
Abstract
The thyrotropin receptor (TSHR) mutation database, consisting of all known TSHR mutations and their clinical characterizations, was established in 1999. The database contents are updated here with the same website (
Introduction
The thyrotropin receptor (TSHR) is a G-protein coupled receptor with two major pathways. The Gs pathway is primarily responsible for thyrocyte proliferation while also affecting thyroid hormone (TH) synthesis. The Gq/11 pathway plays a role in iodination and TH synthesis (1). Mutations leading to constitutive activation or inactivation of the TSHR through either or both of these pathways can lead to thyroid disorders. Constitutively activating germline mutations lead to familial nonautoimmune autosomal dominant hyperthyroidism (FNAH), or sporadic congenital nonautoimmune hyperthyroidism (SNAH) (2). Somatic mutations have been found in up to 84% of single toxic thyroid nodules as well as in toxic multinodular goiters (3 –7). The prevalence of inactivating TSHR mutations has been reported with much variability. Inactivating familial or sporadic TSHR mutations were reported in 13.7% Japanese patients with congenital hypothyroidism: 4.3% with biallelic mutations and 9.4% with monoallelic mutations (8), whereas a population-based Italian study found 1 of 16 (6.3%) and a Finnish study found 2 of 26 (7.7%) congenital hypothyroidism patients to have monoallelic TSHR mutation (9,10). Mutations have also been found in patients with uncommon conditions such as hyperfunctioning thyroid carcinomas (11 –24) and gestational thyrotoxicosis, a transient form of thyrotoxicosis during pregnancy due to a mutant thyrotropin receptor hypersensitive to human chorionic gonadotropin (25).
The TSHR mutation database, established in 1999, documents the clinical findings of patients with TSHR mutations and the functional characterization, the degree to which TSHR mutations activate or inactivate the TSHR (26). The database has been updated in 2003 (27) and in 2012 (28). During the current update, finalized in August 2019, the database was relocated to a University of Calgary server. Its website remains the same (
Additions to the Database
Eight years after the last update, the current database now contains all clinically occurring TSHR mutations published up to August 2019. New entries for 35 novel mutations (7 activating and 28 inactivating) and 72 new cases for previously described mutations (41 activating and 31 inactivating) were added to the TSHR mutation database. A total of 107 new entries were subdivided into 4 categories: Constitutively activating TSHR germline mutations: 5 novel mutations and 12 new cases of previously described mutations Constitutively activating somatic TSHR mutations: 2 novel mutations and 25 cases of previously described mutations Constitutively activating somatic TSHR mutations in hyperfunctioning thyroid carcinomas: 4 cases of previously described somatic gain of function mutations in hyperfunctioning thyroid carcinomas Inactivating TSHR germline mutations: 28 novel mutations and 31 new cases of previously described inactivating TSHR germline mutations.
It is important to note that 28 novel mutations added to the database have not been functionally characterized, this is indicated in each mutation's preview accessed from the list page (
Constitutively activating mutations are generally found in the transmembrane domains, with a disproportionate number found in the sixth transmembrane domain. These are generally point mutations with the exception of three constitutively activating deletion mutants (33 –35). Inactivating mutations are found throughout the receptor and more commonly include deletions, insertions, truncation, and splicing (8,36 –49).
Geographic Origin of Reported Mutations
The previous database had 200,000 hits worldwide since its debut in 1999. Currently, there is a dearth and an under-representation of North American patients with TSHR mutations in this database. Interestingly, much of the data in the TSHR mutation database come from studies in Europe. Asia (particularly Japan) is the second most active continent with published clinical reports on TSHR mutations (Figs. 1 and 2). These data are probably subject to ascertainment bias; however, it is of interest to see which countries are presently screening for TSHR mutations. Interestingly, some mutations have been reported across different continents (North America, Europe, and Asia). There are 14 activating germline mutations described more than once, 6 of these occur only within a single continent (4 in Europe and 2 in Asia), the further 8 mutations have been described in multiple continents (Table 1). Certain inactivating germline mutations referenced in the database have a higher incidence in particular countries or continents, for example, R450H has been described 20 times: 16 of which were in Japan with 3 further incidences in Italy, and 1 in China, whereas P162A has been described 22 times: 16 in Italy, 4 elsewhere in Europe, 1 in the United States, and 1 in Thailand.
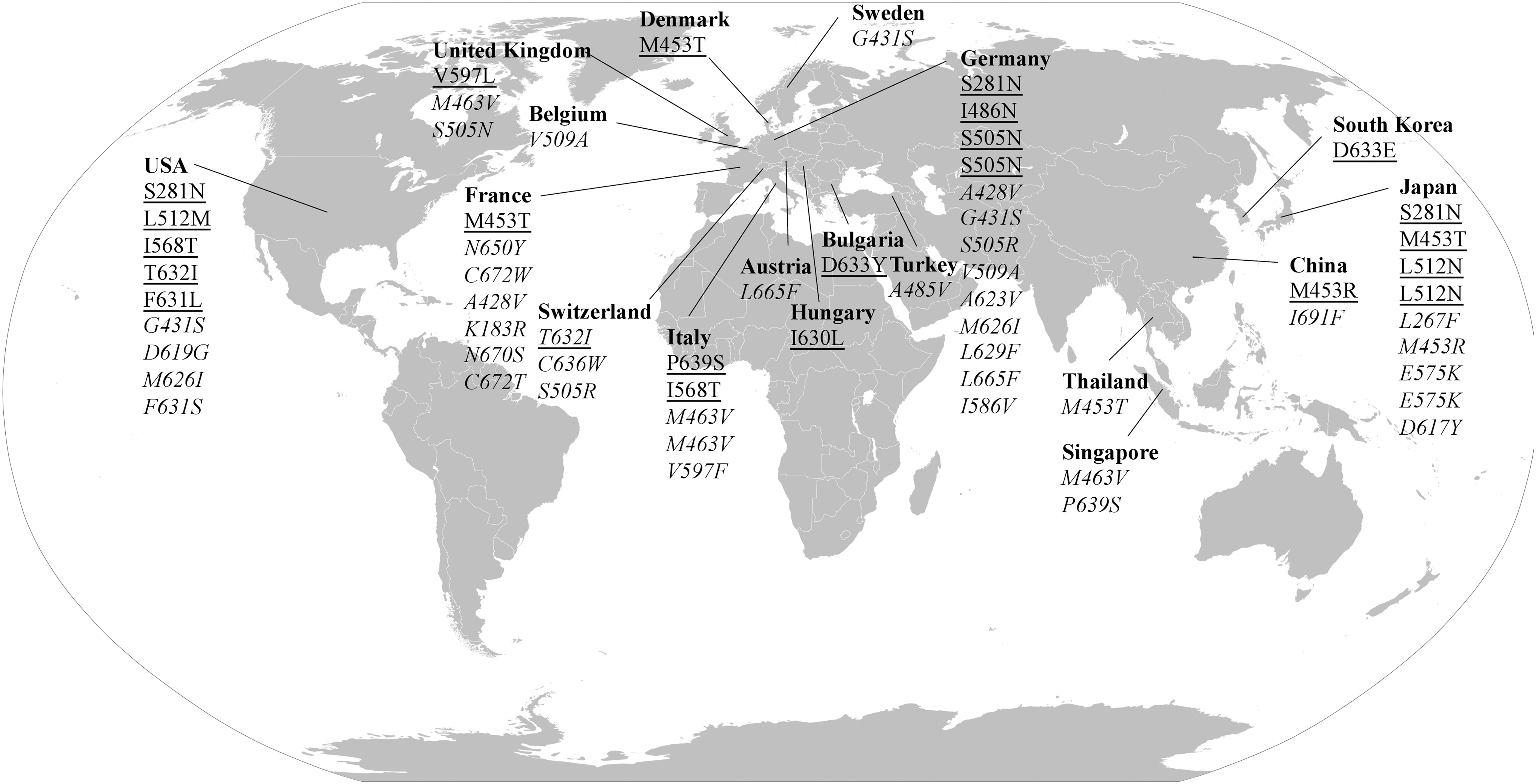
Location of clinician authors caring for respective patients for published cases of activating TSHR germline mutations where there are 39 familial (italics) and 23 sporadic (underlined) cases of activating germline mutations detected thus far. TSHR, thyrotropin receptor.
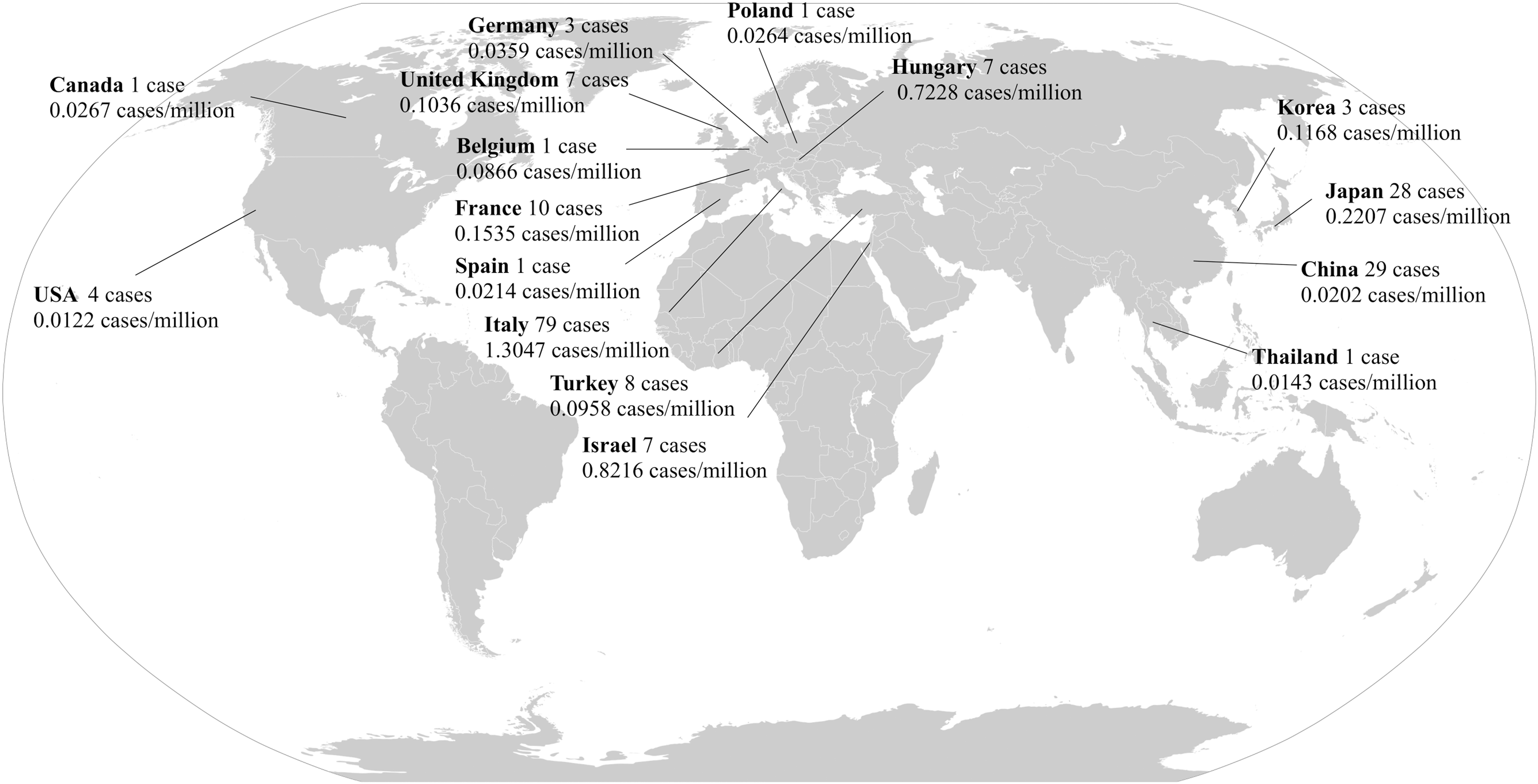
Estimated number of published cases and cases per million of inactivating germline TSHR mutations based on location of clinician authors caring for respective patients. Population statistics from 2019 Revision of World Population Prospects by United Nations Population Division.
Countries of Origin for Patients with Constitutively Activating Germline Mutations That Have Been Described More Than Once
Mutations Described in Thyroid Carcinoma
In this update, we have included a new category for TSHR mutations described in cases of hyperfunctioning thyroid carcinoma. The following mutations have been described in cases of thyroid carcinoma presenting as a hot thyroid nodule: I486P (15,16), M453T (12 –14), L512R (17), I568T (18), T620I (19), A623S (20), F631I (21), T632A (22), T632I (22,23), D633H (24), D33Y (21), and L677V (11). Clarification whether these mutations could contribute to the development of thyroid carcinoma requires further comprehensive genetic analysis of the published TSHR mutation positive carcinomas along with further cases of thyroid carcinoma presenting as a hot thyroid nodules without mutational analysis. The cases described in our database highlight the need for further investigation of the role of TSHR in thyroid carcinoma, especially considering that the increased malignancy risk for TSHR mutation positive hot nodules in children does not appear to be associated with most frequent mutations such as RAS, BRAF, PAX8/PPARG, and RET/PTC mutations (23).
Webpage Changes
While the functionality of the website remains mostly unchanged, new additions include a summary homepage, and an updated prevalence page (
To speed up database access, we have built a website using LAMP technology (Linux, Apache MySQL, and PHP), one of the most popular and fastest ways to generate web pages. The TSHR mutation database is installed as one of the locus-specific HUGO mutation databases (50) and can be accessed through (
Conclusions
New additions to the webpage include a summary and an updated prevalence page that accounts for mutations and/or cases published more than once. As of August 2019, there are 23 cases of SNAH, 39 families with FNAH, 18 cases of hyperfunctioning thyroid carcinomas, 130 families, and 60 sporadic individuals with hypothyroidism or TSH insensitivity with inactivating TSHR mutations. This database allows for rapid validation of patient TSHR mutations causing hyper- or hypothyroidism or insensitivity to TSH.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The revision of the database was supported by a grant from the Laura Linders research fund.