
Abstract
Background:
Studies have highlighted the adverse effects of long work hours on workers' health; however, the association of long work hours with thyroid function has not been studied. This study aimed at assessing long work hours as a risk factor for thyroid dysfunction.
Methods:
This cross-sectional study was based on data obtained from the Korea National Health and Nutrition Examination Survey conducted from 2013 to 2015. A total of 2160 adults who worked 36–83 hours per week were included. Thyroid function was defined based on the population thyroid-stimulating hormone reference ranges, after excluding individuals with positive results for thyroid peroxidase antibody. The association between work hours and thyroid function was confirmed via multinomial logistic regression.
Results:
Hypothyroidism was more prevalent among those with longer work hours (3.5% vs. 1.4% for 53–83 and 36–42 work hours per week, respectively). Individuals who worked longer hours had an increased odds for hypothyroidism (odds ratio 1.46, confidence interval 1.12 − 1.90, per 10-hour increase in work hours per week), after adjustment for age, sex, body mass index, urine iodine concentration, smoking status, work schedule, and socioeconomic status. The association between work hours and hypothyroidism was consistent in various subgroups stratified by sex or socioeconomic status.
Conclusions:
To our knowledge, this study is the first to show that long work hours are associated with hypothyroidism. Further large longitudinal studies are needed to clarify causality.
Introduction
Long work hours are prevalent problems that threaten the health and safety of workers. The International Labor Office reported that more than one-fifth of workers worldwide work more than 48 hours per week (1). The adverse health impact of long work hours has been well established for cardiovascular diseases (2). In addition, there is increasing epidemiologic evidence that long work hours are also associated with adverse metabolic and mental health outcomes such as diabetes mellitus, obesity, metabolic syndrome, fatigue, and depression symptoms (3 –7).
Hypothyroidism is a common disease globally, with a reported prevalence of 3.83% in South Korea (8,9). Hypothyroidism is associated with many other diseases, including atherosclerotic cardiovascular disease, congestive heart failure, diabetes mellitus, obesity, metabolic syndrome, fatigue, and depression, which have large overlaps with overwork-related health outcomes (10 –18). Further, a recent study showed that shift work, another occupational environmental factor that adversely affects health (19), increased the risk of hypothyroidism (20). These pieces of evidence suggest that long work hours may be associated with hypothyroidism. However, there have been no reports on the relationship between work hours and thyroid function to date.
In this study, we aimed at assessing the association between work hours and thyroid function by using up-to-date nationally representative data in South Korea.
Materials and Methods
Study subjects
This study was based on data acquired from the sixth Korea National Health and Nutrition Examination Survey (KNHANES VI), which was conducted from 2013 to 2015. KNHANES is a nationwide, cross-sectional survey of the Korean population performed by the Korea Centers for Disease Control and Prevention, which assesses the overall health, as well as nutritional and socioeconomic status, of the non-institutionalized civilian population in South Korea (21). Participants of the KNHANES were selected by using a stratified multistage clustered probability sampling design, which has been validated as appropriate for representative statistics by the Korea Department of Statistics.
The institutional review board of the Korea Centers for Disease Control and Prevention approved the protocol of the KNHANES (IRB approval number: 2013-07CON-03-4C, 2013-12EXP-03-5C, and 2015–01-02-6C), and written informed consent was obtained from all participants.
From 2013 to 2015, a total of 6564 individuals aged 10 years or older presented for measurement of thyrotropin (TSH), free thyroxine (fT4), thyroid peroxidase antibody (TPOAb), and urinary iodine levels in spot urine samples. Among those participants, 3434 adult workers (individuals aged ≥19 years who responded that they were currently working) were screened in this study (Fig. 1).

Flow chart of study population selection and inclusion and exclusion criteria. fT4, free thyroxine; KNHANES, Korea National Health and Nutrition Examination Survey; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin.
The following subjects were excluded: (i) part-time workers (work hours <36 per week, based on the definition of the Korea Labor Institute) (22) (n = 966); (ii) pregnant women (n = 6); (iii) those with a history of thyroid disease (n = 84) or positive TPOAb results (TPOAb level ≥34.0 IU/mL; n = 126; these individuals were excluded to minimize the potential confounding from musculoskeletal symptoms and fatigue of those with autoimmune thyroid disease) (23 –26); (iv) those with missing parameters on body mass index (BMI), smoking status, occupation, work schedule (those who did not disclose their work schedule and those whose work schedule could not be categorized due to ≥12 work hours per day), educational attainment, or income levels (n = 85); and (v) isolated hypothyroidism (fT4 levels <0.82 ng/mL in combination with TSH levels of 0.62 − 6.68 mIU/L; n = 4) and isolated hyperthyroidism (fT4 levels >1.76 ng/mL in combination with TSH levels of 0.62 − 6.68 mIU/L; n = 3).
A total of 2160 subjects were finally included in the present analyses, a representative sample of 13,033,409 Koreans.
Laboratory assay
Serum TSH, fT4, and TPOAb levels were measured by an electrochemiluminescence immunoassay. TSH level was measured by using an E-TSH kit (Cobas e 411 analyzer; Roche Diagnostics, Mannheim, Germany), and its reference range was considered as 0.62–6.86 mIU/L based on KNHANES VI data (8). The fT4 level was measured by using an E-Free T4 kit (Cobas e 801; Roche Diagnostics), and the reference range was 0.89–1.76 ng/mL. The TPOAb level was measured by using an E-Anti-TPO kit (Cobas e 801; Roche Diagnostics) with a reference range of 0–34 IU/mL. Urine iodine concentrations were measured by using an inductively coupled plasma mass spectrometry device (Perkin Elmer ICP-MS, Waltham, MA), using an iodine standard (Inorganic Venture, Christiansburg, VA).
Anthropometric, behavioral, psychological, occupational, and socioeconomic variables
Participants' heights and weights were measured via direct standardized physical examinations performed at specially equipped mobile examination centers. BMI was calculated by dividing the weight by the square of height (kg/m2). Smoking status was categorized as “current smoker” or “nonsmoker.” The degree of perceived stress was categorized as low or high according to each subject's answer to the relevant multiple choice question. Feeling “only a little” stress or stress “to some extent” was classified as “low,” and feeling stress “to a great extent” or “to a very great extent” was classified as “high.”
The number of work hours per week for each subject was assessed based on the responses to the relevant open questions in the questionnaire. Work schedule was categorized as “daytime workers” or “shift workers” (19). Those who mainly worked between 6 a.m. and 6 p.m. were classified as daytime workers. Those who mainly worked in the afternoon (between 2 p.m. and midnight), at night (between 9 p.m. and 8 a.m. the next day), in segmented shifts (working more than two shifts a day), or in rotation of shifts were classified as shift workers.
Occupations were grouped based on the occupation classification code: Managers, professionals, and clerks were classified as office workers; service and sales workers were classified as service workers; and skilled agricultural, forestry and fishery workers, craft and related trades workers, plant and machine operators, assemblers, and elementary manual workers were classified as manual workers. Individual income levels were categorized into four groups according to income quartile (low, middle-low, middle-high, and high). Educational attainment was classified into four groups: elementary school or lower, middle school, high school, and college or higher.
Definition of thyroid function
Hypothyroidism was defined as a serum TSH level above the upper reference limit with a normal fT4 level (subclinical hypothyroidism) or a low fT4 level (overt hypothyroidism). Hyperthyroidism was defined as a serum TSH level below the lower reference limit with a normal fT4 level (subclinical hyperthyroidism) or a high fT4 level (overt hyperthyroidism). Euthyroidism was defined as a serum TSH level within the reference range with a concomitantly normal fT4 level.
Statistical analysis
Survey sample weights were used in the analysis to account for the complex sampling design and to represent the distribution of the national population. Continuous variables are presented as medians with interquartile ranges (IQRs) or means with their standard errors. Categorical variables are summarized as frequencies and percentages. Comparisons of the prevalence of thyroid dysfunction according to the tertiles of weekly work hours were performed by using the chi-square test. The mean weekly numbers of work hours according to thyroid function were compared via analysis of variance and post hoc analysis with the Bonferroni correction.
Associations of weekly number of work hours (continuous) with hypothyroidism and hyperthyroidism were assessed by using the multinomial logistic regression model. Multinomial multivariable logistic regression was performed to control for potential confounding factors, such as age, sex, BMI, urine iodine level (log-transformed), smoking status, work schedule, occupation, income level, and education level. The associations are presented as odds ratios (ORs) with confidence intervals (CIs). To explore whether long work hours were associated with clinically significant levels of thyroid dysfunction, we also assessed the associations of the number of weekly work hours with TSH levels ≥7.0 mIU/L and TSH levels <0.1 mIU/L, as active interventions are generally considered when these levels of TSH abnormalities are persistent (27,28).
Logistic regression was further performed with stratification according to the following subgroups: sex (male or female), occupation (office workers or service/manual workers), income levels (low to middle-low or middle-high to high), and educational attainment (below college, or college or higher). In addition, multinomial multivariable logistic regression was performed with further exclusion of those with <40 work hours per week (below the standard work hours in Korea) or >68 hours (above the legal limits of work hours in Korea), since those with unusual (very short or very long) work hours might be under unique work environments that were not simply adjustable by a multivariable model. Similarly, logistic regression was performed with exclusion of those with overt thyroid dysfunction, to confirm the association between work hours and thyroid dysfunction after minimizing the effects of extreme values.
To address the possibility of a selection bias driven from excluding of those who work ≥12 hours per day, we also performed multinomial logistic regression with extended data, including those of such individuals. In this analysis, work schedule was not used for adjustment.
All statistical analyses were performed by using SAS 9.4 (SAS Institute, Inc., Cary, NC). Analysis of comparisons with p < 0.05 were considered statistically significant.
Results
Baseline characteristics of study participants
The characteristics of the 2160 study participants are shown in Table 1. The median age of the subjects was 42.4 (IQR 33.0–52.1) years, and 1468 (69.9%) participants were males. The median urine iodine concentration was 291.6 (IQR 158.6–630.9) μg/L, the median BMI value was 23.7 (IQR 21.7–26.0) kg/m2, and 694 (32.5%) participants were current smokers. High perceived stress was reported by 620 (28.8%) participants. The median weekly number of work hours was 47.1 (IQR 39.8–54.9), and 15.4% of participants were shift workers. The proportions of office workers, service workers, and manual workers were 43.4%, 18.7%, and 37.8%, respectively, and 46.4% of participants were college graduates.
Baseline Characteristics of Study Participants
BMI, body mass index.
Prevalence of thyroid dysfunction according to the number of work hours per week
Overall, 2059 (94.9%) participants were euthyroid; hypothyroidism and hyperthyroidism were observed in 45 (2.1%) and 56 (2.9%) participants, respectively (Table 1). We evaluated the prevalence of hypothyroidism and hyperthyroidism according to the number of work hours per week, grouped as tertiles (Table 2; 36–42, 43–52, and 53–83 hours per week). The prevalence of euthyroidism decreased with longer work hours (96.7%, 95.3%, and 92.9% in the first, second, and third tertiles, respectively), whereas that of both hypothyroidism and hyperthyroidism was the highest in the group with the highest work hours (3.6% and 3.5%, respectively; chi-square p = 0.030).
Prevalence of Hypothyroidism and Hyperthyroidism According to Work Hours per Week
The relative proportions of individuals with euthyroidism, hypothyroidism, and hyperthyroidism according to the work hour groups were compared by using the Rao-Scott chi-square test.
Association between long work hours and hypothyroidism
The mean numbers of work hours per week among euthyroid, hypothyroid, and hyperthyroid individuals were 49.5 ± 0.3, 53.4 ± 1.5, and 51.6 ± 1.6 hours, respectively (p = 0.012) (Fig. 2). The post hoc analysis with Bonferroni correction showed that hypothyroid individuals had significantly longer work hours than did euthyroid individuals (p = 0.032). Similarly, work hours >48 hours per week was the most prevalent among individuals with hypothyroidism (Supplementary Table S1; 43.2%, 64.8%, and 52.4% among individuals with euthyroidism, hypothyroidism, and hyperthyroidism, respectively; chi-square p = 0.024).
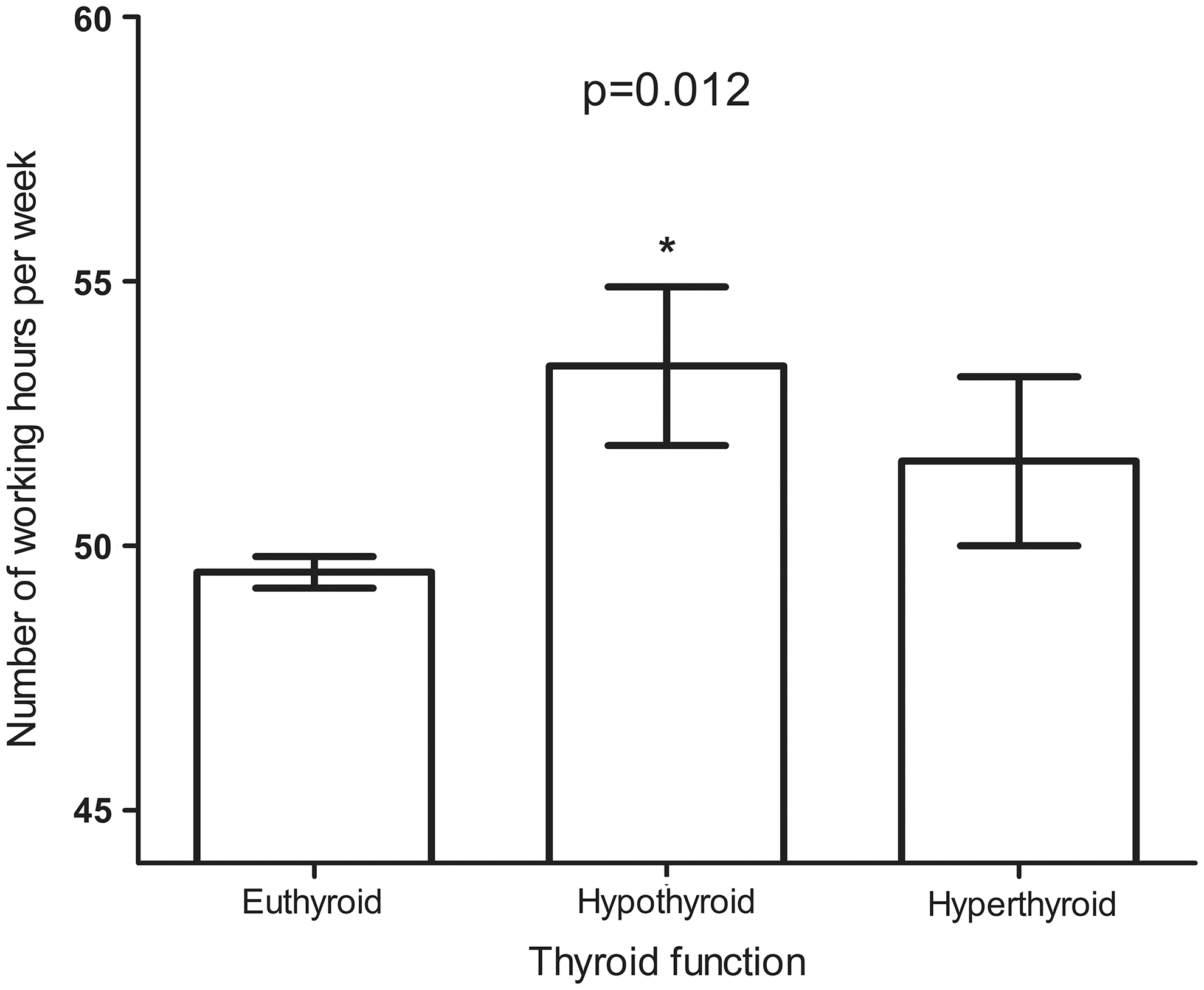
Work hours per week according to thyroid function (presented as means with standard errors), with intergroup comparisons by analysis of variance and post hoc tests. *p < 0.05 vs. euthyroid group.
In the multinomial logistic regression, we observed significantly high OR for the association between hypothyroidism and longer work hours per week (OR 1.38, CI 1.11 − 1.73 per 10-hour increase in work hours per week) (Table 3). The association was also significant after adjusting for age, sex, BMI, log-transformed urine iodine concentration, and cigarette smoking status (OR 1.51, CI 1.20 − 1.89), and after further adjusting for work schedule, occupation, income level, and educational attainment (OR 1.46, CI 1.12 − 1.90).
Association Between the Number of Work Hours per Week and Thyroid Dysfunction
ORs for hypothyroidism and hyperthyroidism, compared with euthyroidism, per 10-hour increase in the number of working hours per week. Model 1 was unadjusted. Model 2 was adjusted for age, sex, BMI, log-transformed urine iodine concentration, and smoking status. Model 3 was further adjusted for work schedule, occupation, income level, and educational attainment.
CI, confidence interval; OR, odds ratio.
In addition, the association was more evident after excluding outliers in the number of work hours per week (adjusted OR 1.99, CI 1.19 − 3.31 among those who worked for 40 − 68 hours per week [n = 1861]), and also significant after excluding participants with overt thyroid dysfunction (adjusted OR 1.44, CI 1.11 − 1.88 among those with normal fT4 level [n = 2155]). On the other hand, the odds for hyperthyroidism were not significantly associated with the number of work hours per week.
We also observed significantly high ORs for the association between TSH levels ≥7.0 mIU/L and long work hours per week (OR 1.42, CI 1.08 − 1.86 per 10-hour increase in work hours per week) after adjusting for age, sex, BMI, log-transformed urine iodine concentration, cigarette smoking status, and occupational and socioeconomic variables (Supplementary Table S2).
The association between hypothyroidism and weekly work hours was also consistent in the extended data (n = 2221), including the data of those working ≥12 hours per day (Supplementary Table S3). Those with long work hours had a high OR for hypothyroidism (OR 1.27, CI 1.04 − 1.53 per 10-hour increase in working hours per week) after adjusting for age, sex, BMI, log-transformed urine iodine concentration, cigarette smoking status, occupation, income level, and educational attainment.
Subgroup analyses
The associations between long work hours per week and hypothyroidism in the subgroups, represented by ORs and their CIs, were compared by using a forest plot (Fig. 3). We observed consistently high ORs for the association between hypothyroidism and long work hours per week in the subgroups stratified by sex or socioeconomic characteristics such as occupation, income level, and educational attainment.

Association between work hours per week and hypothyroidism in the subgroup analysis. Multinomial multivariable logistic regression was adjusted for age, sex, body mass index, log-transformed urine iodine concentration, and smoking status. 1Odds ratios for hypothyroidism per 10-hour increase in working hours per week are presented with confidence intervals.
Discussion
In this study, we showed that long work hours were associated with hypothyroidism in workers with no evidence of thyroid autoimmunity, using well-characterized population representative data. Individuals with longer work hours (53–83 hours per week, 3.6%) had about 2.6 times higher prevalence of hypothyroidism than did those with shorter work hours (36–42 hours per week, 1.4%), and a 10-hour increase in the number of work hours per week increased the OR for hypothyroidism by 1.46 times. In addition, the association between work hours and hypothyroidism was consistent in various subgroups stratified by sex or socioeconomic status.
Many epidemiological studies have investigated the deleterious effects of overwork on workers' health, and currently, long work hours are regarded as an important environmental risk factor. In two large meta-analyses performed by Kivimäki et al., long work hours (≥55 hours per week) increased the risk of incident coronary heart disease and stroke compared with standard work hours (35–40 hours per week) and also increased the risk of type 2 diabetes in individuals with low socioeconomic status (2,3). In addition, other systematic reviews affirmed that long work hours were associated with metabolic syndrome, fatigue, and depressive symptoms (5,6).
However, laboratory assays were limited in many previous epidemiologic studies, which was why the relationship between work hours and thyroid function could not be adequately assessed. Therefore, to our best knowledge, this study is the first article showing that long work hours are associated with a higher risk of hypothyroidism.
Although the potential mechanisms underlying the association between long work hours and hypothyroidism have not been studied in-depth so far, multifactorial causes may be at play. Long work hours contribute to psychological stress (6), and rat models have shown that social, as well as physical chronic stress, reduced thyroid hormone levels (29,30). Overwork-related unhealthy metabolic conditions and physical inactivity (6) may be another cause of hypothyroidism. Subclinical hypothyroidism is prevalent among patients with obesity, although the causal relationship is controversial (14). Hypothyroidism occurs more frequently in cohorts with metabolic syndrome than in those without (16). Further, physical inactivity is associated with higher TSH levels and a higher probability of subclinical hypothyroidism (31,32). Further studies are warranted to determine the mechanisms underlying the association more clearly.
In some studies, the impact of long work hours on health was more pronounced in individuals with low socioeconomic status (2,3). In addition, sex differences were sometimes observed in studies regarding thyroid function (8,33,34). In this study, we showed that the association between work hours and hypothyroidism was consistent in all subgroups classified by occupation, income level, educational attainment, and sex.
Our results need to be considered in view of the study limitations. First, since this was a cross-sectional observational study, the associations observed in this study cannot serve as proof of a causal relationship. However, considering that healthy workers are more likely to remain in a more vigorous workplace (35), the explanation that long work hours cause hypothyroidism seems more plausible than the converse. Second, most of the hypothyroidism cases in this study involved subclinical hypothyroidism. However, we also found that longer working hours were associated with a higher probability of TSH levels ≥7.0 mIU/L, and clinical interventions are generally considered when these elevated levels of TSH are persistent (27). Third, since those with positive TPOAb results were excluded to avoid potential confounding, the effect of work hours on thyroid autoimmunity could not be investigated. Fourth, since work hours were measured based on a single assessment, our results may not represent prolonged exposure to overwork. Similarly, as measurements of TSH and fT4 levels were performed only once for each individual without records of blood collection time, intra-individual variation could not be considered. Further longitudinal studies, with repeat measurements of work hours and laboratory tests, are needed to further clarify the causal relationship and long-term effects, including the persistence of hypothyroidism, and to address intra-individual variations.
If the association between long work hours and hypothyroidism that we observed is confirmed to be a causal relationship in future longitudinal studies, it would have great implications for the public health. First, it could be the basis for recommending reduction in work hours to improve thyroid function among overworked workers with hypothyroidism. Second, hypothyroidism is a well-established predisposing factor for atherosclerotic cardiovascular disease and is also associated with the onset of stroke, congestive heart failure, diabetes mellitus, and diabetic complications (10 –13,36). Therefore, screening and treating hypothyroidism may contribute to the prevention and proper management of cardiovascular disease and diabetes mellitus associated with long work hours (2,3). Third, screening for hypothyroidism can be performed by using simple laboratory tests (37) and may thus be easily integrated into workers' health screening programs. Ultimately, the data from prospective studies on the efficacy of interventions, including shortening work hours and levothyroxine replacement therapy, would be needed to determine the best strategies for treating hypothyroidism associated with long work hours.
In conclusion, our study is the first to show that long working hours are associated with hypothyroidism, using large nationwide representative data and population-based TSH reference ranges. The results of our study suggest that it may be helpful to consider the possibility of hypothyroidism while assessing the health of individuals working long hours. Further research is needed to clarify the causal relationship and the underlying mechanism.
Footnotes
Author Disclosure Statement
No competing financial interests exist. The funding sources had no involvement with the study design, data collection, analysis, interpretation of data, or the decision to submit the article for publication.
Funding Information
This work was supported by grants from the National Cancer Center, Korea (Grant No. 1810153).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3