
Abstract
Background:
Subclinical hypothyroidism (SCH) in pregnancy is associated with adverse pregnancy and perinatal outcomes. However, few studies have investigated the evolution of postpartum thyroid function in these women. This study aimed to determine the postpartum outcomes of SCH during pregnancy and the clinical and biochemical factors related to the evolution of long-term hypothyroidism.
Methods:
A total of 393 women diagnosed with SCH during pregnancy (defined as thyrotropin [TSH] >4.0 μIU/mL with normal free thyroxine levels according to the 2017 American Thyroid Association guidelines) were prospectively followed up after delivery. Among them, 216 underwent long-term follow-up [median (interquartile range) follow-up time: 11 (7–19) months] postpartum. The clinical and biochemical characteristics of the women with long-term postpartum hypothyroidism and euthyroidism were compared. Linear mixed model (LMM) was used to explore the risk factors for longitudinal changes of TSH, and logistic regression analysis was employed to identify the independent predictors of long-term postpartum hypothyroidism.
Results:
The probability of long-term hypothyroidism after delivery in SCH during pregnancy was 38.9%. Among the subjects with normal thyroid function 6-week postpartum, 28.2% developed hypothyroidism during long-term follow-up. The LMM showed that gestational age at the time of SCH diagnosis (estimate: −0.018, p = 0.004) and thyroid peroxidase antibodies (TPOAb) (estimate: 0.001, p = 0.020) were significantly associated with longitudinal changes of TSH. The logistic regression model showed that TPOAb positive both during pregnancy and six-week postpartum was a risk factor for long-term hypothyroidism after delivery (odds ratio = 4.686 [95% confidence interval 1.242 to 17.680], p = 0.023).
Conclusions:
More than one-third of patients with SCH during pregnancy had persistent hypothyroidism after delivery. We recommend that patients with TPOAb positive both during pregnancy and six-week postpartum undergo close follow-up to detect persistent hypothyroidism, especially before the next pregnancy.
Introduction
According to the 2017 American Thyroid Association (ATA) guidelines, subclinical hypothyroidism (SCH) in pregnancy is defined as elevated thyrotropin (TSH) beyond the upper limit of pregnancy-specific reference ranges with normal free thyroxine (fT4) levels (1). Previous studies have shown that the prevalence of SCH in pregnancy varies between 4% and 25%, depending on the trimester-specific reference ranges of TSH (2 –9). Several studies indicate that SCH in pregnancy is associated with adverse pregnancy and perinatal outcomes (10 –16). The 2017 ATA guidelines recommend levothyroxine (LT4) therapy to maintain a TSH value between the lower reference limit and 2.5 mU/L (1). However, the postpartum thyroid status and postpartum management of pregnant women with SCH are not specifically mentioned in the guidelines.
Most studies on thyroid disorders after delivery indicate that the incidence of persistent hypothyroidism varies between 20% and 40% during 3–12 years after an episode of postpartum thyroiditis (PPT) (17 –21). However, few studies have investigated the evolution of postpartum thyroid function in women with SCH during pregnancy. It was reported that ∼25% of gestational SCH subjects had persistent hypothyroidism after delivery, and those with thyroid peroxidase antibodies (TPOAb) positive during pregnancy were more likely to have postpartum hypothyroidism (22, 23). However, these studies did not observe the longitudinal changes of TSH, or had a small study cohort. To prevent adverse perinatal events caused by hypothyroidism, early identification of hypothyroidism in women of reproductive age is important because they may have subsequent pregnancies.
In this study, 393 women diagnosed with SCH during pregnancy were prospectively investigated to evaluate the clinical and biochemical factors associated with hypothyroidism on long-term follow-up.
Methods
Patient population
Patients diagnosed with SCH during pregnancy at the Department of Endocrinology and Metabolism of Shanghai General Hospital during December 2014 and March 2018 were recruited for our study. Subjects with known thyroid disease, use of any drugs that could affect thyroid function (amiodarone, lithium, estrogen, or corticosteroids), pregestational diabetes, pregestational hypertension, autoimmune disease (rheumatoid arthritis, systemic lupus erythematosus, or multiple sclerosis), or a lack of six-week postpartum thyroid function tests were excluded from the study. A total of 393 subjects were suitable for analysis, of which 216 women were followed for >6-month postpartum. The study and follow-up flow chart are shown in Figure 1.
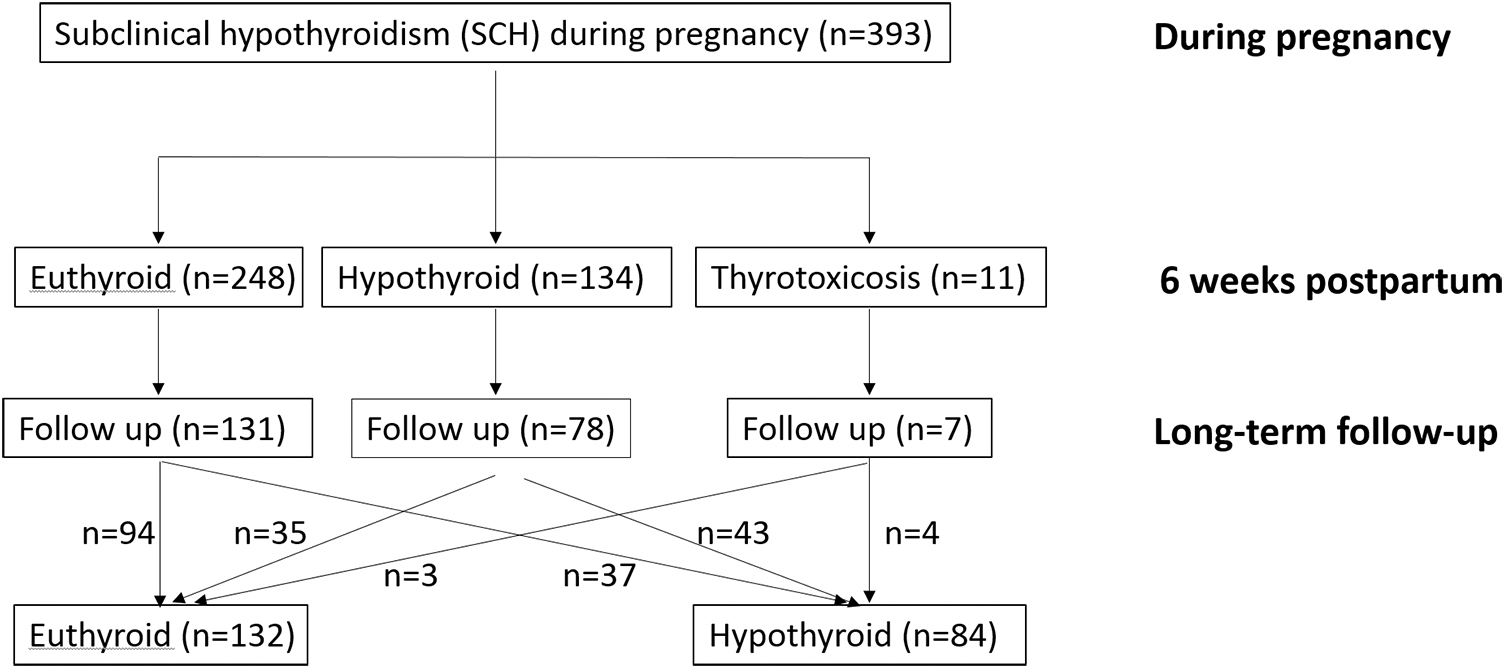
Flow diagram of the study cohort and outcomes during follow-up.
Study protocol and methods
In our hospital, thyroid function is routinely tested at 11–13, 24–28, and 34 weeks of pregnancy. The recruited patients stopped LT4 replacement after delivery and were followed up as follows: (i) thyroid functions were re-examined six-week postpartum synchronized with postnatal examination; (ii) if the TSH levels exceeded 10 μIU/mL, or if patients with TSH levels between 4 and 10 μIU/mL had symptoms of hypothyroidism, LT4 was prescribed and thyroid function was measured every 4–8 weeks according to the 2012 ATA/American Association of Clinical Endocrinologist guidelines (24); (iii) if hyperthyroidism was diagnosed, the thyrotoxic phase of PPT was differentiated according to 2017 ATA guidelines (1); and (iv) thyroid functions were measured every six months after delivery in SCH subjects without LT4 replacement or euthyroidism ones.
Clinical data including age at present pregnancy, gestational age at the time of SCH diagnosis, pregestational body mass index (BMI), 6-week postpartum BMI, family history of thyroid disease, parity, breastfeeding, LT4 replacement after delivery, oral glucose tolerance test, thyroid function [free triiodothyronine (fT3), fT4, TSH] (at the time of SCH diagnosis and 6-week and long-term postpartum follow-up), and thyroid autoantibodies (during pregnancy and at 6-week postpartum and long-term postpartum follow-up) were recorded. All patients stopped LT4 replacement after delivery, while 29 of 216 (13.4%) women restarted LT4 replacement during follow-up and continued until the end of follow-up.
There were no changes in thyroid function or thyroid autoantibodies testing methodology during the study period. fT3 and fT4 were evaluated by radioimmunoassay, and TSH was evaluated by immunoradiometric assay, using an automatic analyzer (GC-1500 gamma radioimmunoassay counter; USTC Chuangxin Co., Ltd., China). TPOAb and thyroglobulin antibodies (TgAb) were analyzed using an electrochemiluminescent immunoassay on a COBAS e602 analyzer (Roche Diagnostics, Mannheim, Germany). The reference ranges were as follows: fT3, 3.1–6.5 pmol/L; fT4, 9–23.2 pmol/L; TSH, 0.25–4 μIU/mL; TgAb, 10–115 IU/mL, and a titer >115 IU/mL was considered TgAb positive; TPOAb, 5–34 IU/mL, and a titer >34 IU/mL was considered TPOAb positive.
SCH during pregnancy and after delivery was defined as a TSH concentration elevated >4 μIU/mL with normal fT4 (1,19,24). Thyroid dysfunction was classified as hypothyroidism (SCH, as shown above; overt hypothyroidism, TSH >4.0 μIU/mL with fT4 < 9 pmol/L) and thyrotoxicosis (subclinical thyrotoxicosis, TSH <0.25 μIU/mL with normal fT4; overt thyrotoxicosis, TSH <0.25 μIU/mL with fT4 > 23.2 pmol/L). Euthyroidism was defined as normal TSH and fT4.
This study was approved by the hospital ethics committee.
Statistical analysis
Variables are expressed as the mean and standard deviation, or as the median and interquartile range (25–75%) as appropriate. Mean values were compared using Student's t-test when variables were normally distributed. Continuous variables without normal distribution were analyzed by the Mann–Whitney U-test. For categorical variables, the chi-squared test was used. For our data included repeated measurements (thyroid function and antibodies), linear mixed model (LMM), which can be used to analyze longitudinal data of individual changes over time and other factors likely to influence changes (25), was used to explore the risk factors for longitudinal changes of TSH, adjusted for age at present pregnancy, BMI, parity, family history of thyroid disease, coexistence with gestational diabetes mellitus (GDM), breastfeeding, gestational age at the time of SCH diagnosis, TgAb, and TPOAb. Logistic regression analysis was employed to identify independent predictors of long-term postpartum hypothyroidism, adjusted for age at present pregnancy, pregestational BMI, parity, family history of thyroid disease, coexistence with GDM, breastfeeding, gestational age at the time of SCH diagnosis, and thyroid autoantibodies (TgAb and TPOAb) status during pregnancy and six-week postpartum. The subjects were categorized into three groups according to their thyroid autoantibodies status: (i) both negative, negative during pregnancy and six-week postpartum; (ii) either positive, positive during pregnancy or six-week postpartum; and (iii) both positive, positive during pregnancy and six-week postpartum. p-Value <0.05 was considered statistically significant. Data were analyzed using the SPSS statistical package (SPSS version 19; IBM Corp., Armonk, NY).
Results
Prevalence of thyroid dysfunction at 6-week postpartum and long-term follow-up visits
For all 393 women diagnosed with SCH during pregnancy, LT4 was administered during pregnancy, and the dosage was titrated according to their thyroid function. After delivery, all patients stopped LT4 treatment. At 6-week postpartum, 248 (63.1%) women were euthyroid; 134 (34.1%) women had persistent hypothyroidism (one had overt hypothyroidism, while the other 133 had SCH); and 11 (2.8%) had thyrotoxicosis (3 had overt thyrotoxicosis, and 8 had subclinical thyrotoxicosis). At the end of follow-up [median length of follow-up of 11 (7 –19) months postpartum], 216 subjects remained in this study; 132 of the 216 (61.1%) subjects had normal thyroid function, and 84 (38.9%) subjects had hypothyroidism, of which 29 subjects were receiving LT4 replacement. Forty-five percent (177/393) of women dropped out, and there were no significant demographic or clinical differences between these women and those who remained in the study (Supplementary Table S1). The prevalence of hypothyroidism at 6-week postpartum follow-up visit was not significantly different from that of women at the long-term postpartum follow-up visit (Table 1).
Thyroid Function of Patients with Subclinical Hypothyroidism During Pregnancy at 6-Week Postpartum and Long-Term Follow-Up
Clinical and biochemical characteristics during and after pregnancy of subjects with long-term postpartum hypothyroidism and euthyroidism
The clinical and biochemical characteristics of subjects categorized by thyroid function at the end of follow-up (hypothyroid group, n = 84; euthyroid group, n = 132) are shown in Table 2. The gestational age at SCH diagnosis for these 216 patients was 22 (15 –27) weeks. The gestational age at SCH diagnosis in the hypothyroid group was significantly earlier than that in the euthyroid group [19 (14 –26) weeks vs. 24 (16 –28) weeks, p = 0.022]. However, there were no significant differences in age at present pregnancy, pregestational BMI, six-week postpartum BMI, parity, family history of thyroid disease, coexistence with GDM, or breastfeeding between the two groups.
Clinical Characteristics of Subjects with Subclinical Hypothyroidism During Pregnancy Who Developed Long-Term Hypothyroidism and Those Who Were Euthyroid After Delivery
Data are presented as the median (interquartile range: 25–75%) or n (%) as appropriate.
p < 0.05.
+, positive; BMI, body mass index; fT3, free triiodothyronine; fT4, free thyroxine; GDM, gestational diabetes mellitus; SCH, subclinical hypothyroidism; TgAb, thyroglobulin antibodies; TPOAb, thyroid peroxidase antibodies; TSH, thyrotropin.
At the time of SCH diagnosis during pregnancy, TgAb positivity (22.9% vs. 13.1%, p = 0.045), TgAb titer [17.03 IU/mL (10.00–99.21) vs. 13.19 IU/mL (10.00–28.01), p = 0.033], TPOAb positivity (26.5% vs. 13.8%, p = 0.015), and Ab (TgAb or TPOAb) positivity (33.7% vs. 19.2%, p = 0.012) were significantly higher in the hypothyroid group than in the euthyroid group. The TPOAb titer was slightly but not significantly higher [14.43 IU/mL (8.61–35.02) vs. 12.83 IU/mL (7.81–20.83), p = 0.059] in the hypothyroid group than in the euthyroid group. The results of the other thyroid function tests, fT3, fT4, and TSH concentrations, were not significantly different.
At 6-week postpartum, women in the hypothyroid group had higher TSH levels [4.16 μIU/mL (2.60–5.08) vs. 3.17 μIU/mL (2.55–4.07), p = 0.03]. The TPOAb positivity (20.5% vs. 8.6%, p = 0.008), Ab positivity (25.3% vs. 13.3%, p = 0.018), and TgAb titer [13.14 IU/mL (10.00–43.97) vs. 10.14 IU/mL (10.00–15.27), p = 0.019] were significantly higher in the hypothyroid group than in the euthyroid group, while there were no significant differences in other thyroid function test results, including fT3 and fT4 concentrations or TgAb positivity or TPOAb titer (p > 0.05). Of the 84 women with hypothyroidism, 51.2% of the subjects had SCH at 6-week postpartum, while in the euthyroid group, only 26.5% (35/132) were diagnosed with SCH at 6-week postpartum (p < 0.001).
Long-term follow-up of thyroid status in subjects with normal thyroid function 6-week postpartum
Of the 393 patients, 216 were followed up for >6 months, including 131 cases with normal thyroid function (Group 1), 78 cases with hypothyroidism (Group 2), and 7 cases with thyrotoxicosis (Group 3) 6-week postpartum. At the end of follow-up, 55.1% (43/78) of the women in Group 2 had persistent hypothyroidism, while 28.2% (37/131) of the women in Group 1 developed hypothyroidism (p < 0.01) (Table 3).
Long-Term Thyroid Function in Subjects with Different Thyroid Statuses at 6-Week Postpartum
Group 1: subjects who were euthyroid at 6-week postpartum. Group 2: subjects who were hypothyroid at 6-week postpartum. Group 3: subjects who were thyrotoxicosis at 6-week postpartum. There were significant differences among the three groups (p < 0.01), and there was a significant difference between Group 1 and Group 2 (p < 0.01).
Table 4 summarizes the clinical characteristics and thyroid function tests of the 131 women with euthyroidism at 6-week postpartum categorized by whether they remained euthyroid (euthyroid group, n = 94) or developed hypothyroidism (hypothyroid group, n = 37) during long-term follow-up. During pregnancy, the TPOAb positivity (38.9% vs. 15.1%, p = 0.003) and titer [20.09 IU/mL (10.37–69.03) vs. 13.48 IU/mL (7.51–20.83), p = 0.022] and Ab positivity (38.9% vs. 18.3%, p = 0.014) were higher in hypothyroid group than in euthyroid group. At 6-week postpartum, the TgAb positivity (21.6% vs. 5.5%, p = 0.006) and titer [14.99 IU/mL (10.00–87.04) vs. 10.14 IU/mL (10.00–14.56), p = 0.035], TPOAb positivity (32.4% vs. 7.7%, p < 0.001) and Ab positivity (37.8% vs. 11.0%, p < 0.001) were also higher in hypothyroid group (Table 4). No significant differences in the other clinical characteristics were found between the two groups (Table 4).
Comparison of Clinical and Biochemical Features of the Subjects Who Developed Long-Term Postpartum Hypothyroidism and Euthyroidism in 131 Euthyroid Subjects at 6-Week Postpartum
Data are presented as the median (interquartile range: 25–75%) or n (%) as appropriate.
p < 0.05.
Analysis of clinical and biochemical risk factors associated with longitudinal changes of TSH and long-term postpartum hypothyroidism
LMM method showed that gestational age at the time of SCH diagnosis (estimate: −0.018, p = 0.004) and TPOAb (estimate: 0.001, p = 0.020) was significantly associated with longitudinal changes of TSH (Table 5). While age at present pregnancy, BMI, parity, family history of thyroid disease, coexistence with GDM, breastfeeding, and TgAb were not significantly associated with longitudinal changes of TSH. Logistic regression analysis indicated that women with TPOAb positive both during pregnancy and six-week postpartum were more likely to develop long-term postpartum hypothyroidism than those with TPOAb negative at that time (odds ratio = 4.686 [95% confidence interval 1.242 to 17.680], p = 0.023) (Table 6). Age at present pregnancy, BMI, parity, family history of thyroid diseases, coexistence with GDM, breastfeeding, gestational age at SCH diagnosis, and TgAb status were not significantly associated with long-term postpartum hypothyroidism.
Linear Mixed Model of Risk Factors for Longitudinal Changes of Thyrotropin
p < 0.05.
CI, 95% confidence interval.
Logistic Regression Model for the Risk Factors of Developing Long-Term Hypothyroidism After Delivery
p < 0.05.
OR, odds ratio.
Progression of thyroid function in subjects with thyrotoxicosis at 6-week postpartum
At 6-week postpartum, 11 subjects developed transient thyrotoxicosis. Four patients dropped out during follow-up, and seven patients stayed in the cohort, with an average follow-up time of 16.4 months (Supplementary Table S2). Of the seven patients, five had subclinical thyrotoxicosis, and two developed overt thyrotoxicosis. At the end of follow-up, three subjects returned to normal thyroid function, while the other four subjects, one of whom was on LT4 treatment, developed persistent SCH. The clinical characteristics and evolution of thyroid function were as follows: (i) two patients were transiently euthyroid and had subsequent persistent SCH; (ii) two patients had persistent SCH; (iii) one patient had transient hypothyroidism, with a return to the euthyroid state; and (iv) two patients had normal thyroid function (Supplementary Table S2).
Discussion
We prospectively evaluated the prevalence of thyroid dysfunction both during short-term (6-week postpartum) and long-term follow-up [median length of follow-up was 11 (7 –19) months postpartum] in women with SCH during pregnancy. Among them, 55% (216/393) of women were followed for a longer period. The major finding in our study was that 34.1% of women with gestational SCH had hypothyroidism at 6-week postpartum, while 38.9% had persistent hypothyroidism at the end of long-term follow-up. Haddow et al. showed that 64% of women with hypothyroidism during pregnancy were diagnosed with overt hypothyroidism over >10 years of follow-up (26). However, Shields et al. found that 24.6% (16/65) of SCH patients during pregnancy had persistently high TSH levels (TSH >4.5 mIU/L) over 5 years postpregnancy (22), and Neelaveni et al. found that 17.8% (83/147) of women developed hypothyroidism at the end of 2-year follow-up (23). In our study, a TSH level >4 μIU/mL was used to diagnose SCH in pregnancy, while in Haddow's study the TSH levels in women with hypothyroidism during pregnancy were much higher (mean 13.2 mIU/L), which was determined by a serum TSH concentration at or above the 98th percentile of the values in all the 25,216 pregnant women. The other two studies used the trimester-specific TSH reference range for gestational SCH diagnosis. Therefore, the differences in the prevalence of long-term postpartum hypothyroidism between our study and the others could be explained by the different SCH diagnostic criteria both during and after pregnancy and follow-up periods. Since the prevalence of persistent hypothyroidism during the postpartum period seemed to increase over time, women with SCH during pregnancy were advised to undergo follow-up evaluations of their thyroid function after delivery.
We observed that the gestational age at the time of SCH diagnosis was earlier in patients with long-term hypothyroidism. In addition, the LMM showed that gestational age at SCH diagnosis was inversely related to the increase of TSH levels, which suggested that the earlier that hypothyroidism was determined during pregnancy, the higher postpartum TSH levels were, and the more likely the patient would have hypothyroidism after delivery. Previous studies have not reported the association between SCH diagnosis time and long-term changes of TSH levels after delivery. We speculate that those with earlier diagnosis of SCH during pregnancy seemed to have worse thyroid status, so their thyroid function does not return to normal after delivery.
Consistent with previous studies (9,27,28), our results suggest that TPOAb was an independent risk factor for elevated TSH levels. And subjects who were TPOAb positive both during pregnancy and six weeks after delivery were more likely to develop long-term postpartum hypothyroidism. Therefore, TPOAb is recommended to be checked in gestational SCH patients during pregnancy and 6-week postpartum even if they are euthyroid at 6-week postpartum. The thyroid disorder is, in part, a consequence of antibody-dependent cell-mediated cytotoxicity generated by TPOAb (29 –31). Anti-TPO antibodies from autoimmune thyroid disease patients can fix complement, destroy thyrocytes, and act as competitive inhibitors of enzymatic activity (32). In addition, it has been documented that immune reactivity increases after delivery, which includes the switch from Th2-type immune response of gestation to the Th1 status postpartum (33,34).
In this study, hyperthyroidism or subclinical hyperthyroidism was found in 11 of the 393 patients at 6-week postpartum. Among seven patients who were followed, the thyroid function of three returned to normal, while the other four subjects developed persistent SCH. PPT is a transient thyroid dysfunction that occurs during the first year postpartum. Half of the PPT patients experienced isolated thyrotoxicosis or hyperthyroidism followed by hypothyroidism. Antithyroid drugs are not necessary during the thyrotoxic phase because this phase of PPT is a destructive thyroiditis and is commonly transitory and typically mild. Lucas et al. (35) reported 45 patients with PPT, 26 of whom had transient thyrotoxicosis. Of the 26 patients, 7 (26.9%) developed persistent hypothyroidism, and the rest had returned to normal thyroid function (35). Filippi et al. reported that 34.9% (15/43) of patients with PTT developed SCH 1-year postpartum (36). Therefore, women with PTT need to be closely followed up for early detection of hypothyroidism and timely treatment.
One limitation to our study needs to be considered when interpreting our findings. Among the 393 subjects, 216 cases were followed up for >6 months after delivery, while 177 patients were lost to follow-up. However, patients who were lost to follow-up and who had long-term follow-up were comparable in both clinical and biochemical parameters.
In conclusion, more than one-third of women with SCH during pregnancy had long-term hypothyroidism after delivery. SCH is an important cause of infertility, and SCH during pregnancy is associated with negative repercussions for both the mother and her newborn. Thus, we recommend postpartum follow-up of thyroid function for women with gestational SCH, particularly those who are TPOAb positive both during pregnancy and six-week postpartum.
Footnotes
Acknowledgment
We thank Prof. Mei Kang, Clinical Research Center, Shanghai General Hospital, Shanghai Jiao Tong University for statistical advice.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
This work was supported by National Natural Science Foundation of China (Grant No. 81870610), Shanghai Science and Technology Commission Foundation (Grant No. 18411968800), and the Clinical Research Innovation Plan of Shanghai General Hospital (Grant No. CTCCR-2018C13).
Supplementary Material
Supplementary Table S1
Supplementary Table S2