
Abstract

Introduction
As a follow-up to the opening session of the 2019 Annual Meeting of the American Thyroid Association, herein I provide a summary of recent original research manuscripts influencing surgical thyroidology. For those interested in more detail and analysis, many of these papers have been reviewed in recent issues of Clinical Thyroidology.
During the past several years, the field of thyroid surgery has evolved progressively toward a de-escalation and personalization of care (Fig. 1). At the peak of surgical aggressiveness circa 2012, prophylactic central neck dissections were being advocated for patients with small papillary thyroid carcinomas (PTCs). The advent of molecular diagnostic tools in 2012, such as the Afirma and Thyroseq tests, reduced the burden of unnecessary surgery for patients with indeterminate thyroid nodules. The publication of the 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer exerted considerable influence in the de-escalation process, principally by liberalizing the use of lobectomy for intrathyroidal PTCs 1–4 cm in diameter and proposing active surveillance as an acceptable management strategy for very low-risk PTCs (1).

The evolution of thyroid surgery, 2012–2019.
In 2016, the term noninvasive follicular thyroid neoplasm with papillary-like nuclear features was introduced, bringing recognition to the fact that an indolent subset of neoplasms previously termed malignant actually had no invasive potential, thus relieving a significant subset of patients from the clinical and psychological burden of a cancer diagnosis (1). Second-generation molecular tests, Afirma GSC and Thyroseq v3, were released by 2018 with improved performance characteristics, permitting a greater proportion of patients with indeterminate nodules to avoid diagnostic hemithyroidectomy (2,3). The changes just mentioned have had an enormous impact on the daily practice of surgical thyroidology. However, the surgical technique itself has remained largely unchanged during this period, for the simple reason that the standard operation has performed consistently well in the hands of experienced surgeons. In other words, recent advances in surgical thyroidology have centered almost entirely on the decision-making process surrounding surgery rather than surgery itself.
Methods
Peer-reviewed original research publications in surgical thyroidology were extracted from multiple sources, including recommendations from the American Thyroid Association members, articles reviewed in Clinical Thyroidology, and an independent literature review. Reports published from January 1, 2018 to September 30, 2019 that addressed the Who, What, Where, When, Why, and How of surgery for benign and malignant thyroid conditions were included.
Who (should have surgery)? Patient selection for surgery versus medical management or observation.
What (operation)? Extent of surgery guided by preoperative evaluation (including molecular markers).
Where (should surgery be performed)? Surgical outcomes and quality.
When (to intervene)? The timing of surgery.
Why (should we operate or not)? New data regarding the risks and benefits of surgery.
How? Innovations in surgical technique and perioperative care.
Results
Who (should have surgery)?
Active surveillance is now an accepted management option in select patients with very low-risk PTC. In April 2019, Oh et al. published a prospective cohort study examining clinical and sonographic predictors of rapid tumor volume doubling time in 273 patients with papillary thyroid microcarcinoma (4). Patients were stratified into either a rapid-growing group (tumor volume double time <5 years) or a stable group (tumor volume double time >5 years) based on the rate of growth observed over serial ultrasound measurements over a median follow-up time of 42 months. Predictors of rapid tumor growth included age <50 years and the presence of macrocalcifications. The study by Oh et al. confirmed that active surveillance is safe for certain patients with PTC, supporting previous findings by Ito et al. (5) and Tuttle et al. (6) on the predictive significance of tumor volume kinetics and patient age.
What (operation)?
The advent of molecular testing in 2012 transformed the treatment landscape for patients with cytologically indeterminate (Bethesda 3 and 4) nodules. Given the relatively low prevalence of cancer (5–30%) in these nodules, the majority of diagnostic hemithyroidectomies were unnecessary. During the past year, two important clinical validation studies examining the performance of second-generation molecular tests were published. In September 2018, Patel et al. published a prospective, multicenter, blinded analysis of a genomic sequencing classifier (Afirma GSC) involving 183 patients, all of whom underwent surgery (2). Mechanistically, Afirma GSC involves nuclear and mitochondrial RNA transcriptome gene expression, RNA sequencing, and genomic copy number analysis. Afirma GSC had a benign call rate of 54% at a cancer prevalence of 24%. When compared with the prior generation Afirma gene expression classifier, Afirma GSC exhibited improvement in specificity from 50% to 68% while maintaining a high sensitivity of 91%. The gains in specificity were largely attributed to an improvement in the correct diagnosis of benign Hurthle cell lesions.
In February 2019, Steward et al. published a prospective, multicenter, blinded analysis of a multigene genomic classifier (Thyroseq v3) involving 286 nodules with all patients undergoing surgery (3). Thyroseq v3 detects five classes of genomic alterations, including point mutations, insertions/deletions, gene fusions, copy number alterations, and gene expression alterations. Thyroseq v3 exhibited a sensitivity of 94% and a specificity of 82% in the diagnosis of Bethesda 3 and 4 nodules. Sensitivity and specificity changed from 95% to 98% and from 43–93% to 82%, respectively. Both of these tests are highly sensitive; the correspondingly low false negative rate now allows more than half of patients with indeterminate thyroid nodules to safely avoid diagnostic hemithyroidectomy. In June 2018, Livhits et al. published a prospective, randomized, pragmatic clinical trial of 149 indeterminate nodules comparing the performance of the (now) prior generation Afirma and Thyroseq tests. This study demonstrated a higher specificity for Thyroseq v2 (91% vs. 66%) and a higher positive predictive value for Thyroseq v2 (57% vs. 39%) compared with Afirma gene expression classifier (7). The same group is now using an identical study design to assess the current-generation molecular tests.
We have now entered an era when molecular markers provide not only diagnostic value but also prognostic value in the management of known or suspected thyroid cancer. Two 2018 studies by the same international consortium of investigators examined the interaction between the BRAFV600E mutation and clinical factors in the prognosis of PTC. In February 2018, Shen et al. published a retrospective, multicenter cohort study of 2638 patients to test whether the prognostic risk of age is determined by the presence of BRAFV600E (8). In patients with wild-type BRAF, age did not influence mortality; the mortality rate was very low even in patients of advanced age. In contrast, the effect of increasing age was clearly visible in patients harboring the BRAFV600E mutation; young patients exhibited negligible rates of mortality, whereas patients aged 65+ exhibited disease-specific mortality rates approaching 50% at 15 years. In September 2018, Wang et al. examined the same cohort of 2638 patients to test whether the prognostic risk of male sex is determined by the presence of BRAFV600E (9). They found no influence of male sex on disease-specific mortality in patients with wild-type BRAF. However, in patients with BRAFV600E PTC, mortality rates were 6.6% in men versus 2.9% in women (hazard ratio 2.74 [confidence interval, CI 1.38–5.43]). Taken together, the two studies just cited demonstrate that BRAFV600E mutation interacts with both patient age and sex as regards prognosis in PTC. In this light, should surgeons be aware of a BRAFV600E mutation preoperatively, they may consider a more aggressive initial operation in some patients. A potential application of these new findings would be to consider a total thyroidectomy instead of a lobectomy for a BRAFV600E-positive solitary intrathyroidal PTC, particularly if the tumor diameter exceeds 2 cm (10).
Where (should surgery be performed)?
Though the volume-outcome relationship has received sufficient attention in past years, a brief discussion of surgical quality and outcomes is warranted. In February 2018, Kim et al. assessed the relationship between surgeon volume and structural recurrence or persistence in N1b PTC (11). High-volume and low-volume surgeons were defined as having 100+ or <100 operations a year, respectively. In this retrospective study of 1103 patients, high-volume surgeons had a 15% disease recurrence rate whereas low-volume surgeons had a 27% disease recurrence rate (hazard ratio 1.46 [CI 1.08–1.96]) with a median follow-up time of 81 months. No differences were found with respect to the development of distant metastases or disease-specific mortality.
When (to intervene)?
With rare exceptions, thyroidectomy has historically been the first treatment for thyroid cancers of all histologic subtypes. A report by Wang et al., published in August 2019, may signal a paradigm shift in the treatment of anaplastic thyroid carcinoma (12). The efficacy of neoadjuvant dabrafenib (a BRAF inhibitor) and trametinib (an MEK inhibitor) followed by surgical resection was examined in a series of six patients with anaplastic thyroid carcinoma confirmed by core biopsy before initiation of treatment. These new agents have been used successfully in BRAF-mutated melanoma (13). Significant reductions in viable tumor mass were observed on both PET scan and histopathologic analysis, permitting complete surgical resection in all patients. All patients survived six months. Two patients died of distant metastases after 8 and 14 months, with the remaining four patients demonstrating no evidence of disease at last follow-up. These remarkable results are an example of molecular markers guiding neoadjuvant therapy to achieve outcomes that are visibly superior to those that have been historically observed in the treatment of a highly aggressive malignancy. With further study, targeted neoadjuvant therapy may become the standard of care in the management of select cases of anaplastic thyroid carcinoma.
Why (should we operate or not)?
Indications for surgical intervention may evolve as thyroidectomy is proven more harmful or more beneficial than previously recognized for individual conditions. In August 2019, Guldvog et al. published a prospective randomized trail comparing total thyroidectomy and standard medical management for 150 euthyroid patients with Hashimoto's thyroiditis and persistent constitutional symptoms (14). The inclusion criteria were extensive. Enrolled patients had serum anti-TPO antibody levels greater than 1000 IU/mL (normal <100 IU/mL), and thyrotropin (TSH) levels above 3.5 mIU/L (normal range 0.2–3.5 mIU/L) before hormone replacement. They were then confirmed to have achieved biochemical euthyroid status on thyroid hormone. Typical symptoms reported included fatigue, sleep disturbance, musculoskeletal pain, and dry mouth and eyes. After 18 months, surgically treated patients displayed an improvement in general health scores (measured by the Short Form-36 Health Survey) from 38 to 64 points, for a between-group difference of 29 points [CI 22–35 points]. This same pattern—substantial improvement in the surgery group versus no change in the control group—was observed in each individual domain of the health survey. Surgically treated patients also experienced reduced fatigue scores and less commonly reported chronic fatigue in comparison to medically managed controls. This study, though compelling, was unable to control for the placebo effect of surgery and has limited generalizability because of the strict inclusion criteria. Further, surgical complication rates were not insignificant in these cases characterized by severe inflammation (hypoparathyroidism 4.1%, unilateral recurrent laryngeal nerve palsy 5.5%).
Two important studies on the management of Graves' disease were published in the past year (15,16). These papers by Okosieme and Kitahara are discussed in the medical review by Dr. Naifa Busaidy in this same issue of Thyroid. Briefly, the former study reported that early definitive control of TSH is associated with reduced risk of cardiovascular events in patients with Graves' disease, and the latter demonstrated an increased risk of solid-cancer mortality after 131I treatment for hyperthyroidism. Historically, about 5% of patients with Graves' disease have undergone thyroidectomy in the United States (17). The recent findings by Okosieme and Kitahara suggest that thyroidectomy should likely be considered as first-line treatment for Graves' disease more often than that.
How? Innovations in surgical technique and perioperative care
In January 2018, Anuwong et al. compared the safety and outcomes of the transoral endoscopic thyroidectomy vestibular approach (TOETVA) with those of open thyroidectomy by retrospectively analyzing 216 propensity score-matched pairs (18). TOETVA, first described by Anuwong in 2016, involves placing three laparoscopic ports through the sulcus behind the bottom lip and in front of the incisors (19). A midline tunnel is then created by working under the platysma, over the chin, and then down between the strap muscles. Compared with open thyroidectomy, TOETVA required longer operative times (100 minutes vs. 80 minutes), resulted in lower pain scores, and had similar complication rates. The authors reported 6 conversions to open surgery (1.4%), 20 seromas (4.7%), and 3 transient mental nerve injuries (0.7%). This favorable safety and feasibility profile has spurred the dissemination of TOETVA from its native Thailand to almost 50 centers in 13 countries over the past 4 years. At present, contraindications to TOETVA include a thyroid lobe measuring greater than 10 cm, cancer greater than 2 cm, benign nodule greater than 6 cm, the need for neck dissection, substernal goiter, and prior neck surgery.
Discussion: De-Escalation and Its Discontents
The last new article discussed in this review is a mathematical simulation that provides insight regarding the population-level effects of de-escalating the role of surgery in managing thyroid nodules and thyroid cancer. In October 2018, White et al. published a cost-effectiveness analysis comparing the Revised American Thyroid Association's 2015 to 2009 Guidelines for the Management of Patients With Thyroid Nodules and Differentiated Thyroid Cancer (20). For those unfamiliar with the field, cost-effectiveness analysis begins with the establishment of certain assumptions about the most common clinical scenarios encountered within a disease process. Derived from literature review, these assumptions include information such as the probability of malignancy within a nodule, the likelihood of death or disability from disease and/or treatment, the cost of procedures and medications, and the quality of life associated with chronic thyroid hormone supplementation. To account for uncertainty, assumptions are varied along a distribution while thousands of simulated patients are processed through the model. The analysis by White et al. demonstrated that the more surgically conservative 2015 guidelines dominated the 2009 guidelines as a management strategy. That is to say, the 2015 strategy delivered greater average quality-adjusted life years (13.09 vs. 12.43) at a lower average cost ($14,752 vs. $20,126) than the 2009 strategy. The advantages of the 2015 strategy arose from fewer fine needle aspirations, less surgery, and fewer surgical complications, including perioperative deaths. Importantly, however, the 2015 strategy led to a slight increase in the number of cancer deaths. The authors noted that the effect of de-escalation on overall rates of cancer-specific survival was small and entirely offset by a reduction in surgical mortality.
The report by White et al. poignantly encapsulates what I perceive to be a fundamental shift in our ethical approach to thyroid nodules and cancer. For perspective, let us revisit a 2006 commentary by Mazzaferri on managing small thyroid cancers (21). In this piece filled with wisdom and prescience, a giant in the thyroid cancer world expounded on the risk of metastases and cancer-specific death arising from papillary thyroid microcarcinomas, advocating aggressive treatment of these very low-risk tumors with routine total thyroidectomy and radioactive iodine. These claims would no longer be supported in the modern evidence environment. Mazzaferri admitted that “Even though many patients might not require such aggressive therapy, at present it is not possible to confidently identify who they are.” Put another way, he advocated subjecting large numbers of patients to excessive treatment to prevent the rare cancer death, effectively assigning little or no value to treatment-related morbidity. Cost-effectiveness analysis allows us to assign appropriate value to the burden of overtreatment.
The ethical dilemma of thyroid cancer management may be expressed metaphorically as a “trolley problem.” In the original trolley problem (Fig. 2A), a trolley races toward five people who are tied to the tracks, facing certain death. The protagonist has the opportunity to throw a switch that will re-direct the trolley to a new track where it will kill only one person. Should they throw the switch? The “thyroid cancer trolley problem” (Fig. 2B, C) is a variation where the protagonist must choose between directing the trolley toward killing one person (a metaphor for cancer death) and injuring a large number of people (a metaphor for overtreatment). The cost-effectiveness analysis by White et al. forces us, the members of the American Thyroid Association, to confront the fact that we have now chosen to direct the trolley to the upper track, that is, we have decided to accept a small number of cancer deaths to avoid the greater total harm brought about by large-scale overtreatment.
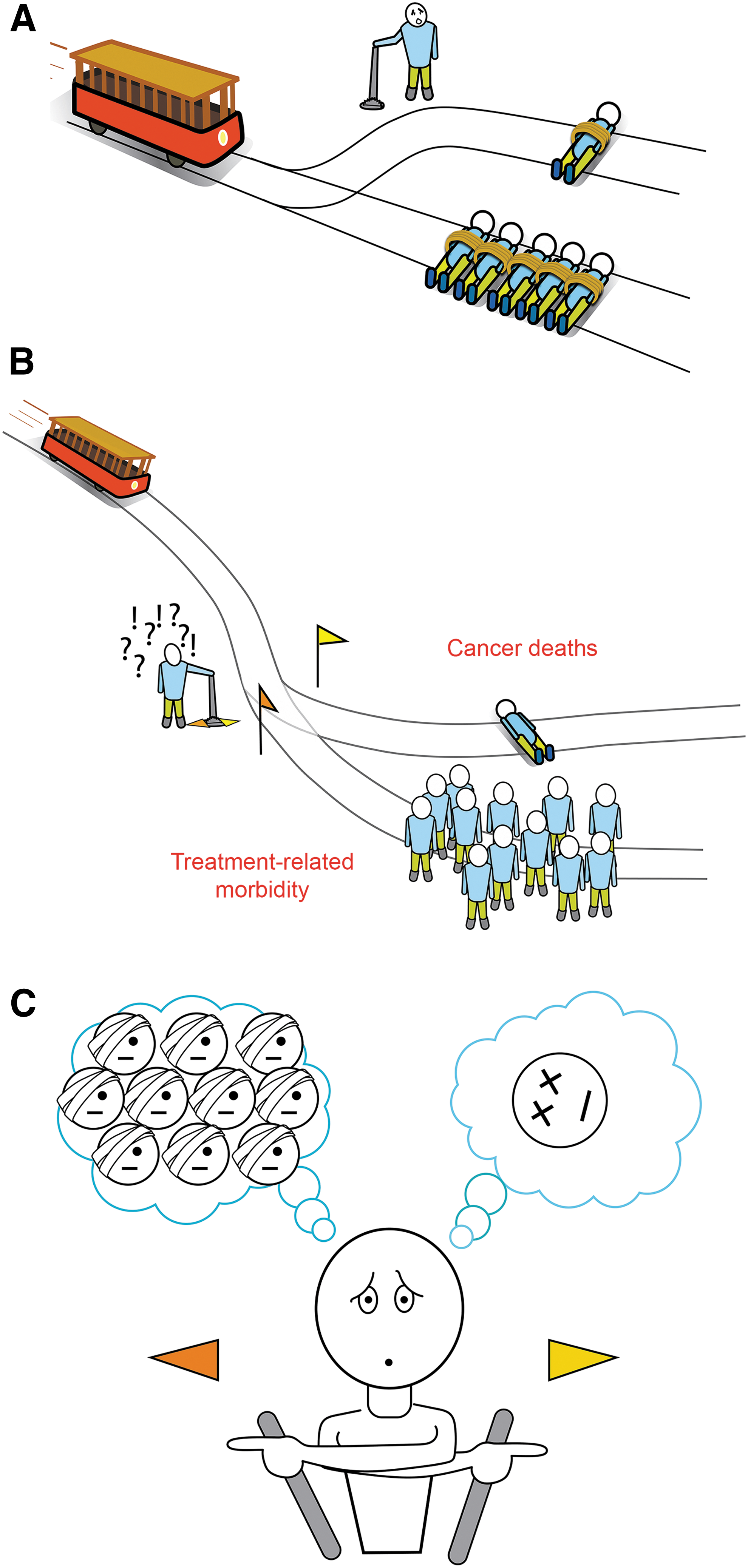
(
Conclusion
The field of surgical thyroidology has evolved considerably over the past year. Though small, incremental changes have been observed in surgical technique; larger and more fundamental shifts have occurred in the decision-making process that surrounds surgery (Box 1). Supported by the growing informational value of molecular markers, thyroid surgeons are better poised than ever to offer just the right amount of surgery (neither too much nor too little) to their patients.
Footnotes
Acknowledgment
The author thanks Martin Bruinsma for the trolley illustrations.
Author Disclosure Statement
The author has no conflicts of interest, commercial associations, or financial ties to disclose.
Funding Information
No funding was received for this article.