
Abstract
Background:
The association between isolated maternal hypothyroxinemia (IMH) during pregnancy and preterm birth (PTB), especially for subtypes of PTB, is unclear. This study aimed at determining the association between IMH diagnosed in early pregnancy and PTB, with further investigation into various subtypes of PTB.
Methods:
This study included 41,911 pregnant women (963 with IMH and 40,948 euthyroid women) who underwent first-trimester prenatal screening at the International Peace Maternity and Child Health Hospital (IPMCH) in Shanghai, China between January 2013 and December 2016. PTB was defined as birth before 37 weeks of gestation. PTB was further classified into three clinically relevant groups to investigate the clinical heterogeneity of PTB: (a) preterm birth with premature rupture of membranes (PROM-PTB); (b) spontaneous preterm birth with intact membranes (S-PTB); and (c) medically-induced preterm birth (MI-PTB). The overall and sex-specific effect of IMH on PTB and various subtypes of PTB were estimated by using logistic regression in crude and adjusted models.
Results:
Pregnant women with IMH had an increased risk of PTB (odds ratio [OR]: 1.32 [95% confidence interval; CI: 1.02–1.70], p = 0.03) compared with women with euthyroid function. The increased risk of PTB is mainly driven by S-PTB (OR: 1.57 [CI: 1.11–2.24], p = 0.01), while women with early pregnancy IMH had no statistically significant increased risk of PROM-PTB and MI-PTB. The effect of IMH on PTB was modified by fetal sex (p-values for interaction = 0.04). More prominent effects were observed in women carrying a female fetus, while no statistically significant effects were found in women carrying a male fetus.
Conclusions:
This study revealed that pregnant women with IMH in early pregnancy have a higher risk of PTB compared with euthyroid women. The effect of IMH on PTB is mainly driven by S-PTB and is modified by fetal sex.
Introduction
During pregnancy, maternal normal thyroid hormone levels play critical roles in fetal growth and development. Thyroid disease during pregnancy may lead to several pregnancy complications. Isolated maternal hypothyroxinemia (IMH) is a thyroid disease with a prevalence of 1–2% during pregnancy. According to recent American Thyroid Association (ATA) guidelines, IMH is defined as a normal maternal thyrotropin (TSH) level in conjunction with free thyroxine (fT4) in the lower 2.5th to 5th percentile of a given population (1). Compared with other types of thyroid function abnormality, there is a dearth of information on the effects of IMH. The etiology of IMH remains unclear and there is no consensus between guidelines regarding the clinical treatment strategy for pregnant women with IMH (2,3). To date, studies on the risk of pregnancy complications related to IMH are limited (1).
Preterm birth (PTB), as a relatively frequent pregnancy complication, is one of the leading causes of newborn mortality, and it is a risk factor for cognitive, metabolic, and cardiovascular disease in later life (4 –6). PTB is generally known as a complex syndrome induced by multiple mechanisms (7), with different etiologies and mechanisms behind each subtype of PTB. Studies on the potential association between IMH and PTB are limited, have methodological flaws, and generate conflicting results (8 –14). Only one study showed a positive correlation between IMH and PTB (9), while other studies found no association (8,10 –13). Some previous studies defined IMH by applying a reference range established within a relatively long pregnancy period (9,10), which potentially led to misclassification of IMH. Both fT4 and TSH change throughout pregnancy. In early pregnancy, due to an elevated level of human chorionic gonadotrophin, fT4 level transiently increases, which, in turn, suppresses TSH level. In late pregnancy, fT4 gradually returns to a low level. Due to these variations throughout the pregnancy, the ATA guidelines recommend using trimester-specific reference values of TSH and fT4 to diagnose IMH (1). Moreover, prior studies on this topic did not differentiate various subtypes of PTB.
Therefore, this study aimed at determining whether IMH was associated with a higher risk of PTB, with further investigation into specific subtypes of PTB.
Materials and Methods
Patient enrollment
This study was embedded in a large prospective study performed at the International Peace Maternity and Child Health Hospital (IPMCH), a large public hospital providing tertiary care in Shanghai, China. The project was approved by the Ethics Committee of IPMCH (No. GKLW2012-49). Eligible pregnant women were those who underwent the first-trimester antenatal screening at IPMCH. A total of 52,027 pregnant women were consecutively enrolled from January 1st, 2013 to December 31st, 2016. All participants signed written informed consent. Within the larger study, women who met the following criteria were included in this specific study: (a) fT4, TSH, and antithyroid peroxidase antibody (TPOAb) data were available and (b) those diagnosed with IMH or with normal thyroid function. A total of 45,370 pregnant women with normal thyroid hormone levels (euthyroid group) and 1166 pregnant women with IMH (IMH group) were included in this study. Further exclusion was performed for those women who (a) underwent in vitro fertilization; (b) had a twin pregnancy or miscarriage; (c) used medication known to interfere with the thyroid function before or after baseline measurements; or (d) had a history of thyroid disease. As a result, the final analysis included 963 pregnant women with IMH and 40,948 euthyroid pregnant women.
Data collection
Nurses, residents, and gynecologists prospectively collected all information during hospital visits. At the first clinical visit (9–13 weeks of pregnancy), maternal age, parity, last menstrual period (LMP), education level, and previous disease were collected via interviews. Prepregnancy body mass index (BMI) was calculated by using height measured by trained nurses in early pregnancy and self-reported weight before pregnancy. Gestational age was estimated based on the date of LMP and adjusted by the ultrasonography in early pregnancy. Fasting blood samples were drawn from the median cubital vein, and the serum was separated by centrifugation within 6 hours. TSH, fT4, and TPOAb concentrations were measured by using the Architect i2000 immunoassay (Abbott, Chicago, USA) according to the manufacturer's protocol. The intra- and inter-assay coefficients of variation ranged between 1.6% and 3.6% for TSH, was 1.9–4.0% for fT4, and was 10.0% for TPOAbs.
Diagnostic criteria
In this study, IMH was defined as TSH within the normal range (2.5th–97.5th percentile) but with fT4 < 2.5th percentile. The euthyroid group was defined as having both TSH and fT4 levels within the normal range (2.5th–97.5th percentile). The early pregnancy 2.5th–97.5th percentiles of fT4 and TSH are 11.7–19.7 pmol/L and 0.03–3.64 mU/L, respectively. The TPOAb level of >5.6 IU/mL was defined as positive.
PTB was defined as birth before 37 weeks of gestation. Very early preterm birth (VPTB) was defined as birth before 34 weeks of gestation. PTB was classified into spontaneous PTB and medically induced preterm birth (MI-PTB) according to clinical presentation, and spontaneous PTBs were further categorized as preterm birth with premature rupture of membranes (PROM-PTB) or spontaneous preterm birth with intact membranes (S-PTB). The classification criteria were as follows: (a) PROM-PTB was defined as PTB with spontaneous rupture of the membranes at less than 37 weeks of gestation and before the onset of contractions; (b) S-PTB was defined as spontaneous PTB with intact membranes; and (c) MI-PTB was defined as PTB after labor induction or cesarean delivery for maternal or fetal indications (15).
Statistical analyses
Differences in the distributions of maternal characteristics between the euthyroid and IMH groups were assessed by using Chi-squared test for categorical variables and Mann–Whitney U test for continuous variables. Logistic regressions were performed to calculate crude and adjusted odds ratios (ORs) and 95% confidence intervals (CIs). We also studied whether the sex of the fetus modifies the effect of IMH on PTB on a multiplicative scale by adding the product interaction term IMH × fetus to the logistic regression models. Potential confounders included maternal age, BMI, parity, education level, fetal sex, and TPOAb status. The selection of potential confounders was based on biological plausibility, identification of a variable as a confounder in previous studies, changes of the effect estimates of interest, or reduction in the residual variability of the outcome.
For the missing variable maternal BMI (missing in 1.5% of the study participants), multiple imputation according to the Markov chain Monte Carlo method was used by creating and pooling five imputed datasets for analyses based on “missing at random” assumption (16). We added variables without missing data (maternal age, gestational age, education level, parity, fetal sex, TSH, fT4, and TPOAb concentrations) to the model as prediction variables. No significant differences in descriptive characteristics were found between the original and imputed datasets. To test the robustness of our findings under different definitions of IMH, sensitivity analysis was performed by using the 5th percentile as the cut-off value for fT4 and TSH within the normal range (2.5th–97.5th percentile) to define IMH in pregnant women.
All statistical analyses were performed by using R Statistical Software version 3.4.1 (package rms, mice) or Statistical Package for the Social Sciences v20.0 for Windows (SPSS v22.0; IBM Corp, Armonk, NY). All statistical tests were performed by using a two-sided p < 0.05 as the level of statistical significance, except for the interaction terms, where we considered statistical significance at an alpha level of 0.10.
Results
Baseline characteristics
After exclusions, 963 pregnant women in the IMH group and 40,948 pregnant women in the euthyroid group remained in the final study population (Fig. 1). Compared with the included 963 untreated pregnant women with IMH, the excluded 36 pregnant women with IMH treated with levothyroxine (LT4) after baseline measurements had no statistically significant difference in PTB rate (Supplementary Table S1).

Flow chart of the study population. The IMH was defined as TSH within normal range (2.5th–97.5th percentile) but with fT4 < 2.5th percentile. fT4, free thyroxine; IMH, isolated maternal hypothyroxinemia; IVF, in vitro fertilization; TSH, thyrotropin.
The characteristics of the women in both groups are shown in Table 1. The IMH group had a median (interquartile range) age of 32 (29–34) years, which was higher than the age in the euthyroid group with a median (interquartile range) age of 30 (27–32) (p < 0.001). The IMH group had a higher median BMI than the euthyroid group (22.0 [20.3–23.9] vs. 20.6 [19.1, 22.4]; p < 0.001) kg/m2. Pregnant women with IMH had a higher level of education than the women in the euthyroid group. The proportion of women positive for TPOAb and gestational diabetes mellitus (GDM) was higher than that in the IMH group. The proportion of primipara in the euthyroid group was higher than that in the IMH group. The distribution of fetal sex was similar in the two groups.
Comparison of the Demographic Characteristics Between Isolated Maternal Hypothyroxinemia Group and Euthyroid Group
BMI, body mass index; GDM, gestational diabetes mellitus; IMH, isolated maternal hypothyroxinemia; TPOAb, antithyroid peroxidase antibody.
IMH in early pregnancy and risk of PTB, VPTB
As shown in Table 1, women with IMH had a higher rate of PTB (7.0% vs. 4.8%) and VPTB (1.6% vs. 0.8%) compared with euthyroid women (p < 0.01). As shown in Table 2, in crude unadjusted analyses, those with IMH had an increased risk of PTB (OR: 1.49 [CI 1.16–1.92], p < 0.01) and VPTB (OR: 2.05 [CI 1.22–3.46], p < 0.01) compared with euthyroid pregnant women. After adjusting for maternal age, BMI, parity, education level, fetal sex, TPOAb status, and GDM, the higher PTB risk remained statistically significant (OR: 1.32 [CI 1.02–1.70], p = 0.04), but the higher VPTB risk did not reach statistical significance (OR: 1.65 [CI 0.97–2.80], p = 0.06). In the same multivariable logistic regression model, no statistically significant associations were found between TPOAb positivity and PTB, VPTB (Supplementary Table S2). There was no statistically significant difference in PTB rate between TPOAb-positive IMH pregnant women and TPOAb-negative IMH pregnant women (Supplementary Table S3).
Isolated Maternal Hypothyroxinemia and Risk of Preterm Birth
IMH was defined as TSH within normal range (2.5th–97.5th percentile) but with fT4 < 2.5th percentile.
The comparison group is the term birth group, which was ≥37 weeks.
Crude model without adjustment.
Analyses were adjusted for maternal age.
Analyses were adjusted for maternal age, BMI, parity, education level, fetal sex, TPOAb status, and GDM.
CI, 95% confidence interval; fT4, free thyroxine; PTB, preterm birth; OR, odds ratio; TSH, thyrotropin; VPTB, very preterm birth.
In the sensitivity analyses, we defined IMH as fT4 lower than the 5th percentile and TSH within the normal range (2.5th–97.5th percentile). This resulted in 1987 pregnant women being grouped in the IMH group and 39,924 women in the euthyroid group (Supplementary Fig. S1). As shown in Supplementary Table S4, the association between IMH and PTB did not change substantially in these sensitivity analyses. After adjusting for maternal age, BMI, parity, education level, fetal sex, TPOAb status, and GDM, pregnant women with IMH had a higher risk of PTB (OR: 1.24 [CI 1.03–1.50], p = 0.02) and VPTB (OR: 1.57 [CI 1.05–2.33], p = 0.03). In the sensitivity analyses using only participants without missing covariate data, the results were similar (data not shown).
The association between IMH and subtypes of PTB
We further explored the risk of IMH on different clinical subtypes of PTB (PROM-PTB, S-PTB, and MI-PTB). The prevalence of S-PTB in the IMH group was higher than in the euthyroid group in all pregnant women (3.53% vs. 2.09%) (Fig. 2). As shown in Table 3, in crude unadjusted analyses including all pregnant women, those with IMH had a 1.74-fold increased risk of S-PTB compared with euthyroid pregnant women. After adjusting for maternal age, BMI, parity, education level, fetal sex, TPOAb status, and GDM, the association between IMH and S-PTB remained statistically significant (OR: 1.57 [CI 1.11–2.24], p = 0.01). The IMH women had no increased risk of PROM-PTB (OR: 0.98 [CI 0.55–1.76], p = 0.95) and MI-PTB (OR: 1.31 [CI 0.84–2.04], p = 0.23) in adjusted models. We performed sensitivity analyses and obtained similar results (Supplementary Table S5 and Supplementary Fig. S2).
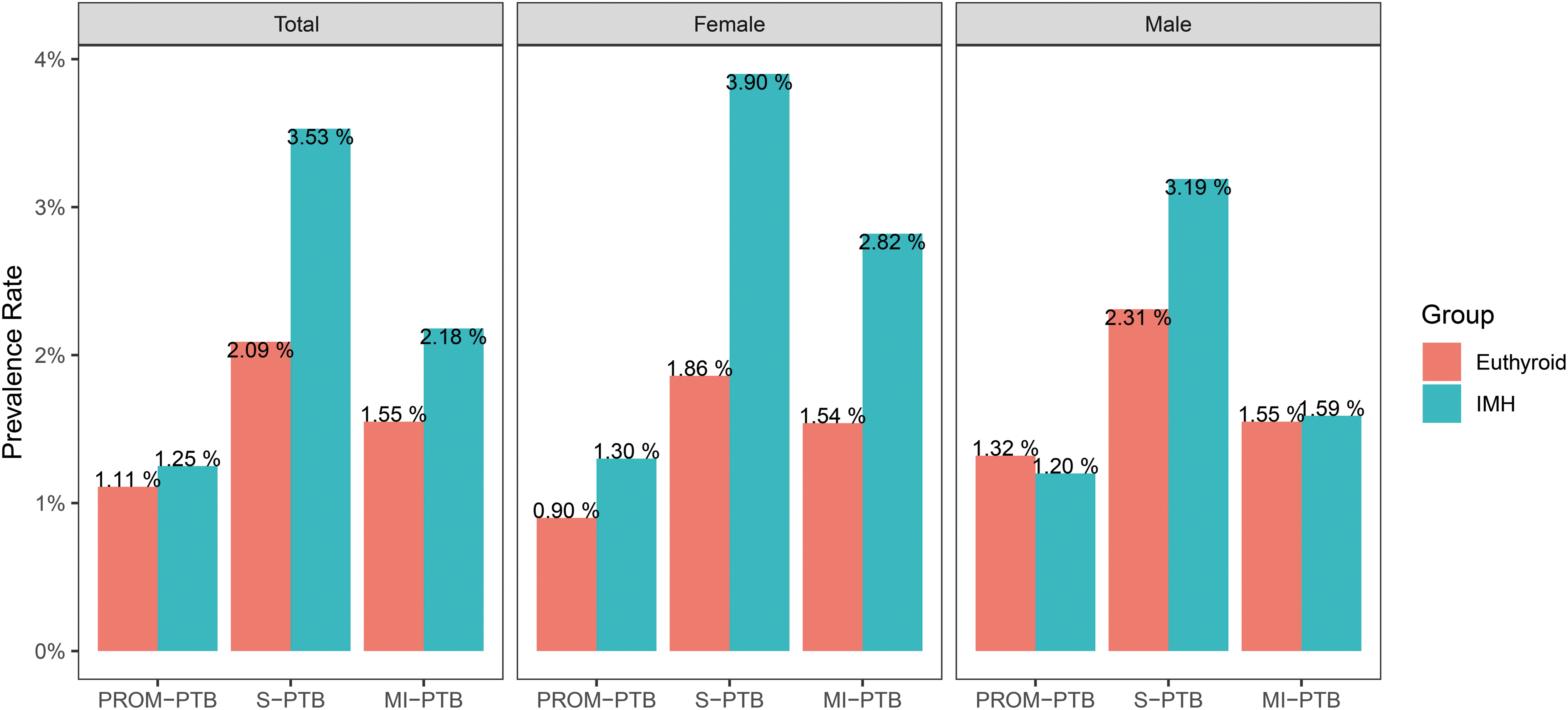
The prevalence of subtypes of PTB between the IMH group and euthyroid group. The IMH was defined as TSH within normal range (2.5th–97.5th percentile) but with fT4 < 2.5th percentile. MI-PTB, medically induced preterm birth; PROM-PTB, preterm birth with premature rupture of membranes; PTB, preterm birth; S-PTB, spontaneous preterm birth with intact membranes.
Univariate and Multivariate Analysis Between Isolated Maternal Hypothyroxinemia and Odds of Subtypes of Preterm Birth, by Fetal Sex
IMH was defined as TSH within normal range (2.5th–97.5th percentile) but with fT4 < 2.5th percentile.
Crude model without adjustment.
Analyses were adjusted for maternal age, BMI, parity, education level, TPOAb status, and GDM.
MI-PTB, medically induced preterm birth; PROM-PTB, preterm birth with premature rupture of membranes; S-PTB, spontaneous preterm birth with intact membranes.
Sex differences in the association between IMH and PTB, VPTB and S-PTB
As shown in Tables 3 and 4, fetal sex modifies the effect of IMH on PTB (p for interaction = 0.04 and 0.08 for PTB and VPTB, respectively). After adjusting for maternal age, BMI, parity, education level, fetal sex, TPOAb status, and GDM, among pregnant women carrying a female fetus with IMH had a 1.70-fold increased risk of PTB (OR: 1.70 [CI 1.20–2.40], p < 0.01), a 2.51-fold increased risk of VPTB (OR: 2.51 [CI 1.30–4.86], p < 0.01), and a 1.99-fold increased risk of S-PTB (OR: 1.99 [CI 1.22–3.24], p < 0.01) compared with euthyroid women. These higher risks were not observed in women carrying a male fetus (PTB; OR: 1.03 [CI 0.71–1.50], p = 0.88, VPTB; OR: 0.99 [CI 0.40–2.43], p = 0.98 and S-PTB; OR: 1.27 [CI 0.76–2.13], p = 0.35). As shown in Supplementary Tables S5 and S6, similar effects were found in the sensitivity analyses.
Univariate and Multivariate Analysis Between Isolated Maternal Hypothyroxinemia and Odds of Preterm Birth, by Fetal Sex
IMH was defined as TSH within normal range (2.5th–97.5th percentile) but with fT4 < 2.5th percentile.
Crude model without adjustment.
Analyses were adjusted for maternal age.
Analyses were adjusted for maternal age, BMI, parity, education level, TPOAb status, and GDM.
We studied the combined effects of IMH and fetus sex on preterm birth by adding a product term of the IMH × sex to the model and generating p for interaction.
Discussion
In this study, we found that pregnant women with IMH had a 1.32-fold increased risk of PTB compared with euthyroid women. The increased risk of PTB was mainly driven by a 1.57-fold increased risk of S-PTB, while women with early pregnancy IMH had no statistically significant increased risk of PROM-PTB and MI-PTB. In addition, these effects were modified by fetus sex.
It is still debated whether the risk of PTB is higher in pregnant women with IMH. Studies on this topic are a few in number. The first meta-analysis conducted on this topic by Sheehan et al. (17) in 2015 included five studies and a total of 458 IMH cases. This study did not find a significantly increased risk of PTB. However, a subsequent meta-analysis (18) with 1078 IMH cases in 2017 and a systematic review with 904 IMH cases in 2019 (19) indicated a 1.33- and 1.46-fold increased risk of PTB, respectively. The small number of studies with a small sample size in each individual study might affect the result of these meta-analyses. Cleary-Goldman et al. (8) found that IMH in the first trimester was associated with a 1.62-fold [CI 1.00–2.62] increased risk of preterm labor, but not with an increased risk of PTB in a population of 232 pregnant women with IMH. Only one cohort study in the Netherlands with 145 IMH cases found that hypothyroxinemia in the first half of pregnancy was associated with a 2.54-fold [CI 1.42–4.54] increased risk of PTB and a 3.56-fold [CI 1.50–8.43] increased risk of VPTB (9). In line with this study, we observed a similar increased risk, which was a 1.34-fold increased risk of PTB. We also observed a 1.65-fold [CI 0.97–2.80] increased risk of VPTB, which was not statistically significant. It might be due to the small number of VPTB cases in the IMH group. When IMH was defined as fT4 lower than the 5th percentile and TSH within the normal range, which resulted in a larger number of VPTB cases, we observed a 1.57-fold increased risk of VPTB [CI 1.05–2.33], which was statistically significant.
One possible reason for the inconsistent findings of previous studies might be variability in the diagnostic criteria of IMH. The fT4 cut-off levels in previous studies ranged from the 2.5th to the 10th percentile (12). Some studies had to use higher percentiles as a cut-off to increase the number of IMH cases. In addition, IMH of these studies is under a different gestational stage, which might make the result not comparable. A study by Cleary-Goldman et al. (8) found that IMH in the first and second trimester is associated with different adverse pregnancy outcomes. This indicates that the effect of IMH might be dependent on gestational stage.
To our knowledge, no previous studies differentiated subtypes of PTB and explored which subtype of PTB attributed most to the association between IMH and PTB. Different subtypes of PTB are due to different etiologies and mechanisms. For example, PROM-PTB is likely be related to inflammation and infection, while S-PTB is more likely associated with progesterone withdrawal, oxytocin initiation, and decidual activation (15). Therefore, assessing which subtype of PTB is associated with IMH could offer more information on the underlying mechanism linking IMH to PTB. In this study, we found that IMH is associated with an increased risk of S-PTB but not with PROM-PTB. Our result is consistent with that of Cleary-Goldman et al., who found no association of IMH with PROM but is discordant with a study showing that women with IMH had a higher risk of PROM-related spontaneous PTB than euthyroid women (9). PROM is closely related to inflammation and, therefore, the higher PTB risk in the IMH group may not have been induced by inflammation. In this study, we did not find an association of IMH with MI-PTB, which is commonly caused by pre-eclampsia or eclampsia and intrauterine growth restriction (15).
We found that IMH is associated with an increased risk of S-PTB, which implies that IMH is related to the mechanisms that lead to the early onset of labor. Several potential pathways might be involved in this association between IMH and the onset of S-PTB. For example, studies reported elevated levels of vasopressin (20), which plays a critical role in the onset of labor in pregnant women with hypothyroidism. In addition, hypothyroidism increases oxidative stress (21), which is associated with the occurrence of PTB with an intact membrane (22,23).
Limited research is available to justify LT4 treatment to decrease the risk of PTB in pregnant women with IMH. An observational study compared the PTB rate between 95 IMH cases who chose to receive LT4 in early pregnancy and 106 untreated IMH cases. No statistically significant differences were found, but there were only five and two PTBs in those two groups, respectively (14). A recent randomized controlled trial reported that LT4 treatment in IMH patients did not decrease the risk of PTB compared with placebo (24). However, PTB was one of the secondary outcomes, and no power analysis for secondary outcomes was provided in that study.
Interestingly, we observed an increased risk of PTB only in women with a female fetus in our study. This is the first study that shows that maternal thyroid status affects PTB in a sex-specific manner, with the effect mainly driven by S-PTB. However, the mechanism behind this higher risk of S-PTB in IMH women carrying a female fetus is unclear. A sex-related intrauterine change in metabolism might exist in hypothyroxinemia circumstances. The intrauterine environment plays a critical role in the prevalence of spontaneous PTB (25,26). In addition, studies found that redox imbalances may contribute to the sexual dimorphism of thyroid diseases (27,28).
Our study has some limitations. First, IMH was defined in early pregnancy. We did not study the association between IMH in late pregnancy and PTB. Second, although a series of potential confounders were added to the adjusted model, the possibility of residual confounding could not be completely ruled out. Further, since our study was an observational study, the beneficial effects of LT4 therapy in IMH could not be established. The current consensus is that IMH should not be routinely treated in pregnancy (1). Whether LT4 treatment will be beneficial in reducing the risk of PTB in pregnant women with IMH, especially for IMH women with a female fetus, requires further exploration.
In conclusion, our study suggests that IMH is associated with an increased risk of PTB. The increased risk of PTB is mainly driven by S-PTB. Our study also indicates a fetal sex-specific association between IMH and the risk of PTB, which requires further exploration.
Footnotes
Acknowledgments
The authors thank the pregnant women who participated in this study. They also thank the doctors and nurses who assisted with recruiting patients into this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the National Key Research and Development Program of China (2018YFC1004602), Shanghai Municipal Commission of Health and Family Planning (15GWZK0701), and the International Cooperation Project of China and Canada NSFC (81661128010).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6