
Abstract
Background:
Measurements of both basal (b) calcitonin (CT) and calcium (Ca)-stimulated CT (Ca-sCT) levels are performed to identify medullary thyroid cancer (MTC) at an early stage when used as part of the diagnostic workup of thyroid nodules (CT screening). Novel immunochemiluminometric assays, which are highly sensitive and specific for monomeric CT and avoid cross-reactivity, have been introduced over the past decade. No prospectively generated data have so far become available to answer the frequently raised question as to whether Ca-sCT in contrast to bCT alone is helpful and, therefore, still indicated for the early detection of MTC.
Methods:
Ca-stimulation tests were performed in 149 consecutive patients with thyroid nodules and elevated bCT. Regardless of Ca-sCT levels, all patients had an operation applying a uniform surgical protocol, including thyroidectomy and systematic lymph node dissection. Recently published sex-specific cutoff levels for the differentiation of MTC and other C-cell pathologies (C-cell hyperplasia [CCH]) were used to compare the diagnostic performance of bCT or Ca-sCT alone and in combination using receiver-operating characteristic (ROC) analysis. In addition, CT cutoff levels to predict lateral lymph node metastasis were evaluated for bCT compared with Ca-sCT. Follow-up for all patients was documented and correlated with initial CT levels.
Results:
MTC was identified in 76 (50.1%) patients, in 21/76 (27.6%) with lymph node and in 4 (5.3%) with distant metastasis. Using predefined cutoff levels, patients could effectively be subdivided into a group above the cutoff level with definitive diagnosis of MTC (100%) and below (gray zone) with a significant overlap of CCH and MTC (all classified as pT1a; males: 19/58 [37.5%], females: 7/41 [17.1%]). The areas under the ROC curve (AUC) were excellent for the diagnosis of MTC in all tests. Determination of bCT proved to be superior for both diagnosing MTC in males (AUC for bCT: 0.894; AUC for Ca-sCT: 0.849) and females (bCT: 0.935; Ca-sCT: 0.868) and also for diagnosing lymph node metastasis in the lateral compartment (males: bCT: 0.925; Ca-sCT: 0.810; females: bCT: 0.797; Ca-sCT: 0.674). Combining both tests did not improve diagnostic accuracy. Using a cutoff level of >85 pg/mL for females and >100 pg/mL for males, the sensitivity for diagnosing lateral neck lymph node metastasis was 100%. Below these cutoff levels, no patient showed persistent or recurrent disease (median follow-up: 46 [ ± 27] months).
Conclusions:
Predefined sex-specific bCT cutoff levels are helpful for the early detection of MTC and for predicting lateral neck lymph node metastasis. Ca-sCT did not improve preoperative diagnostics. bCT levels >43 and >100 pg/mL for males and of >23 and >85 pg/mL for females are relevant for advising patients and planning the extent of surgery.
Introduction
Calcitonin (CT) is the established preoperative tumor marker for medullary thyroid cancer (MTC). In the case of thyroid nodules with elevated CT, a reasonable suspicion of thyroid C-cell malignancy is indicated. However, sporadic hypercalcitoninemia is not thyroid-C-cell-derived in all patients and does not always warrant a therapeutic intervention. The value of CT is influenced by analytical, physiological, pharmacological, and pathological factors in patients with and without thyroid abnormalities. Release of CT in C-cell disease can be stimulated by intravenous injection of stimulating agents, for example, pentagastrin or calcium (1).
Stimulation tests are used to differentiate MTC from other rare conditions in which mainly nonthyroid diseases (e.g., hypergastrinemia, hypercalcemia, renal insufficiency, and neuroendocrine tumors) are responsible for the elevation of serum CT (2). A significant rise of serum CT levels after stimulation is only expected in patients with MTC (3 –5).
In the past decade, commercial assays for measuring CT have progressed to the newest immunochemiluminometric assays that are highly sensitive and specific for monomeric CT. The cross-reactivity with other CT-related peptides is largely but not completely eliminated, thus improving sensitivity and specificity for diagnosing MTC. Therefore, these “new” CT assays are recommended whenever CT screening is part of the workup of thyroid nodules (6).
As shown in the literature, CT screening in patients with thyroid disease reduced the TNM stages of sporadic MTC comparing the periods before and after the routine measurements of serum CT (7) and biochemical cure rates improved (8).
Although routine serum CT screening in patients undergoing evaluation for thyroid nodules appeared to be cost-effective (comparable with the measurement of thyroid-stimulating hormone, colonoscopy, and mammography screening) (9), there still is an ongoing discussion concerning its practical value. While European guidelines recommend this procedure, Anglo-American guidelines are more restricted (6,10).
Because expert opinions vary regarding the usefulness of routinely measuring serum CT levels in patients with nodular goiters, the members of the American Task Force suggested that the individual physician should decide whether CT determinations are useful in the particular clinical situation (6).
Ultrasensitive CT assays have mostly eliminated false-negative rates of a basal CT (bCT) measurement when diagnosing C-cell disease. However, as higher bCT levels are pathognomonic for advanced MTC, diagnostic uncertainty exists at lower bCT concentrations (“gray zone”) during CT screening. To increase the sensitivity of bCT in these cases, the application of CT stimulation tests has been recommended (10 –14).
This prospective study aimed, on the one hand, to verify and confirm recently defined sex-specific bCT and calcium (Ca)-stimulated (Ca-sCT) cutoff levels for a more precise early diagnosis of MTC (1) and to confirm independently acquired data from another study group (13,15).
To our knowledge, this is the first study to prospectively investigate whether Ca-sCT compared with bCT is still helpful in improving the diagnosis of MTC and to predict the presence of lymph node metastasis in the era of novel immunochemiluminometric CT assays in patients with elevated bCT concentrations in general and, in particular, in those with “borderline” elevated CT increase, as recommended (16).
To answer these questions, this study was designed to analyze patients with elevated CT levels diagnosed within a CT screening program applying one single, prospective, diagnostic, surgical, and pathohistological protocol.
Patients and Methods
Prospective protocol
Austria is an iodine-replete endemic goiter region (17,18). In 1994, the routine determination of CT concentrations (CT screening) was introduced into the workup of nodular thyroid disease at the Medical University of Vienna (a tertiary care center) regardless of thyroid function, ultrasound morphology, and/or size of the thyroid nodule(s).
As compared with 1.1 cases of MTC per 1000 patients with nodular thyroid diseases diagnosed at the Medical University of Vienna before CT screening was initiated, 3.2 cases of MTC per 1000 patients were identified when bCT was determined in all patients with thyroid nodules (19).
As not all patients with thyroid nodules and mildly elevated bCT levels have MTC and are candidates for thyroid surgery, only subjects with bCT levels ≥10 pg/mL underwent a CT stimulation test using pentagastrin as stimulation agent, regardless of the patients' sex or the immunoassay available at that time (20) to more precisely predict MTC (21,22). However, pentagastrin, which was not available worldwide, was definitively taken off the European market by the end of 2015. Therefore, stimulation by Ca gluconate was initially recommended and introduced into clinical routine without clear cutoff CT levels.
As shown recently (1), Ca is able to replace pentagastrin to predict MTC with a similar diagnostic power using newly defined sex-specific cutoff values.
Because patients with Ca-sCT concentrations at least twofold higher than bCT levels or >100 pg/mL have a substantial risk of MTC, patients were offered an operation if there was no relevant comorbidity (20). In patients who fulfilled the criteria (20), a uniform surgical (23,24) and pathological (25) protocol, both parts of the standard operative procedure (SOP) to diagnose and treat MTC, was followed rigorously.
As part of the SOP, a standardized ultrasound of the neck was performed in all patients to confirm thyroid nodules of various sizes and morphology. However, the findings were not used for surgical decision-making, as previous analyses revealed an unsatisfying sensitivity of ultrasound to detect particularly microMTCs. In addition, the sensitivity for diagnosing lymph node metastases was seen to be low, especially for micro-metastasis (23,26).
Fine needle aspiration biopsy (FNAB) or CT measurements in wash-out fluid from fine needle aspiration (27) were not performed in this series, as routine bCT measurements have been documented to show a higher sensitivity to diagnose MTC compared with fine needle aspiration cytology, especially in diagnosing small (≤10 mm) curable MTC (28).
Patients
In 5 years (2012–2016), 149 consecutive patients visited one of the three outpatient departments of Vienna General Hospital at the Medical University. These patients presented with various thyroid nodular diseases detected by standardized ultrasound of the neck, with normal thyroid function tests and elevated bCT levels (confirmed at least one time on repeat measurements), and had an operation after performing a Ca stimulation test.
No patient who was a member of a known MTC family or who had undergone prior surgery for MTC was included in the study.
All patients had normal or nearly normal kidney function (glomerular filtration rate ≥45 mL/min/1.73m2) and other causes modifying bCT levels (e.g., intake of proton-pump inhibitors) were excluded before applying the Ca stimulation test.
The Ethics Committee of the Medical University of Vienna approved the clinical standard protocol, including all diagnostic and therapeutic procedures in thyroid nodules, in the case of elevated bCT concentrations further actions and the retrospective analysis of the patients' records (EK1506/2014). Informed consent to all diagnostic and surgical procedures was obtained from each patient, adhering to the Declaration of Helsinki. All biochemical and morphological data were collected prospectively and were analyzed retrospectively correlated to histological findings in the thyroid gland and lymph nodes after applying the same standardized surgical protocol in all patients.
To increase the power of the analysis, the data included in this study were pooled with those obtained in a previous preliminary study following the same SOP (1).
Biochemical analysis
The CT concentrations were determined with an immunochemiluminescent assay (ICMA) from Diagnostic Products Corporation (DPC, Los Angeles, CA), running as a fully automated test on a Siemens 2000 Immunoassay System (Siemens Health Care), as previously described in detail (22). This ICMA has been used worldwide in many publications. Therefore, the results of this study are comparable with findings in other studies using the same assay.
Calcium-stimulated CT test
Blood samples for CT determination were drawn with an indwelling catheter before (0) and 2, 3, and 5 minutes after a 30-second infusion of 2.5 mg Ca/kg body weight (Ca gluconate 10% [10 mL containing Ca gluconate 2.25 mmol = 90 mg Ca++; Calcium Braun 10%®; B. Braun Melsungen AG, Melsungen, Germany]), as recently described in detail (1).
Surgery
Total thyroidectomy and bilateral central neck lymph node microdissection (level 6) were performed in all patients regardless of preoperative bCT and sCT levels (23).
During initial surgery, systematic microdissection of both lateral neck lymph node compartments (levels 2–5) saving the internal jugular vein, all nerves and muscles (“functional” dissection) (24,29) was performed without transsternal mediastinal dissection (compartment C4) as part of the surgical SOP in all patients.
No permanent complications (hypoparathyroidism, paralysis of the recurrent nerve) were documented in the study patients.
Pathological examinations
As published previously (25), the removed thyroid glands and all lymph node specimens were submitted to pathological examinations. The surgeon provided the pathologist with the CT levels before starting histological examinations, thus serving to look more carefully for C-cell abnormalities (25).
C-cell hyperplasia (CCH) was considered when at least one area with >50 C-cells per one low power field ( × 100) was found in both thyroid lobes.
CCH was morphologically classified as focal, diffuse, nodular (summarized as “physiological”), or neoplastic CCH (30,31).
MTC was diagnosed if a focal loss or reduplication of the basement membrane was observed upon immunohistochemistry (32).
The tumors were classified in accordance with the Union for International Cancer Control (UICC) 2010 (6,33).
Molecular genetic analysis
The presence of germline mutations was tested in all patients by screening exons 5, 8, 10, 11, 13, 14, 15, and 16 of the rearranged during transfection (RET) proto-oncogene (34). Corresponding to the study protocol, the first patient diagnosed with MTC in a family with a germline mutation (“index patient”) was not excluded from further analysis.
Postoperative follow-up
All patients were followed clinically and biochemically. bCT and Ca-sCT levels were determined at 6 weeks, 6 and 12 months, and then bCT once a year after surgery. The patients appeared to be cured when both bCT and Ca-sCT levels remained <10 pg/mL 12 months after surgery. Persistently high bCT and/or Ca-sCT levels were referred to as “persistent” disease. Elevated bCT levels 12 months after previous normalization were defined as “recurrent” disease.
Statistical methods
The sensitivity, specificity, positive predictive value, and negative predictive value of the bCT and Ca-sCT cutoff values to predict MTC were calculated. The cutoff values to predict lateral compartment lymph node metastasis were defined by receiver-operating characteristic curves describing the area under the ROC curve (AUC), confidence intervals, and p values for males and females.
Subsequently, the documented sex-specific thresholds of bCT and Ca-sCT levels were used to evaluate whether bCT or Ca-sCT alone or in combination may improve the prediction of MTC and whether bCT or sCT may also predict positive lateral lymph nodes as the basis for planning the extent of surgery.
All calculations were done with SPSS Statistics (Version 23.0, IBM Corp. Released 2015. IBM SPSS Statistics for Windows; IBM Corp., Armonk, NY) version 23 for Windows and Microsoft Excel 16 for Windows.
Results
Baseline characteristics
All relevant demographic details of the study are summarized in Table 1.
Demographic, Clinical, and Pathological Details of the Study Population
Local tumor stage according to UICC 2010 [1, 26]—pT1a, ≤10 mm; pT1b, 11–20 mm; pT2, 21–40 mm; pT3, tumor >4 cm in greatest dimension limited to the thyroid or tumor of any size with minimal extrathyroid extension beyond the thyroid capsule; pT4, advanced or very advanced disease; N1, lymph node metastasis; N1a, central lymph node metastasis; N1b, lateral lymph node metastasis; M1, distant metastasis; germline RET mutation, germline mutation in the RET proto-oncogene; MLNR, ratio between number of metastatic nodes and total number of lymph nodes removed.
Percentile (25–75).
CCH, C-cell hyperplasia; FTC, follicular thyroid cancer; MTC, medullary thyroid cancer; PTC, papillary thyroid cancer; RET, rearranged during transfection.
In the study period, 149 patients (males: 79; females: 70) had an operation for elevated bCT and Ca-sCT levels.
MTC was diagnosed in 76/149 patients (males: 40/79 [50.6%]; females: 36/70 [51.4%]). The tumors were classified as pT1a in 48/76 patients (63.2%), pT1b in 16/76 (21.1%), pT2 in 6/76 (7.9%) and pT3 in 6/76 (7.9%) patients. No patient was diagnosed with a pT4 tumor.
The median tumor size was 5 mm (1–17 mm) in male patients and 9 mm (5–15 mm) in female patients. Bilateral tumors were found in 12 patients (15.8%) and tumors were multifocal in one thyroid lobe in another 4 patients (5.3%).
Lymph node metastases were diagnosed in 21/79 (26.6%) patients (males: 12/40 [27.6%]; females: 9/36 [25%]). Four patients had pN1a (central compartment only) disease and 17 had pN1b disease (lateral compartment with/without central compartment). On average, 126 (interquartile range [IQR] 78–147; absolute range: 8–177) lymph nodes were dissected. Among patients in whom lymph node metastasis were found, a median of 12 (IQR 2–26; absolute range: 1–53) lymph nodes were affected. The metastatic lymph node ratio (ratio between the number of metastatic lymph nodes and number of total removed lymph nodes) was 0.095.
At the time of diagnosis, distant metastases were documented radiologically (rM1) in 4/76 (5.3%) patients (males: 3/40 [57.5%]; females: 1/36 [2.8%]). Two patients had metastases to the liver, one to the brain and another patient had multiple metastases to the lung, liver, and bones.
In patients without MTC (overall: 73/149 [48.9%]—males: 39/79 [49.4%]; females: 34/70 [48.5%]), CCH was diagnosed after immunohistochemical workup.
CCH was classified as physiological in 37/73 patients (50.7%) and as neoplastic in 36/73 patients (49.3%), respectively.
Additional follicular cell-derived thyroid cancer was found in 44/149 patients (29.5%).
Histologically, and apart from nodules of various sizes, the pathologist described diffuse parenchymal infiltrations by lymphocytes (by definition chronic lymphocytic thyroiditis) in 31/149 patients (20.8%; males: 13/79 [MTC: 4, CCH: 9]; females: 19/70 [MTC: 9; CCH: 10]).
Germline RET mutations were documented in 8/76 patients (10.5%) with MTC (males: 4/40 [10.0%]; females: 4/36 [11.1%]) and in 2/73 (11.1%) with CCH (males: 1/39 [2.6%]; females: 1/34 [2.9%]).
Sex-specific basal and calcium-stimulated CT values to predict medullary thyroid cancer
As presented recently, cutoff levels for male and female patients were different for predicting MTC (Table 2).
Sex-Specific bCT and Ca-sCT Levels
AUC, sensitivity–specificity, positive, and negative values to predict MTC (with/without lymph node metastasis) and lymph nodes metastasis in the lateral neck. CT assay: Siemens Immulite.
AUC, area under the ROC curve; bCT, basal calcitonin level; Ca-sCT, calcium-stimulated CT levels; CT, calcitonin; N, lymph node; NPV, negative predictive value; N0, no lymph node metastasis; N1a, lymph node metastasis in the central neck along the recurrent laryngeal nerves; N1b, lymph node metastasis in the lateral neck; PPV, positive predictive value.
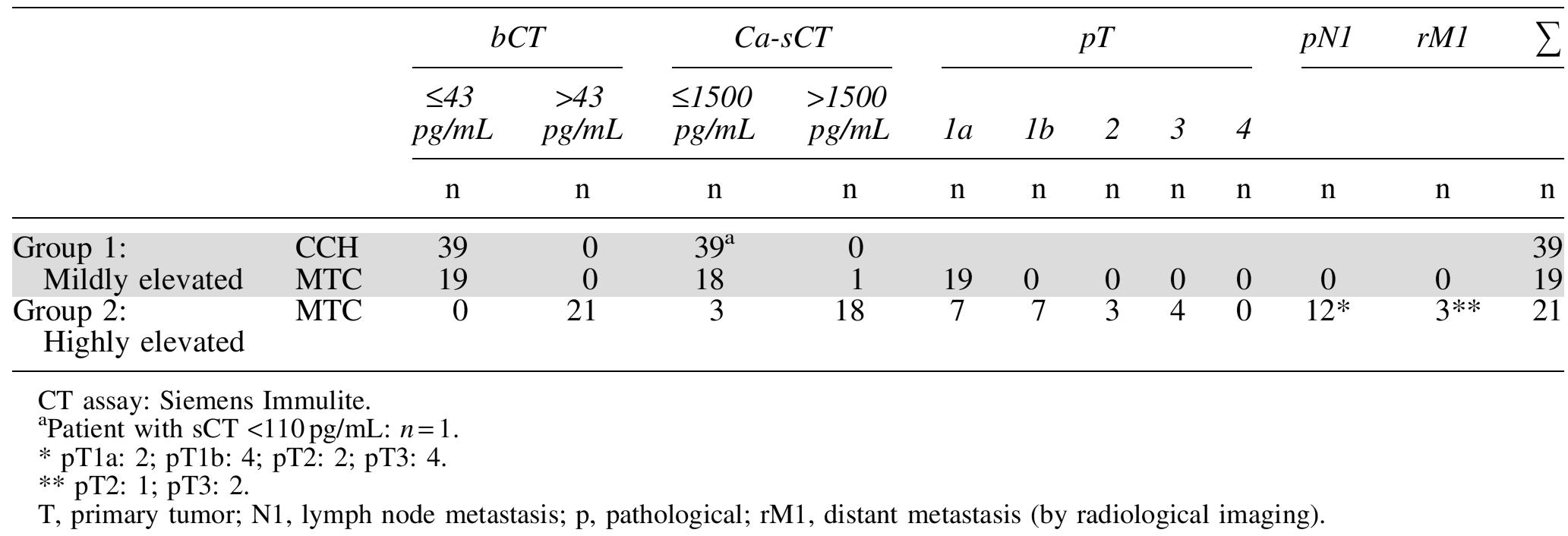
Applying the predefined cutoff levels (1) for males with bCT levels >43 pg/mL or Ca-sCT >1500 pg/mL and for females with bCT levels >23 pg/mL or Ca-sCT >780 pg/mL the patients could effectively be subdivided into two groups: Whereas MTC was detected in 100% (group 2; MTC only; no false-positive patients) of the patients with CT levels above the sex-specific cutoffs, there was a relevant overlap of patients with MTC or with CCH among those with bCT or Ca-sCT levels below the cutoffs (group 1; mildly elevated).
In group 1, all patients with MTC (males: n = 19; females: n = 7) were classified as pT1a (tumor diameter ≤10 mm). Only one female but no male patient was diagnosed with a lymph node metastasis in the central compartment. No lymph node metastases in the lateral compartment or distant metastases were found within this group (Tables 3 and 4).
C-Cell Morphology, TNM Classification, and Comparison of Basal Calcitonin and Calcium-Stimulated Calcitonin Cutoffs in Male Patients (n = 79)
C-Cell Morphology, TNM Classification, and Comparison of Basal Calcitonin and Calcium-Stimulated Calcitonin Cutoffs in Female Patients (n = 70)
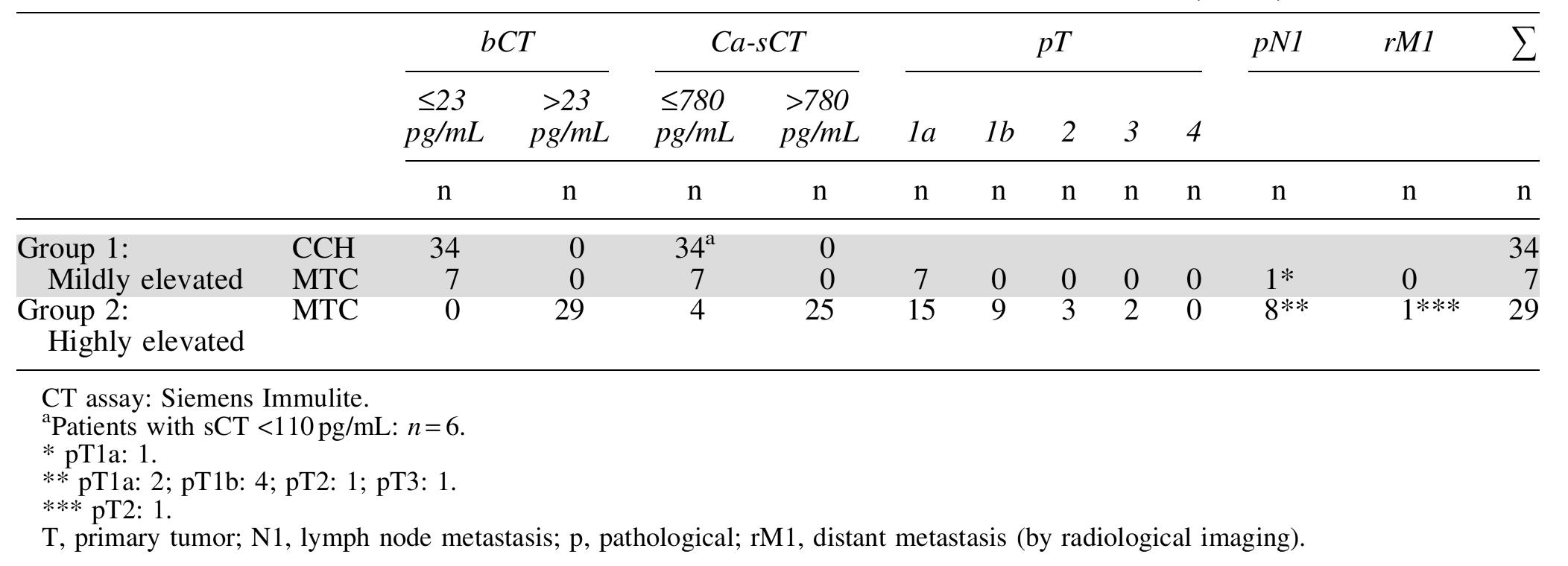
In group 2 (Tables 3 and 4), MTC was classified as pT1 in 38/50 (76%) patients, as pT2 in 6/50 (12.0%) and as pT3 in 6/50 (12.0%) patients. Lymph node metastasis (pN1a 3/50 [6.0%], pN1b 17/50 [34.0%]) were present in 20/50 (40.0%), (Table 5) and distant metastasis in 4/50 (8.0%).
Lymph Node Metastasis in the Lateral Compartment (N1b) and Basal Calcitonin Cutoff Values and Follow-Up
CT assay: Siemens Immulite.
Follow-up (median follow-up: 46 [ ± 27] months).
Lost to follow-up: n = 1.
N0, no lymph node metastasis; N1a, lymph node metastasis in the central neck along the recurrent laryngeal nerves; N1b, lymph node metastasis in the lateral neck.
Comparing the value of bCT and calcium-stimulated CT alone or in combination for predicting medullary thyroid cancer
Overall, the potentials of both bCT and Ca-sCT to predict the presence of MTC expressed as AUC were excellent (35). However, in both male and female patients, determination of bCT alone showed a slightly better test performance than CT stimulated by Ca (males: 0.894 vs. 0.849; females: 0.935 vs. 0.868; Table 2). Whereas in males the sensitivity was only 5% higher for bCT measurement (53% vs. 48%; specificity 100% for both), the difference in sensitivity was higher for females (81% vs. 69%; specificity 100% for both). Therefore, 7 more patients (males: 3; females: 4) were correctly classified (definitive MTC) by using bCT compared with Ca-sCT (Tables 3 and 4).
However, based on the observation that no patient with Ca-sCT levels <110 pg/mL was diagnosed with MTC, MTC could be ruled out in seven patients using this cutoff (males: 1; females: 6).
When combining the results of bCT and Ca-sCT, the definitive diagnosis of MTC failed to be improved: Only one male patient was diagnosed with definitive MTC using Ca-sCT (>1500 pg/mL) but had bCT levels lower than the cutoff of 43 pg/mL. Hence, sensitivity improved from 53% to 55% for the combination of bCT and Ca-sCT in male patients only, it did not change in female patients.
Comparing the value of bCT or calcium-stimulated CT for the prediction of lymph node metastasis
In both males and females, the AUC were higher for bCT levels than for Ca-sCT levels in the diagnosis of both pN1a and/or pN1b lymph node metastasis (Table 2).
All male patients with lymph node metastases had bCT levels ≥100 pg/mL (Table 5; sensitivity: 100%). The specificity for the diagnosis of any lymph node metastases (pN1a or pN1b) was 82% and for the presence of lateral lymph node metastases (pN1b only) was 74% (Table 2).
In women, one patient was diagnosed with a single lymph node metastasis in the central compartment (N1a) with a bCT level of 23 pg/mL. Therefore, the cutoff of ≥23 pg/mL was used to diagnose any lymph node metastases (pN1a or pN1b) and the specificity was only 22% with a sensitivity of 100%. However, all other women (n = 8) with lymph node metastases had bCT levels ≥85 pg/mL and metastasis in the lateral compartment (Tables 2 and 5; specificity: 57%).
Follow-up
By definition, surgery served to clinically and biochemically cure 31/39 males (79.5%; lost to follow-up: n = 1) and 32/36 females (88.9%). Within the follow-up period of 46 [ ± 27] months, clinically or biochemically recurrent disease was documented in none of the initially cured patients. All patients in group 1 (mildly elevated) and all patients not predicted to have lymph node metastasis in the lateral neck compartment were cured (Table 5). Overall, persistent disease was documented in 9/76 patients (11.8%; all in group 2 and initially with positive lymph nodes). Three of 76 patients (3.9%) (males: 2; females: 1; all with distant metastasis at the time of diagnosis) died 19, 35, and 65 months after surgery of persistent MTC.
According to the TNM staging and by definition, all stage I (n = 51), stage II (n = 3), and stage III (n = 6) patients, and 2/12 stage IVA (16.7%) patients were cured by surgery.
Persistent disease was identified in 9/12 stage IVA (75%) and 2/4 stage IVC patients (50%). One stage IVA and two stage IVC patients died of their disease.
Discussion
There is an ongoing discussion with regard to the value of routine serum CT screening for MTC in the preoperative workup of thyroid nodules. Since surgical treatment for even small MTC must be more aggressive compared with other types of thyroid cancer, the preoperatively definitive (early) diagnosis of MTC significantly influences management (7).
However, elevated bCT levels must always be questioned and reasons for non C-cell-derived CT elevations or the rare cases of false-positive results due to heterophilic antibodies are to be excluded (2).
Especially in the absence of thyroid nodules on ultrasound (no indication per se to determine CT), or if there is a discrepancy between the size of a thyroid nodule and bCT level (a small nodule and an inadequately high bCT level), stimulation tests may help to differentiate thyroid from nonthyroid sources of CT production (3 –5).
Ectopic CT production by neuroendocrine tumors has to be taken into account, characterized by no or a less than twofold increase in CT levels after stimulation. When stimulation exceeds bCT by more than twofold, MTC is found exclusively (3).
As it may occasionally be difficult to interpret and draw conclusions regarding reproducible elevated CT levels, various authors (36,37) have discussed that if cutoff levels based on Ca stimulation testing would become well validated, CT screening would likely become more widely accepted in the diagnostic workup for thyroid nodules.
After excluding non-C-cell-derived CT elevations (2), the recommendation for further diagnosis or treatment of patients with elevated CT values is to be based on the CT assay used, the given patient's sex, and the absolute CT levels.
Up to now, there are no globally accepted CT cutoff levels to predict MTC, as different CT assays are used in different laboratories. The normal range of bCT and Ca-sCT levels may vary from laboratory to laboratory and from assay to assay. Each institution has to define its own bCT and Ca-sCT cutoff labels to discriminate CCH/intrathyroid micro-MTC from larger tumors that may be associated with lymph node metastases. For serial measurements of CT, it is recommended to use the same laboratory with its established reference ranges (37).
Without specifying the characteristics of the CT assay, concentrations between 60 and 100 pg/mL have been assessed as highly suggestive/pathognomonic of MTC in recently published guidelines (10).
Applying different assays makes it difficult to interpret published results, impossible to compare data and cutoff values, and hard to follow recommendations to guide surgery (21). In one recently published article (38), four different assays based on three assay types were used for CT measurement. Costante et al. (39) applied only one single assay (Nichols Advantage [ICMA]) but did not offer sex-specific cutoffs. Studies should be compared with respect to both assay characteristics and well-known sex differences in bCT levels, which are physiologically higher in males than in females (24,40).
The Nichols and Siemens DPC assay and recently, also the Siemens DPC and the Roche Cobas assay have been demonstrated to show an almost perfect linear correlation (21,22,41), and CT levels from one assay can thus easily be converted to another. In this study, one of the widely used highly sensitive ICMA (DPC Siemens Immulite 2000) for CT was applied. Clear sex-specific cutoff levels to prognosticate MTC preoperatively have recently been published for this assay (1).
Based on the greatest accuracy at the lowest possible bCT level, MTC was predicted in all males with bCT levels >43 pg/mL or Ca-sCT >1500 pg/mL and in all females with bCT levels >23 or >780 pg/mL after Ca stimulation (no false-positive). In this CT screening program, more females were assigned preoperatively to the patients' group with highly elevated bCT levels. MTC was thus correctly predicted in more females (41.4%) than males (26.6%; trend; p = 0.055; chi-square) (1). This is in accordance with recently published data by Chambon et al. (42).
Using the same diagnostic standards, Colombo et al. (15) and Mian et al. (13) (in a lower number of more inhomogeneous patients and without a prospective treatment protocol) showed that the best levels of bCT to separate normal and CCH cases from MTC patients were >18.7 pg/mL (15) and, more precisely, >26 pg/mL (13) in females and >68 pg/mL (13,15) in males. Furthermore, Ca-sCT levels >79 pg/mL (13) and, more precisely, >184 pg/mL (15) in females and >544 pg/mL (13) and, more precisely, >1620 pg/mL (15) in males were shown to yield the highest accuracy to distinguish normal and CCH cases from patients with MTC. However, CCH and MTC could not be discriminated below the published cutoff levels (patients with “mildly elevated” bCT levels) (13).
Patients with bCT levels above the presented cutoffs (highly elevated bCT levels in the Siemens Immulite assay) are likely to have MTC (no false-positive patients in the study) and, therefore, should be offered an operation.
The findings of routinely applied neck ultrasound were not incorporated in the surgical decision-making because of previous findings (23) that neck ultrasound revealed an overall sensitivity of only 90% in detecting MTC with a mean tumor size of 20 mm and larger. As shown recently, in the subgroup of patients with pT1a tumors, the sensitivity was even lower (71%) (26).
In this study, 63.2% of patients were diagnosed with pT1a tumors. Overall median tumor size was 7 mm (IQR 2–16 mm), for pT1a tumors only 3 mm (IQR 1–6 mm). Without determination of bCT levels most of these thyroid nodules and as a consequence MTC would not have been treated because of their small size. In addition, the majority of tumors ≤10 mm would not be indicated to have FNAB. Small nodules are difficult or impossible to examine by FNAB. The evaluation of bCT was shown to be superior as compared with FNAB, especially in diagnosing small (≤10 mm) curable MTC (43 –47). Boi et al. (27) were the first to recommend CT measurements in wash-out fluids from fine needle aspiration to improve the diagnosis in primary (and metastatic) MTC in the workup of thyroid nodules and to prevent unnecessary surgery. However, even this modification of fine needle aspiration evaluation may be inconclusive or hardly possible because of the small tumor sizes (48).
Lastly, the sensitivity of ultrasound to diagnose lymph node metastasis was only 43% overall and 6% and 56% in the central and lateral neck, respectively (26).
The Ca-sCT compared with the bCT (or the combination of both) did not improve the accuracy for detecting MTC in females in this study. Only in one additional male patient, MTC was predicted correctly by also considering the Ca-sCT level in interpreting the biochemical results.
As tumor volume correlates with bCT levels (49,50), the extent of initial surgery should be adapted to preoperative CT levels (51). In this study, lymph node and distant metastases were documented in 57.1% and 14.3% of male and in 27.9% and 3.4% of female patients with highly elevated CT levels.
Knowledge of bCT levels in patients with thyroid nodules facilitates a tailored surgical strategy. Besides total thyroidectomy and central neck lymph node dissection, the indication for lateral neck dissection at initial surgery may be individualized. Based on the current analysis, it is recommended only in male patients with bCT levels ≥100 pg/mL and in females with bCT levels ≥85 pg/mL as an additional procedure during initial surgical strategy, since in this group, lateral lymph node metastases were detected in 52.9% males and 40.0% females.
In 41/70 (58.6%) females and 58/79 (73.4%) males, the bCT levels were documented below the “high risk” cutoff CT, which strongly suggest MTC. In these patients with mildly elevated bCT levels, there was an indistinct overlap between CCH and microMTC (gray zone) (1) and bCT levels did not seem sufficiently specific to assess the diagnosis of MTC. This is why stimulation tests have been recommended in the literature (11,12,39,52).
To our knowledge, this study is the first analysis to prospectively investigate the possible value of Ca stimulation tests in patients with “mildly elevated” bCT to better discriminate CCH and MTC. However, CT stimulation failed to improve diagnostic accuracy, as within the gray zone, neither bCT nor Ca-sCT levels (or the combination of both) were able to discriminate between CCH and MTC in either sex.
The goal of surgical treatment is to perform thyroidectomy before MTC develops or while it is still confined to the gland in an attempt to prevent persistence and recurrent disease and to improve cure rates. Respecting the sex-specific cutoff levels, in patients with mildly elevated bCT values (gray zone), the final histological examination of the thyroid gland and the central lymph nodes revealed MTC in more males (19/59 [32.2%]) than in females (7/41 [17.1%]). All MTC in males and females of this group were classified as pT1. While all tumors in 19 males were staged pN0, central lymph node metastases (pN1a) were documented in 1/7 females. However, total thyroidectomy and bilateral central neck dissection served to cure all individuals biochemically.
Frank-Raue et al. (53) recommended to re-evaluate patients with lower bCT values in intervals of 3–6 months and advise surgery in patients only with rising CT levels, which may indicate MTC. However, there is limited clinical experience using this approach. There is only one series of 171 patients who were followed for 2–4 years and in 170 of those basal levels remained <20 pg/mL [applying the ICMA assay by Nichols Advantage, corresponding to 16 pg/mL with the ICMA CT assay by Diagnostic Products Corporation (22)]. Only one man experienced an increase (to 33 [26] pg/mL) after 2 years of follow-up. He underwent a stimulation test (with pentagastrin) with positive results and a peak level of 317 (254) pg/mL. Surgery demonstrated the presence of CCH only (39).
Many patients are aware that CT is a sensitive tumor marker for MTC. Reproducible mildly elevated bCT levels may be the first sign of MTC in those presenting with thyroid nodules ≤10 mm. With regard to the psychological burden of this knowledge, keeping some patients in persistent anxiety and uncertainty, many patients request for an operation even after having been informed about the minor long-term consequences of mildly elevated bCT. Potential morbidity must be carefully discussed with the patients and be balanced against unnecessary thyroid surgery and continuous follow-up.
In experienced surgical teams, patients who decide for surgery may be treated early by total thyroidectomy and bilateral central neck dissection, which is mandatory because micrometastasis may also be present in patients with mildly elevated bCT levels, as seen in one female patient.
Nevertheless, a restricted indication for surgery may theoretically exist in women, as MTC was found in <20% of the female patients. A more liberal indication for surgery should be considered in men, as MTC was found on histology in at least 1/3 males.
The Ca stimulation test may only be helpful to subclassify patients with mildly elevated bCT, who are definitively not candidates for surgery:
In a previous investigation (cited by many following studies), surgery was recommended in all subjects with an abnormal CT response (to pentagastrin) >100 pg/mL. This was because peak CT levels exceeding 100 pg/mL were considered to be indicative of MTC and MTC was definitively documented in many patients (20). Costante et al. (39) also reported that stimulated CT values after pentagastrin infusion of >100 pg/mL predicted MTC in at least 40%. Performing a Ca stimulation test in this study, females and males with Ca-sCT levels ≤110 had various types of CCH on immunohistochemistry, but no MTC was found. Therefore, one may conclude that these patients are not candidates for surgery.
In conclusion, neither Ca-sCT alone nor the combination of bCT and Ca-sCT as compared with bCT help to further improve the diagnosis of MTC in patients with highly elevated CT levels (above predefined cutoffs) or to differentiate between patients with CCH and micro-MTC in those with only mildly elevated CT levels (below predefined cutoffs).
Knowledge of bCT levels alone facilitates a “tailored” surgical strategy in the central and lateral neck in patients with thyroid nodules. Total thyroidectomy and central neck dissection are the treatments of choice for initial surgery, as lymph node metastases in the central compartment can be found even at low (mildly elevated) CT levels.
Analyzing the prospectively acquired data based on a broadly applied highly sensitive CT assay (DPC Siemens Immulite 2000), the cutoff bCT levels for lateral neck lymph node metastasis were ≥100 pg/mL in males and ≥85 pg/mL in females. sCT was not superior in predicting lymph node metastasis and, therefore, should not influence the extent of surgery. According to these results, lateral neck dissection seems to be indicated in patients with bCT levels above these cutoffs as lymph node metastases in the lateral compartment were found in 52.9% of males and 40.0% of females.
After critically excluding the rare cases of other sources of CT elevation in the workup of thyroid nodules, surgery is definitively indicated in patients with highly elevated bCT levels. Surveillance with periodical bCT measurements seems justified in compliant patients with only mildly elevated bCT levels. In anxious patients and in those who refuse biochemical follow-up, early total thyroidectomy and bilateral central neck dissection can be considered.
Disclaimer
This article is not based on a previous communication to a society or a meeting.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.