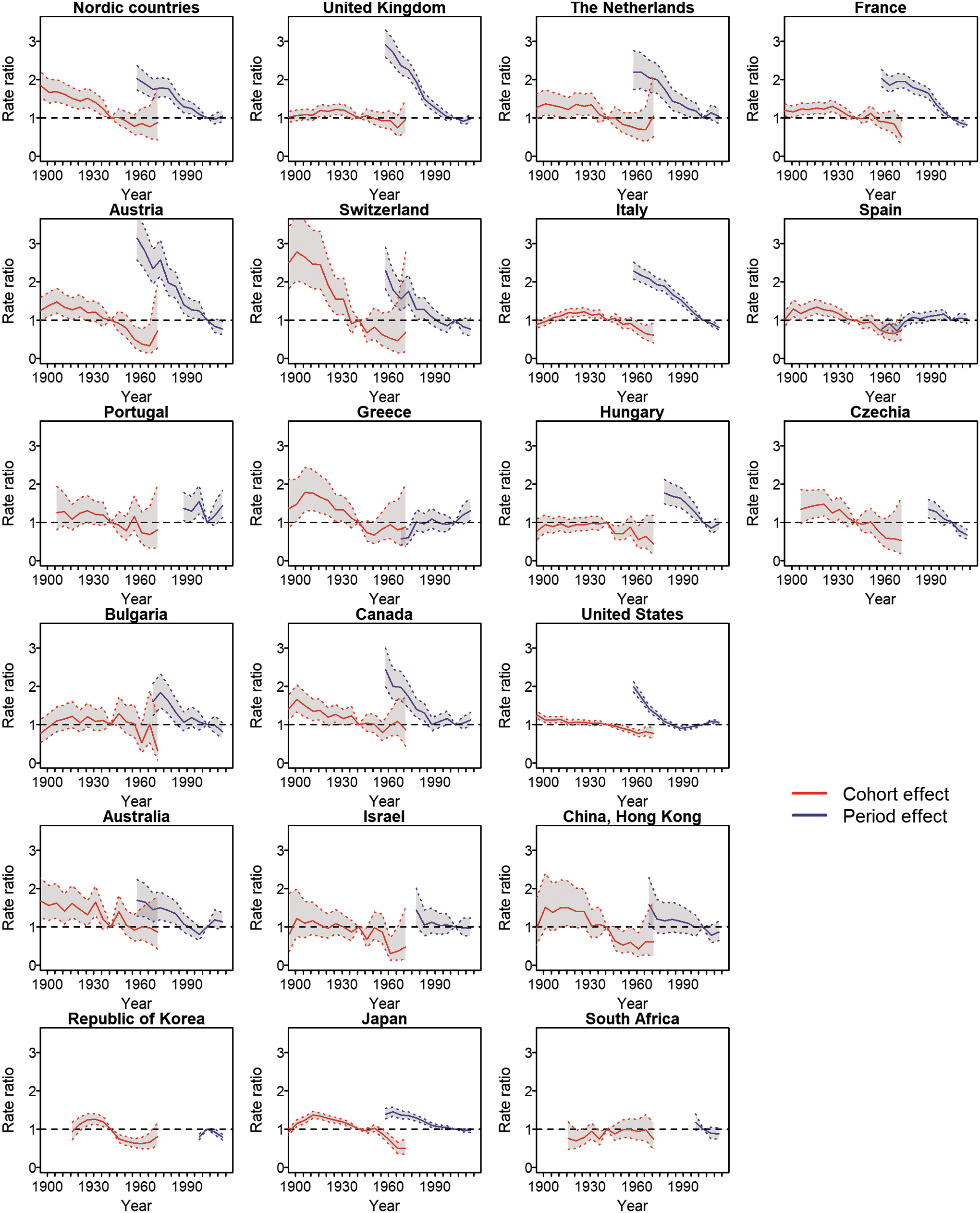
Age–period–cohort analysis of thyroid cancer mortality trends in women. The reference period and birth cohort is 2001–2005 and 1939–1943, respectively. The shaded areas represent 95% confidence intervals (CIs). Age is not shown because its effect was constrained to be linear on the log–log scale. Color images are available online.

Age–period–cohort analysis of thyroid cancer mortality trends in men. The reference period and birth cohort is 2001–2005 and 1939–1943, respectively. The shaded areas represent CIs. Age is not shown because its effect was constrained to be linear on the log–log scale. Color images are available online.
Cohort effects were generally declining in all countries, with the possible exception of South Africa, where the trends were rather stable. Long-term cohort decreases were less pronounced than period declines in most countries in Europe and America, with the exception of Switzerland where the decline across successive generations in individuals was particularly pronounced. In some countries, such as Hungary, Bulgaria, and Israel, cohort-specific declines were only seen starting from generations of women born after the 1940s. There were indications of possible increasing TC mortality for the youngest generations (born around 1960s) in some countries, including the Netherlands, Austria, Switzerland, Israel, China-Hong Kong, and the Republic of Korea, but estimates were unstable and CIs wide (Fig. 2). The declining patterns of period and cohort effects in men were generally similar to those observed in women, although less pronounced (Fig. 3).
Discussion
Our study presents a comprehensive and up-to-date assessment of time trends of TC mortality, highlighting changes over the three major temporal components of time, age, and calendar period and birth cohort. We found that secular, global declines in TC mortality have been generally accompanied by parallel long-term decreases over period of death and successive birth cohorts. Thus, while caution is necessary when interpreting descriptive cancer data, this international comparison overall suggests lack of evidence of major increasing risks of TC mortality by period and by birth cohort for the majority of the studied countries, including France, Italy, and the Republic of Korea, that have experienced remarkably high increases in TC incidence in the past decades.
We have found that the shape of the age-specific curves of TC mortality was similar across countries and did not substantially change over time. TC death rates increased exponentially with age, a behavior common to other epithelial cancers (14) and, importantly, also to the incidence of TC in periods before the widespread use of modern diagnostic techniques (1,15). The approximately constant shape of the age-specific curves for TC mortality contrasts with that for TC incidence, which progressively changed over time, gradually resembling an inverted U-shaped curve, likely as a result of increased screening and diagnostic pressure in middle-aged individuals (16). The knowledge of the relative consistency of the shape of age-specific curves for TC mortality was also useful to circumvent the nonidentifiability of APC models (17).
Overall, this study shows that global TC mortality trends have been driven by declines over both period and birth cohort. The steepest historical declines by period have been observed in regions with particularly high past levels of iodine deficiency, endemic goiter, TC mortality, and with the earliest implementation of iodine supplementation programs, in North and Central Europe, the Alpine region, including Austria, Switzerland, and Italy, and the United States. Chronic iodine deficiency and goiter are strong risk factors for TC, particularly for follicular and anaplastic TC (18,19). In fact, several epidemiological studies have shown a significant decrease in the incidence of anaplastic TC (the most lethal subtype of TC) after the introduction of iodized salt in Slovenia, Italy, and Sweden (20 –22). In Switzerland, the significant decrease in the incidence of anaplastic TC after the introduction of iodized salt has been considered a factor that contributed to the marked decrease in TC mortality from 1921 to 1978 (23). It is thus possible that the downward period trends could be driven by the progressively declining levels in iodine deficiency in individuals of all ages. Another factor that may contribute to the decline in TC mortality is death from competing causes. With increased diagnosis of small- and low-risk TC, it is possible that patients are less likely to die from TC, and more likely to experience noncancer events as the cause of death, such as cardiovascular disease (24). In addition, lower TC mortality rates could also be attributed to a better ascertainment of cause of death. Methods of causes of death have improved over time due to a more complete and adequate record information. It is possible that a patient with metastatic TC could have his/her death attributed incorrectly to TC if records, explaining that metastatic disease is stable and nonlife-threatening, are not available at time of the ascertainment of cause of death. Other possible reasons such as improvements in treatment over the past decades, likely affecting in a similar way patients of all ages, may have also contributed to the downward period effects.
Cohort effects have also been declining in the long term in most of the countries, and the most recent generations overall did not have a higher risk of dying of TC compared with their older fellow citizens born during the first half of the 20th century. The reasons behind the trends are not clearly understood, but overall they suggest lack of a major impact of exposures to known or new risk factors. There were hints of possible small increases in TC mortality for the youngest generations of both genders (born around 1960s) in some countries, such as the United States and Canada. Although we cannot exclude a possible recent impact of certain risk factors, such as the progressively increased exposure to medical ionizing radiation, particularly in childhood and adolescence, changes are too recent to be treated as unequivocal. In some countries, we cannot exclude that because of the dramatic increase in incidence, a certain number of deaths could have been erroneously attributed to TC in individuals diagnosed with this type of cancer but who died from other causes. Nevertheless, interpretation should be made with caution, particularly because the most recent cohorts, as opposed to other cohorts, can contribute only with the youngest age group, for which the number of cases is very low, thus causing a large variability in the later birth cohorts with unstable estimates and wide CIs.
The long-term declines of TC mortality stabilized and eventually converged to similar contemporary values in the large majority of the studied populations, even in those with formerly high death rates. It is still unclear whether this could be possibly considered the currently lowest level of mortality comprising all TC cases with the worst prognosis (25). Declines in ASMRs have been relatively gradual, without evidence of sudden changes. Importantly, patterns by period and cohort have been similar across sexes, although declines were generally more pronounced in women than in men, thus leading to similar recent values of mortality by sexes, as evidenced by the values of the female-to-male ratios closer to 1. The relative uniformity of the declines and patterns of TC mortality across countries and genders contrasts with the striking but heterogeneous increases observed for TC incidence worldwide (6), and confirms that most of the increase in TC incidence is due to overdiagnosis.
Our study has some limitations. First, information on TC subtypes is not available in the mortality database. The possible variation in mortality trends of different subtypes may influence the time trends of overall TC mortality. Second, although many countries from different parts of the world were included in this study, long-term data were not available for many low- and middle-income countries, and it is unclear whether the results of this study may represent sufficiently well other settings.
The strengths of the present study include the fact that, contrary to incidence, which is largely influenced by overdiagnosis, a proper assessment of the mortality patterns can provide the most appropriate perspective to inspect whether real “risk factors” are behind the current TC epidemic. The study benefits from a new approach to circumvent the nonidentifiability problem in the APC model and to estimate period and cohort linear effects, based on integrating information on the shape of age curves.
In conclusion, the global declines in TC mortality have been accompanied by long-term decreases over both calendar periods and birth cohorts, suggesting lack of evidence of a possible major contribution of “real” risk factors in TC mortality, and indirectly confirming the main role of overdiagnosis in the epidemic of TC incidence.
Disclaimer
The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions, or policies of the institutions with which they are affiliated.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Institut National du Cancer (INCa), France (Grant No. 2017-138).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1