
Abstract
Background:
The 2015 American Thyroid Association (ATA) guidelines proposed a three-category system for estimating the risk of recurrence of differentiated thyroid carcinoma (DTC). This system includes several perioperative features, but not age at diagnosis. However, age has traditionally been recognized as a critical factor in the survival of DTC patients, and the eighth edition of TNM stated that patients older than 55 years were at higher risk of death. In this study, we raised the question of whether age at DTC diagnosis impacts on its risk of recurrence. Specifically, the present study aimed to (i) evaluate the association between age at diagnosis and structural recurrence and (ii) investigate whether age at diagnosis could improve the performance of the ATA system.
Methods:
During the study period, four institutions selected DTC patients treated with both thyroidectomy and radioiodine and who had follow-up for at least one year. Patients with proven structural evidence of disease during follow-up were identified, and disease-free survival (DFS) was calculated accordingly.
Results:
The study involved 1603 DTC patients with a median age of 49 years and DFS of 44 months. Disease recurred in 8%. The shortest DFS was found in the oldest patients. The Kaplan–Meier curves were calculated for each decade of age, and there was a significant association with DFS (p = 0.0014). Patients older than 55 years had significantly higher risk (hazard ratio [HR] 1.78, 95% confidence interval [CI 1.23–2.56]). The Kaplan–Meier curves of DFS in high-, intermediate- and low-risk groups showed a significant association only in the high-risk group (p = 0.0058). Patients older than 55 years had significantly higher risk of relapse over time only in the high-risk group (HR 2.15 [CI 2.01–4.53]). Cox's proportional analysis showed that the age cutoff of 55 years and the ATA system were significant predictors of relapse. Adding age at diagnosis above 55 years to the ATA system identified a subgroup of patients at highest risk for relapse.
Conclusions:
The age threshold adopted in the eighth edition of TNM staging system for DTC patients' prognosis also identifies cases at higher risk of relapse. Applying age at diagnosis, with a cutoff of 55 years, to the ATA risk stratification system identifies cases at highest risk of relapse.
Introduction
Thyroid cancers are the most prevalent malignant endocrine tumors. Among all thyroid malignancies, differentiated thyroid carcinomas (DTCs) are the most common and are recognized as indolent cancers. Indeed, while 5–20% of DTC patients suffer cancer relapse after the initial treatment, only a small number of patients die from their disease (1).
After diagnosis, DTC patients are staged according to the TNM staging system (2). This staging system is based on the initial histological/imaging information (i.e., size of the primary cancer, invasion of nearby tissues, regional lymph node involvement, and distant metastases). In DTCs, in addition to the above features, age at the time of diagnosis plays a major role in prognosis. Indeed, the most recent edition of the TNM staging manual stated that patients older than 55 years were at higher risk of death (2,3). Although the TNM was originally conceived as a tool for stratifying the risk of disease-specific death in patients affected by malignant tumors, in clinical practice, it has also been frequently used to assess the risk of cancer relapse and to guide follow-up. In the field of thyroid cancer, this is due to two main reasons: the low rate of DTC-specific death and the lack of alternative systems for identifying patients at high risk of recurrence. However, as the TNM system is thought to identify patients at risk of death, this use is debatable.
To fill this gap, the American Thyroid Association (ATA) guidelines published in 2015 proposed a three-category (high risk, intermediate risk, low risk) system for estimating the likelihood of DTC developing a structural recurrence during postoperative follow-up (1). This risk assessment, in addition to some TNM features, includes perioperative data (i.e., aggressive or nonaggressive histological subtype, extension of invasion, completeness of tumor resection, presurgical evidence of suspicious neck lymph nodes, and number and size of neck lymph nodes removed) and further molecular analyses (i.e., BRAF, TERT mutation). In brief, according to the ATA guidelines, DTCs with gross extension are at high risk for recurrence, intrathyroidal DTCs with nonaggressive histology are at low risk, and the remaining DTCs are classified as being at intermediate risk. While age at diagnosis has traditionally been recognized as a critical factor in the survival of DTC patients, some questions arise. Does age at DTC diagnosis actually have an impact on the risk of recurrence after the initial treatment? Moreover, can age at diagnosis improve the predictive model of the ATA risk stratification system?
The present study was undertaken to evaluate the impact of age at diagnosis on DTC relapse in a large retrospective multi-institutional cohort. Specifically, the main outcomes of this study were to (i) evaluate the association between age at diagnosis and structural recurrence in DTCs and (ii) investigate whether age at diagnosis can improve the ATA risk stratification system of these patients.
Materials and Methods
Study design
Four institutions participated in the present multicenter survey: three from Italy (Galliera Hospital in Genoa, S. Andrea Hospital in Rome, and Regina Elena National Cancer Institute in Rome) and one from Switzerland (Ente Ospedalero Cantonale in Bellinzona). At our institutions, DTC patients are seen annually after initial treatment. The study design was a retrospective analysis that included DTC patients treated and followed up at our institutions and evaluated for their annual visit during the period of January to December 2018. The inclusion criteria were patients diagnosed and treated with both thyroidectomy (plus lymph node neck dissection when necessary) and radioiodine (RAI). Patients younger than 18 years at diagnosis, with incidental microcarcinomas, with initially unresectable DTC, with a follow-up period shorter than one year, and/or with incomplete follow-up data were excluded. The cases included were classified according to the ATA guidelines for risk assessment (1). This study was reviewed and approved by all local institutional review and ethical boards.
Reference standards of the study
Patients were classified as alive with no evidence of disease (NED) if there was no clinical, imaging, or cytological/histological evidence of disease and their measured basal thyroglobulin (Tg) levels were undetectable (i.e., below the functional sensitivity of the locally used assay) or, if detectable, were less than 1 ng/mL and decreased or remained unchanged over time. Patients with structural evidence of disease proven by cytology/histology and/or functional imaging findings with increased Tg were deemed to have structural recurrence (REC). Structural disease-free survival (DFS) was calculated from the date of RAI to the date of the last follow-up examination in NED patients, and from the date of RAI to the date of detection of structural relapse in REC patients.
Statistical analysis
The Mann–Whitney U, Wilcoxon test, and paired or unpaired t-test were used to analyze differences between paired or unpaired variables in the two groups of patients. DFS was estimated by means of the Kaplan–Meier method, and differences between curves were analyzed by the log-rank or Mantel–Cox test and expressed as hazard ratios (HRs). Cox's proportional hazards model was performed in univariate and multivariate analyses to evaluate the effect upon time of any potential predictor of cancer relapse (expressed as the HR). Continuous variables are reported in the text as medians and interquartile ranges. Statistical significance was set at p < 0.05. Statistical tests were performed using MedCalc Statistical Software, version 15.8 (MedCalc Software bvba, Ostend, Belgium) or GraphPad Prism version 8 (GraphPad Software, San Diego, CA).
Results
Demographic data
A total of 1603 DTC patients were finally enrolled, 74% of whom were female. The median age at diagnosis was 49 years. The median DFS was of 44 months. Papillary (papillary thyroid carcinoma) was the most prevalent cancer type, while follicular (follicular thyroid carcinoma) and oncocytic (oncocytic thyroid carcinoma) carcinomas accounting for ∼10% of cases. High-risk cases accounted for 5% of the total cohort. Recurrences occurred in 8.3% of cases. Table 1 summarizes the clinicopathological features of the study cohort.
Clinicopathological Characteristics of the Study Cohort
Values in parentheses of median age and disease-free survival represent the interquartile range. All the other parameters are reported as number (percentage).
ATA, American Thyroid Association; FTC, follicular thyroid carcinoma; OTC, oncocytic thyroid carcinoma; PTC, papillary thyroid carcinoma.
Analysis of age as a risk factor for structural recurrence
The median age of patients with REC (52 years, 39–66) was significantly (p = 0.010) higher than that of NED patients (48 years, 39–57). Two-thirds of patients were between 31 and 60 years at diagnosis; 20% of patients were older and 10% were younger. When the overall series was stratified according to age at diagnosis, the median DFS was longest in the youngest subgroup (54 months) and shortest in the oldest subgroup (38 months). The lowest rates of recurrence were found in patients aged 31–50 years, while those older than 70 years had the highest rate. Among patients aged 18–30 years, the rate of REC was 16.87% in the 18- to 25-year-old subgroup and 7.45% in the 26- to 30-year-old subgroup (p = 0.089). Table 2 summarizes the details of these subgroups.
Analysis of Differentiated Thyroid Carcinoma Patients by the American Thyroid Association Risk Stratification System and Age
DFS, disease-free survival.
When the Kaplan–Meier curves were calculated for each subgroup of age at diagnosis, a significant difference was found (Fig. 1A). The subgroup of patients aged 31–40 years showed a lower risk than that of the subgroup aged 18–30 years. Patients older than 70 years at diagnosis had a shorter DFS than those aged between 61 and 70 years. All other comparisons showed no significant differences. As shown in Figure 1B, patients older than 55 years had a significantly higher risk of relapse than those younger than 55 years, with a median DFS of 41 and 47 months, respectively. No significant difference was found when comparing patients older than or younger than 45 years (Fig. 1C).

Kaplan–Meier curves for all decades of age at diagnosis (
Performance of the ATA risk stratification system in predicting relapse
The median age at diagnosis in the three groups was 53 years in the high-risk patients, 49 years in the intermediate-risk patients, and 47 years in the low-risk patients. A significant difference was found only between the low-risk and high-risk groups (p = 0.0032). The Kaplan–Meier curves of DFS in the three groups were compared, and a significant difference was found (p < 0.0001).
The inclusion of age at diagnosis showed different impacts in the three different ATA risk groups. In the high-risk group, an age at diagnosis >55 was able to further stratify the population, and patients older than 55 years had a significantly higher risk of recurrence than that of the younger (<55 years) patients (Fig. 2). Importantly, the high-risk <55-year-old patients showed no difference in the risk of relapse than the whole group of intermediate-risk patients. No significant differences were found between age subgroups in the other two ATA (low-risk and intermediate-risk) categories.
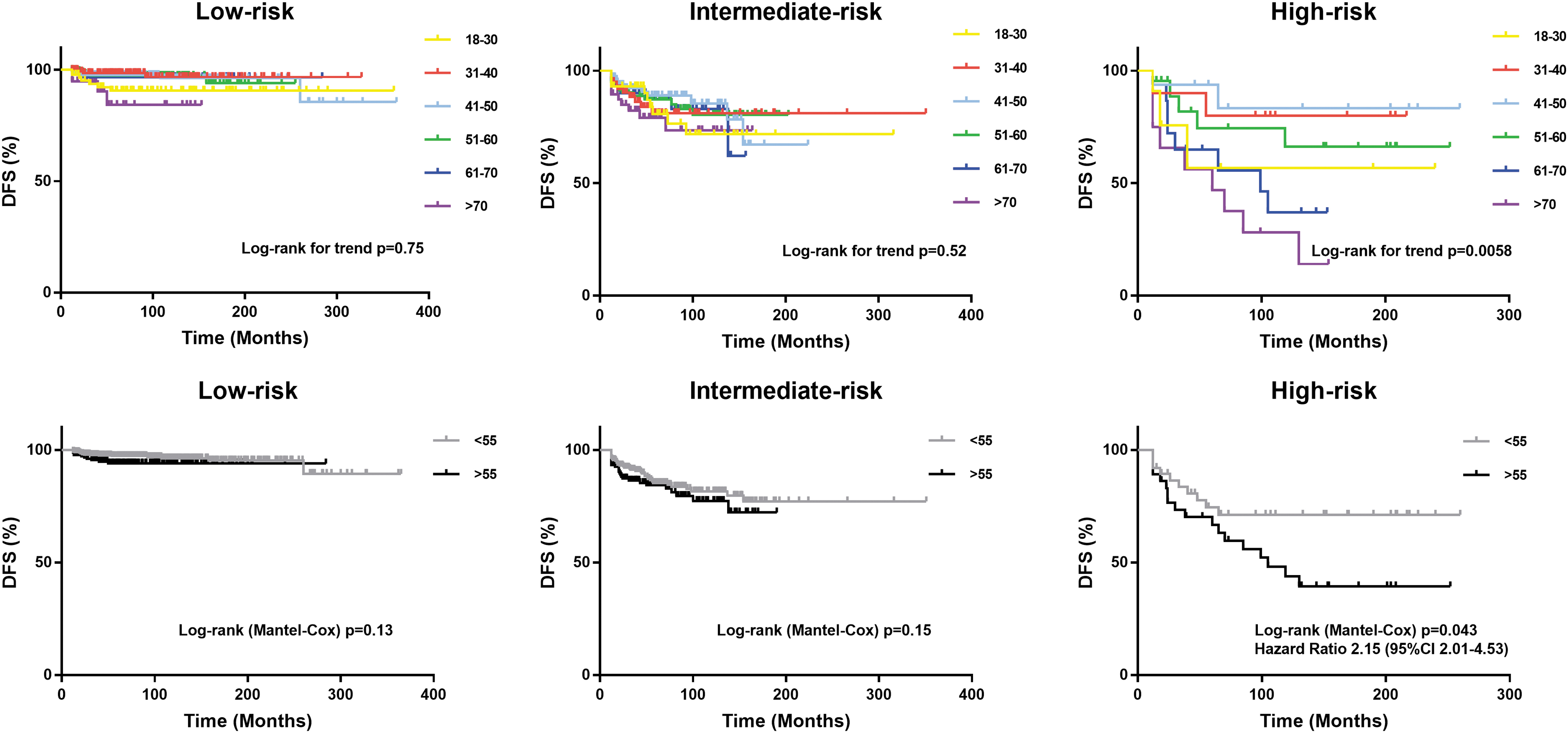
Kaplan–Meier curves for DFS in DTC patients according to their ATA risk category. In the upper panel, patients were divided on the basis of their decade of age at diagnosis. In the lower panel, patients were divided into two groups according to age at diagnosis below or above 55 years. ATA, American Thyroid Association; DFS, disease-free survival; DTC, differentiated thyroid carcinoma.
Cox's proportional hazards model
On univariate analysis, we evaluated age at diagnosis as a continuous variable, age at diagnosis above or below 55 years, and ATA risk classification. The ATA risk classification was the strongest predictor of relapse (Table 3). On multivariate analysis, the model including an age cutoff of 55 years and the ATA system was significant, and both variables were significantly associated with relapse (Table 3).
Univariate and Multivariate Analysis
HR, hazard ratio.
Adding age at diagnosis to the ATA risk stratification system
Following all the above results, we sought to build a prognostic model including the ATA stratification system with age >55 years old as a new prognostic factor. In this model, we defined four subgroups of risk patients: low-risk, intermediate-risk, and high-risk younger than 55 years, and high-risk older than 55 years. As shown in Figure 3, there was a significant difference for the four Kaplan–Meier curves (log-rank trend test, p < 0.0001). In particular, there was a significant difference between high-risk >55 years cohort and high-risk <55 years (p = 0.043), intermediate-risk (<0.0001), and low-risk (<0.0001) groups, and between intermediate-risk and low-risk groups (p < 0.0001).

Kaplan–Meier curves of DFS in DTC patients according to their ATA risk category; the high-risk group is divided into two groups of age at diagnosis: below or above 55 years.
Discussion
The present study was conceived to evaluate whether age at diagnosis may be a risk factor for DTC relapse after primary treatment. It is well recognized that old age is associated with poor prognosis in these patients, and the most recent version of the TNM system has changed the age cutoff of risk from 45 to 55 years (2). This decision was mainly supported by findings from a large retrospective study from 10 American institutions (3). In addition, other relevant earlier studies on this topic should be mentioned (4). To date, some studies have attempted to validate the eighth edition of the TNM, and some of the findings have supported the change from the previous edition (5 –7), while others have proposed further improvements (8,9). One study specifically analyzed the effect of changing the age cutoff of risk from 45 to 55 years (10) and found that this new threshold was more accurate in staging DTCs. The outcome of all these studies was always disease-specific death, consistent with the aim of using TNM staging system. In 2015, the ATA guidelines proposed a system for stratifying the risk of relapse of DTCs. According to this system, DTCs are classified on the basis of their histology, molecular assessment when available, and preoperative clinical presentation of cancer. However, patient age at diagnosis is not included in the ATA risk classification.
The objective of the present study was to evaluate the role of age at diagnosis as a predictor of structural recurrence, either alone or when combined with the ATA risk stratification system. According to specific selection criteria, we included a large number of DTC patients who were followed at four different institutions after total thyroidectomy and RAI therapy. The main findings of the study were the following. First, age at DTC diagnosis was a significant risk factor of structural cancer relapse. This cutoff performed better than 45 years because an increase in the relapse rate was present only from age 60 years and older (Table 2). Specifically, patients older than 70 years at diagnosis had the highest rate of relapse. Because the ATA risk stratification system already includes several clinical, pathological, molecular, and imaging characteristics, this finding suggests that age at diagnosis should be considered an additional feature for stratifying the initial risk of patients. The patients in our study cohort with an age at diagnosis between 18 and 30 years showed a higher percentage of relapse than those with an age at diagnosis between 31 and 40 years. This finding could probably be influenced by the high rate of REC recorded in the subgroup with age at diagnosis between 18 and 25 years. Even though we did not include patients <18 years old, it is well recognized that young DTC patients have a high risk of recurrence (11). Second, when DTCs were classified as high risk according to the ATA system and subdivided by age older than or younger than 55 years at diagnosis, a significantly different risk of relapse over time was observed. Patients classified as ATA high risk who were older than 55 years constituted a category at very high risk, while younger high-risk patients had a similar outcome to those of any age in the intermediate-risk group. In contrast, in the ATA low- and intermediate-risk classes, only a trend toward significance was observed between age at diagnosis and DFS. Third, in our multivariate logistic model, both ATA risk assessment and the 55-year age cutoff proved to be reliable and independent risk factors for identifying DTCs with the highest likelihood of structural relapse. This analysis identifies a subgroup of DTC patients at highest risk of relapse in whom adequate staging based on multimodality imaging (12) and molecular assessment (13) has to be considered due to the high likelihood of these patients needing adjuvant RAI (14). Since TNM staging stratifies the risk of disease-specific death, this cluster of patients has to be considered at high risk of death from DTC. These data may also guide the careful management and follow-up of the elderly patients, who are often frail and have comorbidities and are not amenable to an aggressive therapeutic approach after the initial treatment (i.e., surgery and RAI) (1,15). The present results corroborate and extend the findings reported by Shah and Boucai (16) who evaluated the effect of age at diagnosis on response to therapy and mortality in high-risk DTC.
Our study has several limitations and strengths. This was a retrospective study. Specific selection criteria were used to obtain a multicenter series of surviving DTC patients in whom complete follow-up data were available. Only adult patients treated with thyroidectomy and RAI were included. Importantly, these patients were treated and followed up at four different institutions, and the study results may be applicable only to patients having such treatment.
In conclusion, the age cutoff adopted in the eighth edition of thyroid TNM staging system for DTC patients at risk of death (i.e., 55 years) is also alone able to identify patients at higher risk of structural relapse. Applying this age cutoff to the ATA risk stratification system significantly improves the selection of cases at highest risk of relapse.
Authors' Contributions
P.T., L.G., and A.P.: conceptualization. A.B., G.S., A.D.P., V.S., A.C., and G.F.: extraction and curation of data. P.T. and L.C.: analysis of data. P.T. and A.P.: original draft and writing. All authors have reviewed the article and agreed to their individual contributions before submission.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.