
Abstract
Background:
Literature to date has been inconclusive regarding the value of thyroglobulin (Tg) as a marker of iodine status in pregnant women. This systematic review and meta-analysis is one of the first to assess whether Tg concentration accurately reflects iodine status among pregnant women.
Methods:
We searched MEDLINE, the Web of Science, the Cochrane Library, Scopus, and other relevant databases to identify relevant studies published in the English language, between January 1988 and December 2018. The criteria for study inclusion in the systematic review were human studies, healthy pregnant women as participants, and available data for maternal urinary iodine concentration (UIC) and Tg level. Each study was assessed for quality and risk of bias. The pooled mean Tg values, and 95% confidence intervals were estimated in a population of women with UIC <150 and UIC ≥150 μg/L during pregnancy. Potential linear or nonlinear dose
Results:
Of 814 identified studies, 25 were eligible for inclusion in the meta-analysis. Studies included were conducted in Africa, Asia, Europe, South America, and the Oceania. The pooled mean (95% confidence interval [CI]) Tg concentration in iodine-deficient pregnant women was higher than that in iodine-sufficient pregnant women (10.73 μg/L [5.65–15.82] vs. 7.34 μg/L [2.20–12.47]); a comparison of the 95% CI showed that none of these values was significantly different. No significant differences were observed in Tg concentration between the two groups in each trimester of pregnancy. Dose
Conclusions:
Our meta-analysis showed that Tg concentration can be a sensitive indicator of iodine deficiency, specifically in populations of pregnant women with median UIC <100 μg/L. Further studies are warranted to determine the sensitivity of Tg at different degrees of iodine deficiency during pregnancy.
Introduction
Iodine, a trace element, is a vital component of thyroid hormones (thyroxine [T4] and triiodothyronine [T3]) that have fundamental roles in proper growth and central nervous system development in fetuses and infants (1,2). Iodine requirements increase substantially during pregnancy, to ∼150% of those of nonpregnant women, due to increased thyroid hormone production, iodine transfer to the fetus, and increased urinary iodine excretion (3,4). The consequences of iodine deficiency during this critical period depend on the timing and severity of the deficiency and can include cretinism, neonatal hypothyroidism, growth retardation, neurologic and cognitive deficits, increased risk of miscarriage, and infant mortality (5).
According to the criteria of the World Health Organization (WHO), the Iodine Global Network (IGN, formerly the International Council for the Control of Iodine Deficiency Disorders [ICCIDD]), and the United Nations Children's Fund (UNICEF), median urinary iodine concentration (UIC) is a well-accepted, cost-efficient, and easily measured indicator for determining iodine status at the population level (6). However, UIC is only considered to be a sensitive marker of recent iodine intake; it cannot be used to determine an individual's iodine status and thyroid function (7). Other recommended markers for iodine status include thyroid volume, a sensitive marker for severe iodine deficiency over a period of months or years (8), and thyroid hormones, such as thyroid stimulating hormone (TSH), T4, and T3, which are weak markers of iodine status because the levels remain within the normal reference range during mild-to-moderate iodine deficiency (9). Recent studies suggest that thyroglobulin (Tg), a thyroid-specific protein, may be a better indicator of iodine status, particularly in populations of school-aged children (10). In a former statement by the WHO/ICCIDD/UNICEF in 1994, a median Tg concentration <10 μg/L was recommended as the cut-off for iodine sufficiency in school-aged children and adults (11), and more recently, a study by Zimmermann et al. proposed a median Tg concentration of <13 μg/L as a biomarker of adequate iodine status in healthy populations of school-aged children (12).
However, there is some controversy regarding the value of Tg in assessing iodine status in populations of pregnant women. Current studies report inconsistent findings regarding the association between UIC and Tg during pregnancy. In some studies, little to no correlation was found between maternal UIC and Tg during pregnancy (13,14), while others reported variations in Tg concentration between severe iodine deficiency and more-than-adequate iodine status (15,16). A recent international study by Stinca et al. proposed a cutoff value of 10 μg/L for Tg, measured in a dried blood spot, as an index of iodine sufficiency among pregnant women (15). However, there is currently no scientific consensus for a Tg cutoff point to accurately identify iodine deficiency during pregnancy, and it is unclear whether the Tg cutoff of 13 μg/L, suggested as a marker of iodine status in school-aged children, is applicable to populations of pregnant women. Therefore, this study represents one of the first systematic reviews and meta-analyses to investigate the association between maternal UIC and Tg levels during pregnancy, and to determine whether Tg concentration accurately reflects iodine status among populations of pregnant women, using the median UIC as an index of iodine status.
Methods
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (17).
Search strategy
We conducted a systematic literature search of all articles published between January 1988 and December 2018, using electronic databases including MEDLINE/PubMed (National Library of Medicine), the Web of Science citation indexing service (produced by the Institute for Scientific Information), the Cochrane Library CENTRAL, and Scopus. In addition, searches were conducted by using internet search engines Google and Google Scholar. Key terms used in the searches were “iodine nutrition,” “urinary iodine,” “maternal iodine status,” “pregnancy,” “pregnant women,” “thyroglobulin,” “Tg,” “thyroid function parameters,” and “thyroid hormones.” To further identify relevant papers, we also performed a manual search by using the reference lists of original articles and relevant reviews. All resulting articles were downloaded into EndNote to merge retrieved citations, remove duplicates, and simplify the review process.
Study selection and data extraction
Two investigators performed independent searches. On completion, the titles and abstracts of the studies identified were visually scanned to exclude studies that were obviously irrelevant. The full text of remaining studies was retrieved, and all relevant articles were identified. The criteria for study inclusion in the systematic review were as follows: human studies, healthy pregnant women as participants, and available data for maternal UIC and Tg concentration. Exclusion criteria were as follows: animal studies, non-English articles, inclusion of pregnant women exposed to environmental factors that can influence iodine status and thyroid function (i.e., tobacco smoking, iodine supplements, and iodine overload, for example, iodine-containing contrast media, radioactive iodine, and povidone-iodine disinfection), inclusion of pregnant women with thyroid disorders, and any duplicate publications or incomplete articles. The PICO (Participant, Intervention, Comparator, and Outcome) criteria are shown in Table 1.
Participant, Intervention, Comparator, and Outcome Criteria for Inclusion of Studies
Data from the included studies were extracted independently by two investigators, using standardized forms developed for this review. Any discrepancies were resolved by consensus. The following data were extracted: first author, year of publication, country or location of study, number of pregnant women investigated, gestational age or trimester of pregnancy, and mean or median UIC and Tg concentrations with their correlation coefficients.
Quality assessment
We assessed the study quality by using the Newcastle-Ottawa Scale and scored each study on the basis of three different points of view, including the selection of the study samples, comparability of groups, and methods used to determine the outcome of interest. Each study received 0–2 asterisks for each criterion, and an overall quality score was calculated as the sum of individual asterisks. For descriptive purposes, we categorized the Newcastle-Ottawa scores of 2–3, 4–6, and 7–10 as studies of low, moderate, and high quality, respectively.
Data synthesis
According to international criteria, median UIC values <150 and ≥150 μg/L in the population of pregnant women are considered to represent iodine-deficient and -sufficient status, respectively (6). Women were assigned to iodine status groups based on overall study median UIC during pregnancy. If maternal UICs were reported at different trimesters of pregnancy in a single study, we pooled these as a single study for our analysis. To estimate a combined effect size across subgroups (i.e., different trimesters) within a study, the mean and variance of subgroups were computed; then, meta-analysis was conducted based on the summary effect and variance was computed. In studies in which Tg concentrations were reported among groups of pregnant women with UIC <150 and ≥150 μg/L, we included each group as a separate study.
Statistical analysis
We calculated the mean values and standard deviations (SDs) of Tg based on the median, lower, and upper interquartile range (IQR), range, or 95% confidence interval (CI) if the mean and SD were not directly reported. The mean Tg values and 95% CI were estimated based on maternal UIC (< 150 μg/L vs. ≥150 μg/L) during pregnancy. To indicate whether Tg concentration can be influenced by human chorionic gonadotropin (hCG) in the first trimester compared with the two other trimesters, studies were divided into three trimesters and then a sub-analysis was done to estimate mean and 95% CI of Tg concentration in iodine-deficient and -sufficient populations of pregnant women in each trimester. For the analysis, we used a fixed-effect model based on the absence of heterogeneity. We evaluated statistical heterogeneity according to Q Cochrane and the I 2 index. In the fixed-effect analysis, each study was weighted by the inverse of its variance.
For the dose
Results
Figure 1 shows the literature search and study selection process. Among 418 studies identified in our initial search, 129 appeared potentially relevant and were thus assessed as full-text papers for inclusion. After exclusion of potential studies that failed to meet the eligibility criteria described earlier, 27 studies were found to be eligible for inclusion in this systematic review. The main reason for the exclusion of most studies was that they did not report any data for either maternal UIC or Tg concentration during pregnancy. After excluding studies reporting duplicate data, 25 studies were eligible for inclusion in the meta-analysis. The general characteristics of the included studies are presented in Table 2. Studies included were conducted in Africa (Democratic Republic of the Congo, Morocco, Niger, South Africa, Sudan, and Tanzania), Asia (China, India, Iran, Nepal, Philippines, Sri Lanka, Thailand, and Turkey), Europe (Belgium, Croatia, Denmark, France, Greece, Hungary, Iceland, Poland, Portugal, Spain, Sweden, Switzerland, and the United Kingdom), South America (Brazil), and Oceania (New Zealand). Based on the data from the studies included in this systematic review, the median/mean UIC of pregnant women residing in China, Hungary, India, Nepal, South Africa, Spain, and Tanzania was ≥150 μg/L; whereas in other countries such as Belgium, Brazil, Croatia, Denmark, Democratic Republic of the Congo, France, Greece, Iceland, Iran, Morocco, New Zealand, Niger, Philippines, Poland, Portugal, Sri Lanka, Sudan, Sweden, Switzerland, Thailand, Turkey, and the United Kingdom, pregnant women had a median/mean UIC <150 μg/L. The quality scores of studies included in the meta-analysis ranged from 6 to 9. The majority of studies received high-quality scores; 3 were scored as moderate (Table 3).
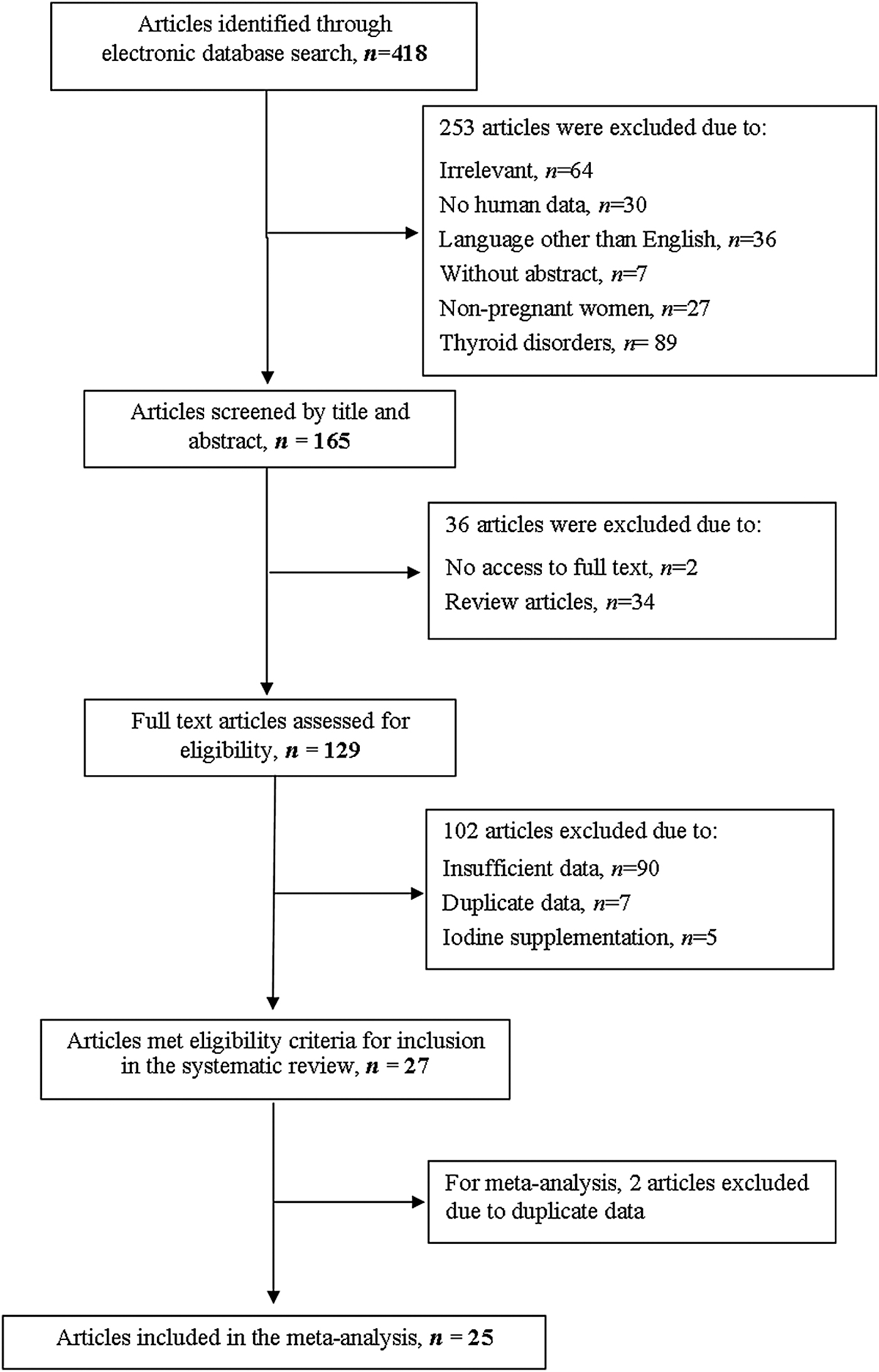
Flow chart of studies selection for the present systematic review and meta-analysis.
Urinary Iodine and Thyroglobulin Concentrations in Pregnant Women
Values are means ± SDs, geometric means (95% CIs), medians, medians [IQRs], or medians {ranges}.
Values are given in μg/Cr.
Correlation coefficient reported at the population level.
ECLIA, electrochemiluminescence immunoassay; ELISA, enzyme-linked immunosorbent assay; ICMA, immunochemiluminescence assay; ILMA, immunoluminometric assay; IRMA, immunoradiometric assay; NS, not stated; RIA, radioimmunoassay; Tg, thyroglobulin; T; trimester; UIC, urinary iodine concentration; wk, week.
Quality Assessment of All Studies Included in the Meta-Analysis
Newcastle- Ottawa scores 2–3, 4–6, and 7–10 were considered as having low, moderate, and high qualities, respectively. The asterisks denote the score(s) for each criterion. One asterisk denotes a score of 1, and 2 asterisks denote a score of 2.
The forest plot with mean and 95% CI and the pooled estimates for the mean Tg concentration in pregnant women with iodine deficiency or sufficiency are presented in Figure 2. The median/mean maternal UIC concentration in the iodine-deficient group ranged between 25 and 149 μg/L, while in the iodine-sufficient group, this value ranged between 155 and 625 μg/L. No substantial heterogeneity was identified between the study-specific estimates (I2 = 0.0%, p-heterogeneity = 1.0 and I2 = 0.0%, p-heterogeneity = 0.968, respectively). There was a publication bias between the two subgroups (p < 0.05). The mean Tg concentrations of women with iodine deficiency were higher than those of women with iodine sufficiency during pregnancy (10.73 μg/L [95% CI 5.65–15.82] vs. 7.34 μg/L [95% CI 2.20–12.47]); however, when comparing the 95% CI, no significant difference was observed between the two groups. A summary of pooled estimates of Tg concentration by trimester of pregnancy is given in Table 4. In the trimester-specific analysis, the mean Tg concentrations of pregnant women with iodine deficiency versus sufficiency were 11.47 μg/L [95% CI 6.67–16.27] vs. 11.09 μg/L [95% CI 6.19–15.99] in the first trimester, 8.55 μg/L [95% CI 4.62–12.47] vs. 10.88 μg/L [95% CI 5.09–16.66] in the second trimester, and 11.59 μg/L [95% CI 7.31–15.88] vs. 8.86 μg/L [95% CI 4.43–13.29] in the third trimester of pregnancy. Comparison of the 95% CI showed no significant differences in the pooled mean Tg concentration between populations of pregnant women with iodine deficiency and sufficiency in each trimester.

Mean and 95% confidence interval and the pooled estimates for mean of thyroglobulin concentration in populations of pregnant women with iodine deficiency versus sufficiency Subgroup analysis was based on maternal iodine status. Open diamonds represent the pooled estimates for each subgroup and the overall estimate for thyroglobulin concentration. The solid diamonds represent the point estimate of each study (horizontal lines represent 95% CIs), and the size of squares is proportional to the percentage weight of each study. The I 2 values refer to the statistical heterogeneity within each subgroup and combined studies. CI, confidence interval.
Summary of Pooled Estimates of Thyroglobulin Concentration by Trimester of Pregnancy
Pooled means (95% CIs)
Eight studies reported no correlation between maternal UIC and Tg concentration during pregnancy, and five studies reported negative significant correlations between these two parameters (Table 2). Figures 3 and 4 show linear and nonlinear dose
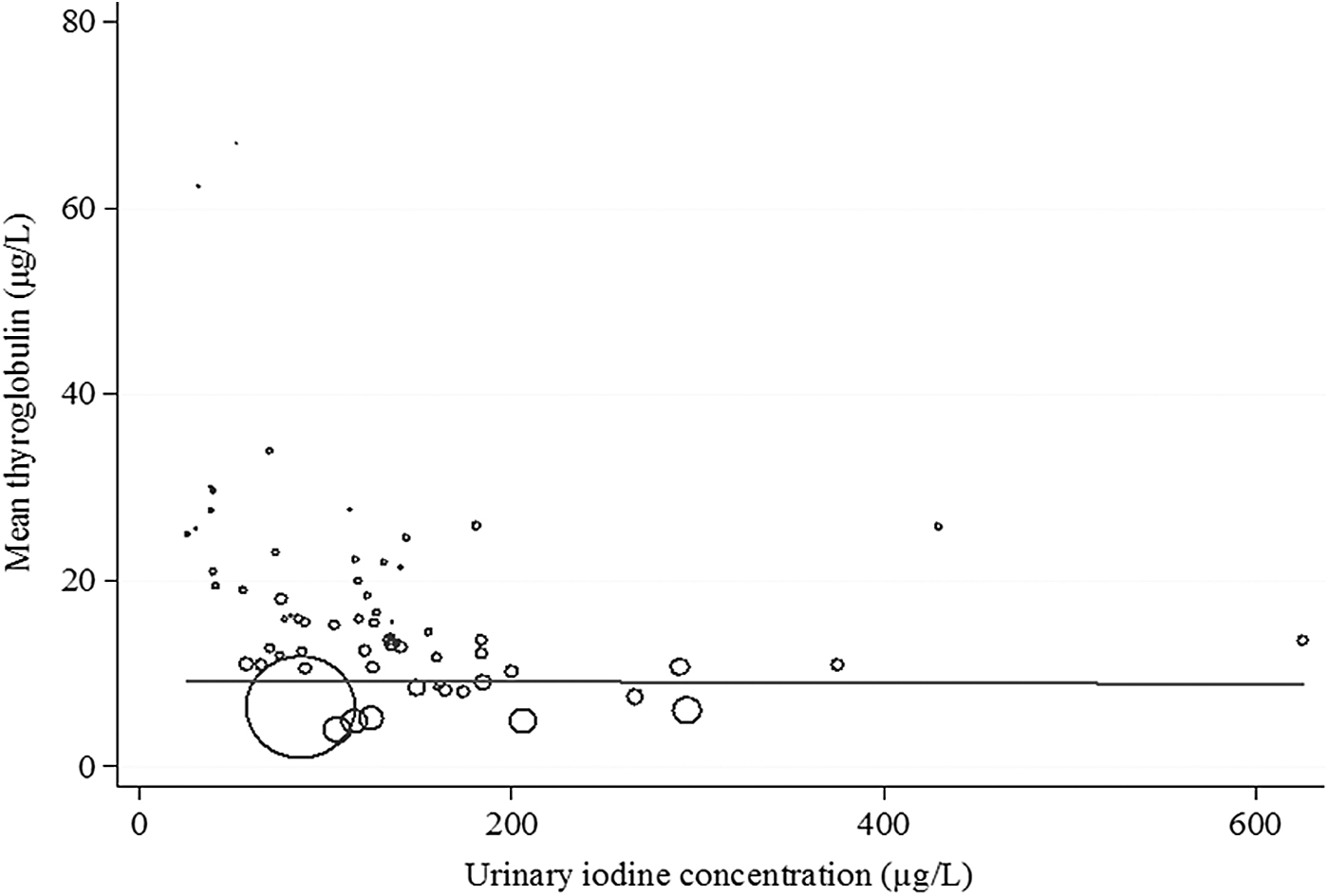
Linear dose
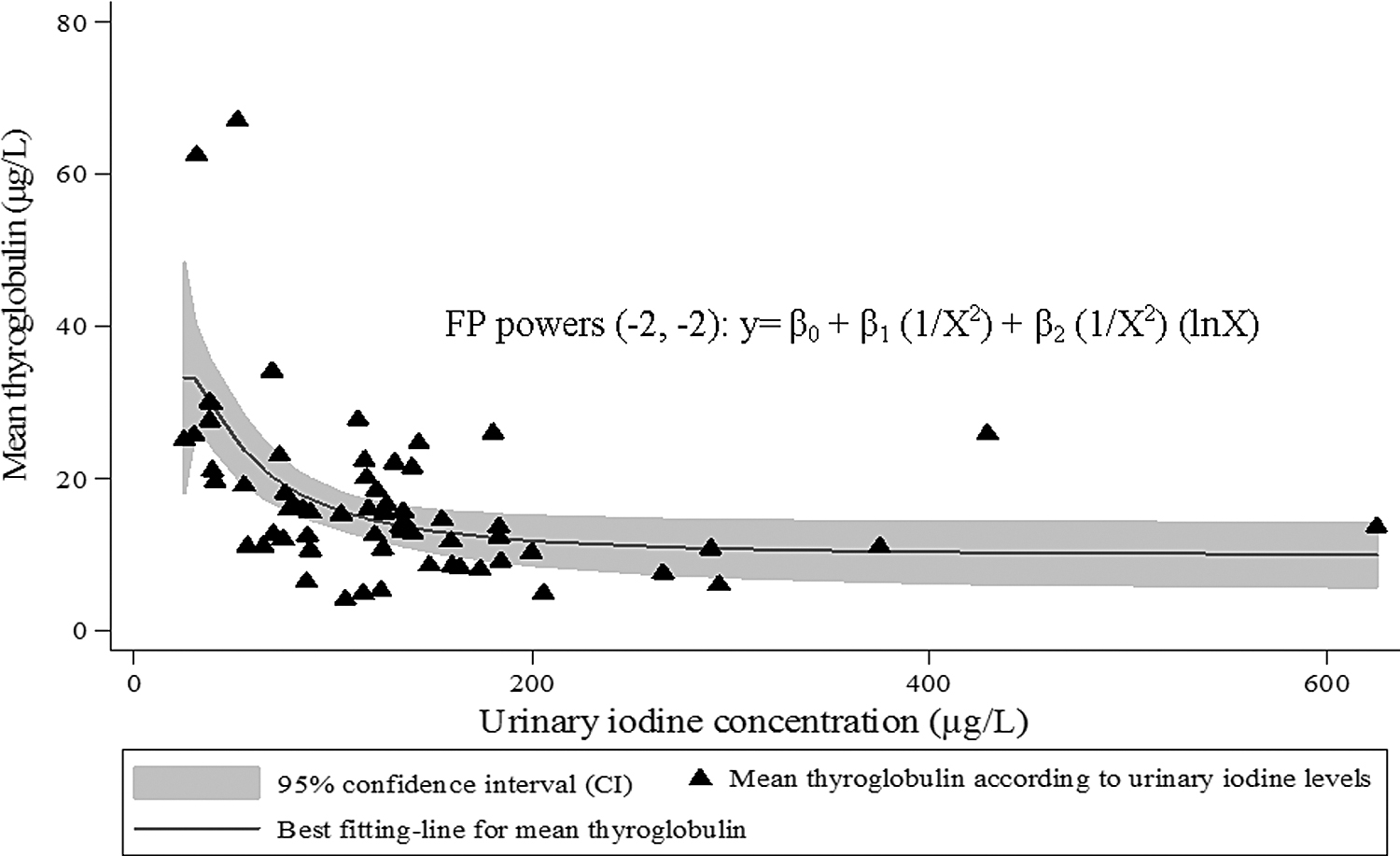
Nonlinear dose

Associations between thyroglobulin concentration and maternal urinary iodine levels of <100 μg/L (
Discussion
This meta-analysis indicates that populations of pregnant women with iodine deficiency in the included studies had a higher Tg concentration compared with those with iodine sufficiency, although the difference was not statistically significant. No differences were found in Tg concentration between iodine-deficient and -sufficient groups by trimester of pregnancy. When we grouped populations of pregnant women by their median UIC (<100, 100–150, and >150 μg/L), an inverse association of Tg was observed with UIC among populations with moderate iodine deficiency (median UIC <100 μg/L); however, there was no association between Tg concentrations and UIC in populations of pregnant women where median UIC was >100 μg/L.
Available data show that Tg concentration may be elevated in both deficiency and excessive iodine status during pregnancy (18); however, no definitive correlation between Tg concentration and UIC has been reported. Although a few studies have been conducted in populations of pregnant women with adequate or excess iodine intake (15), studies in iodine-deficient populations of pregnant women indicate that a decrease in maternal UIC is not always accompanied by an alteration in Tg concentration (9,13,14,19 –21). The lack of correlation between these two indicators may be attributed to a single measurement of UIC, which could be confounded by hydration status, dietary intake, and diurnal variation (22). Significant variations in Tg assays among the studied populations of pregnant women may be a possible reason for inconsistent findings on correlation between Tg concentration and UIC. Studies have shown that the concentration of Tg is method dependent (10) and there can be a two-fold difference in Tg values reported for the same serum measured by different methods (23). Another possible explanation is that in addition to iodine status, Tg concentrations can be influenced by hCG and TSH levels during pregnancy, both of which stimulate Tg secretion (24,25). However, in our meta-analysis, there was no significant difference in Tg concentration across the three trimesters of pregnancy. Also, it is worth noting that the UIC only assesses recent iodine intake (i.e., days), whereas Tg is a better biomarker of iodine status that reflects intermediate change (i.e., weeks to months) in iodine intake (10,26). In some studies, iodine/creatinine ratio (UIC/Cr) was used to indicate iodine status during pregnancy, to minimize variation in UIC, and to improve the classification of iodine status; however, these population-based studies were also inconclusive regarding a relationship between UIC/Cr and Tg (16,27). Our meta-analysis showed that mean Tg concentration tended to be elevated in iodine deficiency, although there was no statistically significant difference in Tg concentration between populations of pregnant women with iodine sufficiency and -deficiency when they were categorized based on the median UIC of 150 μg/L.
The WHO recommendations (6) do not provide cutoff points to distinguish between severe, moderate, and mild iodine deficiency during pregnancy; however, recent studies suggest that the corresponding values of median UIC <50 μg/L, 50–100 μg/L, and 100–150 μg/L in populations of pregnant women can be considered representative of the severity of iodine deficiency (9,28). In our study, mean Tg concentration was significantly higher among populations of pregnant women with median UIC <100 μg/L than that in populations of pregnant women where median UIC was >100 μg/L. Within populations, in a large-scale population of pregnant women in an iodine-sufficient region of China, higher concentrations of Tg were observed among groups of women with UIC <100 μg/L and ≥500 μg/L, indicating a U-shaped curve for the relationship between Tg concentration and UIC (18). In a cohort of mildly to moderately iodine-deficient pregnant women in the United Kingdom, a UIC/Cr <100 μg/L observed across all trimesters was also inversely associated with serum Tg concentration (16). However, a study in France found that in a population of pregnant women with a median UIC of 81 μg/L, maternal UIC was not associated with the thyroid parameters of TSH, free T4, and Tg (21). A similar pattern was also observed in Iran, where the population of pregnant women had a median UIC of 87 μg/L, emphasizing that mild/moderate iodine deficiency is not always accompanied by alterations in commonly accepted indicators of thyroid status (9). Consistent with our results, a previous study conducted among 11 countries with varying iodine status reported no association between median maternal UIC and Tg concentration across populations of pregnant women with sufficient or more-than-adequate iodine intakes (15).
To date, no consensus has been reached regarding the optimal cutoff value for Tg concentration to indicate iodine status during pregnancy. For instance, in Belgium, a mildly iodine-deficient country, a median Tg of <20 μg/L suggested iodine sufficiency in a population of pregnant women (29); whereas a review by Ma et al. used a median Tg of <13 μg/L to indicate adequate iodine status among populations of pregnant women (10), taken from the cutoff value proposed by Zimmermann et al. to indicate iodine status in school-aged children (30). The authors concluded that although Tg ≥13 μg/L was an appropriate value to indicate iodine deficiency, this cutoff point should be used with caution due to lack of large observational studies in populations of pregnant women with adequate iodine status. In our meta-analysis, the mean Tg concentration in populations of pregnant women with iodine deficiency and sufficiency was 10.73 μg/L and 7.34 μg/L, respectively, with overlapping of confidence intervals. This finding was not entirely inconsistent with recent studies, which proposed a cutoff Tg concentration of 10 μg/L measured in serum or dried blood spot as an indicator of iodine sufficiency during pregnancy (15,18,31). However, our study design could not provide an adequate resolution for testing a specific cutoff.
To our knowledge, this study is the first meta-analysis conducted on Tg concentration and its association with iodine status (iodine deficiency vs. sufficiency) among populations of pregnant women. We used both linear and nonlinear dose
Considering that pregnant women and their fetuses are highly vulnerable to iodine deficiency, identifying a biomarker that accurately reflects iodine status during pregnancy is critical. The findings of our meta-analysis show that Tg concentration can be a sensitive indicator of iodine deficiency, specifically in populations of pregnant women with median UIC <100 μg/L, and it may provide a more reliable assessment than UIC alone when both measures are used in conjunction during pregnancy. However, these data should be interpreted cautiously, given the limited number of studies in populations of pregnant women with adequate iodine status. To confirm these findings, the sensitivity of Tg to determine different degrees of iodine deficiency needs to be evaluated in subsequent studies.
Footnotes
Author Disclosure Statement
None of the authors has any personal or financial conflicts of interest.
Funding Information
This study was supported by a financial grant from the Tehran University of Medical Sciences, Tehran, Iran.