
Abstract
Background:
Newer transoral thyroidectomy techniques that aim to avoid scars in the neck and maximize cosmetic outcomes have become more prevalent. We conducted a discrete choice experiment (DCE) to evaluate the influence of cosmetic concerns and other factors on patients' decision-making processes when choosing among different thyroidectomy approaches.
Methods:
A questionnaire was developed to identify key attributes driving patient preferences around thyroidectomy approaches using mixed analyses of patient focus groups, expert opinion, and literature review. These attributes included (i) risk of recurrent laryngeal nerve (RLN) injury, (ii) risk of mental nerve injury, (iii) travel distance for surgery, (iv) out-of-pocket cost, and (v) incision site. Using fractional factorial design, discrete choice sets consisting of randomly generated hypothetical scenarios across all attributes were created. A face-to-face DCE survey was administered to patients being evaluated in clinic for thyroid lobectomy for noncancerous thyroid disease. Participants chose among scenarios constructed from the choice sets of attributes. Analyses were conducted using a mixed logit model, and the trade-offs between different attributes that patients were willing to accept were quantified.
Results:
The DCE was completed by 109 participants (86 [79%] women; mean age 51.3 ± 3.0 years). Overall, the risk of having RLN and/or mental nerve injury, travel distance, and cost were the most influential attributes. Participants aged ≤60 years significantly preferred an approach without a neck incision and were willing to accept an additional $2332 USD in out-of-pocket cost, 693 miles of travel distance, 0.6% increased risk of RLN injury, and 2.2% risk of mental nerve injury. Patients aged >60 years significantly preferred a conventional neck incision and were willing to pay an additional $3401 out-of-pocket and travel 1011 miles to avoid a scarless approach.
Conclusions:
The risk of nerve injury, travel distance, and cost were the most important drivers for patients choosing among surgical approaches for thyroidectomy. Cosmetic considerations also influenced patient choices, but in opposing ways depending on patient age.
Introduction
Thyroidectomy is the most commonly performed cervical endocrine operation, with more than 200,000 cases performed annually in the United States. The conventional technique of thyroidectomy via transverse cervical incision has existed in its fundamental form for over a century, although with several improvements over time that have led to its evolution into the safe and effective procedure it is today. Over the past two decades, the advent of new surgical technologies—particularly endoscopic instrumentation—was accompanied by greater interest in the adverse consequences due to the presence of a neck scar from conventional thyroidectomy (1). The convergence of these two forces led to the development of several so-called remote access techniques that relocate the incision to more hidden areas of the body.
One recently developed remote access thyroidectomy technique utilizing transoral endoscopic incisions in the oral vestibule has gained attention and adoption in the United States over the past several years because of its virtual obviation of a visible scar. This technique, dubbed the TransOral Endoscopic Thyroidectomy–Vestibular Approach (TOETVA), largely supplanted all other transoral or natural orifice thyroidectomy techniques because of a large and growing body of literature suggesting a favorable safety and efficacy profile (2,3). A modification of TOETVA known as TransOral and Submental Technique (TOaST), which relocated the middle endoscopic incision to a hidden location underneath the chin, was developed in an effort to reduce postoperative chin discomfort and accommodate larger incisions than the standard TOETVA incision would allow. One study estimated that these techniques may be applicable to over half of patients being evaluated for thyroidectomy in endocrine surgery practices (4).
The advent of these transoral and other remote access techniques requires a comprehensive and nuanced discussion with patients about the relative benefits and risks of each approach; however, such a discussion would be improved with a greater understanding of patient-level preferences when deciding among different thyroidectomy approaches than is currently available (5). Having a better understanding would help improve shared decision-making between surgeons and patients by identifying and evaluating the factors that are most important in choosing a particular surgical approach.
Discrete choice experiment (DCE) is a modeling method originally used in behavioral economics and increasingly used in health care that identifies and quantifies the various preferences people consider when making a decision among a finite set of choices (6 –8). In this experimental model, participants are asked to choose between a number of scenarios that have been systematically randomized according to a number of attributes that serve as the main decision-driving variables. The aggregate data are then analyzed to estimate the probability of certain decision profiles as well as the relative importance of each individual attribute and the trade-offs between attributes that people are willing to accept. We conducted a DCE designed to evaluate patient preferences when choosing between the conventional open thyroidectomy and transoral thyroidectomy approaches.
Methods
Study setting and participants
The DCE was conducted as a face-to-face survey enrolling a voluntary sample of adult U.S. patients aged 18 years and older seen in the endocrine surgery clinic at a high volume tertiary/quaternary urban academic medical center from November 2018 to May 2019 who were deemed eligible for unilateral thyroid lobectomy as treatment for a noncancerous thyroid condition. Disease-based inclusion criteria followed current accepted indications for transoral unilateral thyroid lobectomy, which included: (i) cytologically benign (Bethesda 2) thyroid nodule ≤6 cm in maximal dimension; (ii) cytologically indeterminate (Bethesda 3 or 4) thyroid nodule ≤4 cm in maximal dimension; or (iii) a goiter with maximal unilateral lobe dimension ≤10 cm in which unilateral lobectomy was the treatment agreed upon by the patient and surgeon. Exclusion criteria included a preoperative high suspicion for, or cytological diagnosis of, thyroid cancer.
The patients were first evaluated by one of the seven attending endocrine surgeons (Q.-Y.D., J.E.G., S.A.R., W.T.S., C.D.S., J.A.S., and I.S.) as part of their initial surgical consultation and were screened for study eligibility. As a part of the standard of care, the surgical consultation included a comprehensive description of the disease process, surgical indication, and benefits and risks of open thyroid lobectomy. A single surgeon (I.S.) also selectively described the details, benefits, and risks of transoral techniques as a part of the consultation. Patients underwent final screening for study eligibility after the surgeon consultation. Eligible participants then underwent written informed consent, and the face-to-face DCE survey was conducted with study coordinators. The timing of the survey was chosen to take place right after surgeon consultation because this would capture patients at their most educated and informed about their condition and surgical management, with the relevant knowledge fresh in their minds.
Demographic and clinical data were obtained via patient self-report and electronic medical record review. Written informed consent was obtained from each participant. This study was approved by the institutional review board of the University of California, San Francisco. Because the study design called for patients to be recruited and enrolled only and immediately after surgeon evaluation, the study was incompatible with public listing in a national database such as ClinicalTrials.gov.
Development of attributes and levels
DCE is at its core a theoretical experiment designed to analyze decisions made from hypothetical scenarios. DCE methodology is based on the idea that the value of any choice can be described by its individual characteristics, otherwise known as “attributes,” and that the value of each attribute to the ultimate decision as well as to one another can be quantified by presenting participants with a series of different hypothetical scenarios that vary the degree or “level” of each attribute.
The identification of attributes for this DCE was based on literature review, and their respective importance was pilot-tested in a series of initial qualitative interviews with eight thyroid surgery patients and a seven-surgeon expert opinion panel. The list of identified attributes was then ranked in importance based on qualitative survey of a focus group of eight additional thyroid surgery patients. The final five attributes validated through this process included: (i) incision site, (ii) risk of mental nerve injury, (iii) risk of recurrent laryngeal nerve (RLN) injury, (iv) travel distance, and (v) out-of-pocket cost (Table 1). Notably, attributes related to the surgical implications of a preoperative cancer diagnosis, as well as the risk of hypoparathyroidism, were excluded intentionally based on the study design and inclusion of only patients undergoing unilateral thyroid lobectomy for noncancerous diagnoses. Levels were selected based on the literature review and an expert panel including all study authors. Levels should generally reflect a wide range of possible outcomes in order for the DCE to have discriminatory power for analysis. To be relevant, the chosen attributes and levels should fall within reasonable and realistic ranges, which is why, for example, the three level options given to participants for the risk of losing the voice were chosen as 1%, 2%, and 5%.
Selected Attributes and Attribute Levels
RLN, recurrent laryngeal nerve.
DCE design
Using a full factorial design for the DCE would yield a total of 324 possible combinations of attributes and levels. This large number was problematic for two reasons.
First, it would not be practical to ask participants to consider all 324 alternatives in a single survey. Second, some combinations were unrealistic; for example, it would be virtually impossible for either a conventional neck incision to lead to any risk of mental nerve injury or a transoral approach to be completely free of mental nerve injury risk. Therefore, we constructed a nested attribute combining the “incision site” and “risk of mental nerve injury” together (Supplementary Table S1) and then employed a validated orthogonal fractional factorial design on this new set of nested attributes and levels (9).
This reduced the final number of scenarios for participants to evaluate to 27, which was both practical for survey completion but also statistically sufficient to estimate the impact of each attribute on patient preferences, which were measured as utility values. The final set of 27 orthogonally generated scenarios were then grouped into nine separate choice sets consisting of three scenarios—that is, with each attribute independently chosen with no clearly dominant choice (Fig. 1).
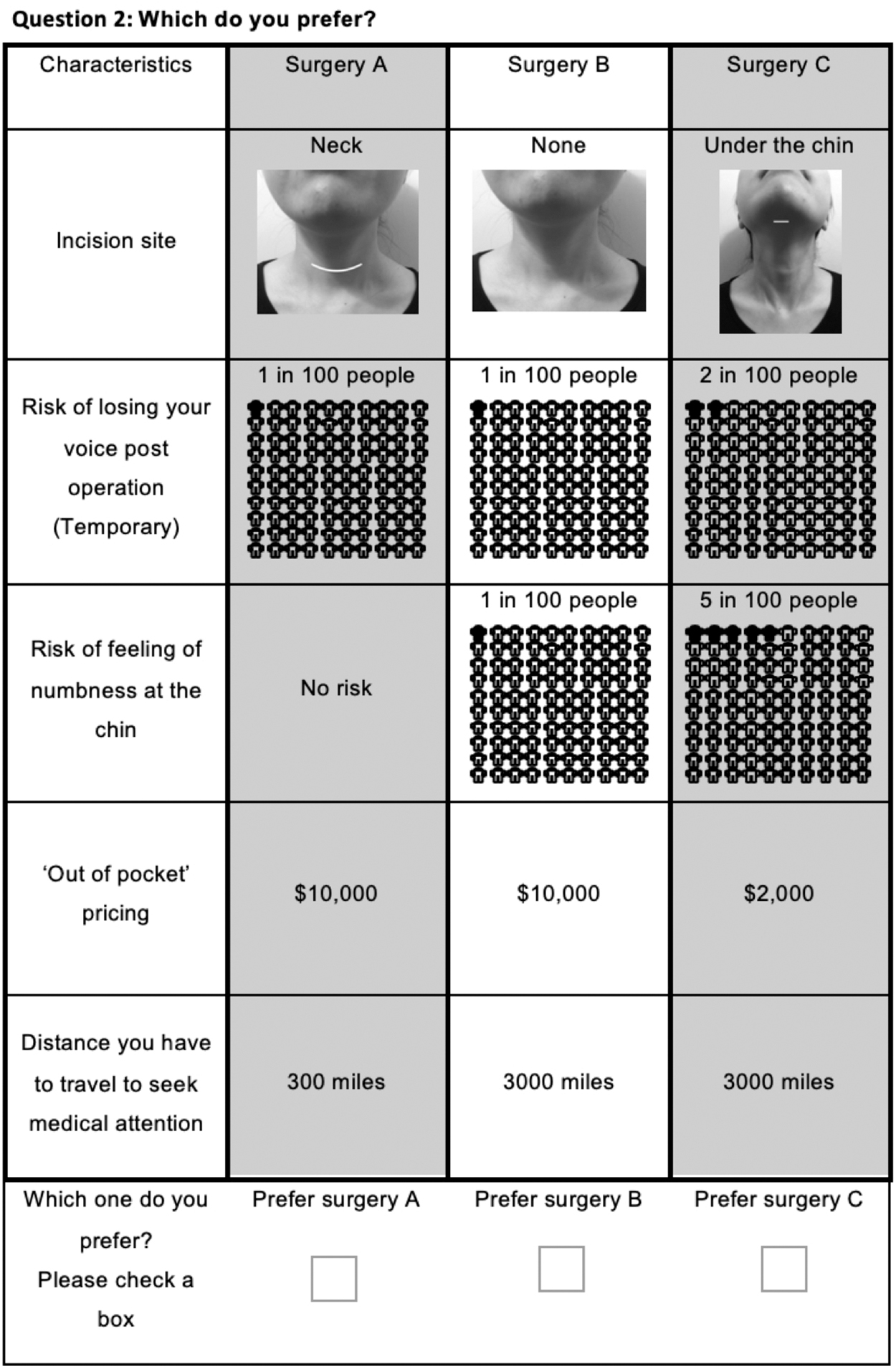
Sample of discrete choice task.
Statistical analyses
DCE analysis was performed using a mixed logit model (or random parameter logit) technique to estimate the relative priority participants placed on each attribute. In the mixed logit model, each decision in a choice set presenting three scenarios is defined as an observation; since each survey had nine choice sets consisting of three scenarios to choose from, each participant provided nine observations. The impact of each attribute on patient preference (or utility) was analyzed by treating the decision made by participants as a dependent variable and the different levels for each attribute as independent variables. Results are reported as β coefficients with 95% confidence interval [CI]. Coefficients were treated as normally distributed parameters. A positive or negative β coefficient reflected whether the attribute had a positive or negative effect on the preference (utility), and higher absolute values reflected the strength of preference.
The utility function is as follows:
where
V represents the utility (preference score) derived for a thyroidectomy scenario.
“Submental” and “Transoral” are dummy variables for the incision sites associated with the TOaST and TOETVA techniques, respectively, in which the conventional neck incision is set as the base level.
“Age” is a dummy variable to account for a patient older than 60 years, with the base level defined as a patient aged 60 years or younger.
Numbness at the chin and loss of voice (coded above as “Numb” and “Voice,” respectively) are variables representing the risk of mental nerve injury and risk of RLN injury, respectively.
β1–β8 are the coefficients that indicate the relative importance of each attribute (level);
β1 and β2 indicate the relative importance of the TOaST and TOETVA incisions compared with conventional neck incision for younger patients.
β3 and β4 are used to analyze the difference between how older versus younger patients perceive the location of the incision site; for example, (β1 + β3) and (β2 + β4) would be used to calculate the relative importance of the TOaST and TOETVA incisions, respectively, compared with the conventional neck incision for older patients.
The trade-offs between attributes that participants were willing to accept were calculated from the ratios of their respective coefficients.
Sample size requirements for this DCE were approximated by the previously described formula: (10)
where
c is the largest number of levels for any of the attributes.
t is the number of choice sets completed per respondent.
a is the number of scenarios per choice set.
The estimated required sample size per this method was 56 patients. These methods for estimating DCE sample size are not meant for explicit power calculation and are instead meant as a guide. We set out to recruit 100 patients.
Statistical analyses were performed using SPSS software (IBM Corp, Armonk, NY).
Results
Participants
The DCE was completed by 109 participants (Table 2). The majority were female (79%). The mean age was 51.3 years (range 18–87 years), with 43% of participants falling in the 41–60 year age group. Most patients identified themselves as white (66%), although a relatively high proportion of participants identified as Asian (19%), likely reflecting the diversity of the surrounding patient population. Most participants were covered by private insurance (70%), with the remainder covered by Medicare or Medicaid. Most participants had high educational status, with 82% reporting at least obtaining an undergraduate college degree. Of the 109 total participants, 9 underwent a transoral approach (4 TOETVA and 5 TOaST) for thyroid lobectomy. The other 100 underwent traditional open thyroid lobectomy.
Respondent Characteristics
Four respondents had both Medicare and supplemental private insurance.
Percentage of income range and education level based on reported data.
Preferences, attributes, and trade-off analyses
Overall, the attributes that most significantly influenced preferences between thyroidectomy approaches were the risk of RLN injury (β coefficient −0.71 for every 1% increased risk of injury [CI −0.92 to −0.51]), risk of mental nerve injury (β coefficient −0.20 for every 1% increased risk of injury [CI −0.25 to −0.14]), out-of-pocket cost (β coefficient −0.0002 for every $1 increase in cost [CI −0.0002 to −0.0001]), and traveling distance to seek surgical treatment (β coefficient −0.0006 for every 1 mile increase in distance [CI −0.0007 to −0.0005], Table 3). Attributes behaved in the expected directions as the levels increased; for instance, increasing the risk of complications made a scenario less likely to be selected in any given choice set. The same directionality held true for increased out-of-pocket cost and travel distance, which were associated with a lower probability of selection.
Estimated Coefficients and Marginal Willingness to Pay (All Patients)
CI, 95% confidence interval.
The relative importance of each attribute was demonstrated by willingness-to-pay trade-off analysis. Participants were willing to pay $3842 and $1060 USD for every 1% reduction in the risk of RLN injury and mental nerve injury, respectively, and $3.36 for every mile reduction of travel distance (Table 3). The importance of these attributes did not differ significantly when analyzed separately based on other demographic characteristics including sex, race/ethnicity, employment/personal/insurance status, or education level.
The importance of incision location was highly dependent on participant age. Stratification of participants by decade-age groups revealed a dichotomy in preference patterns at an age cutoff of 60 years. Patients aged ≤60 years were significantly more likely to prefer the TOETVA approach over the conventional incision (β coefficient 0.43 [CI 0.02 to 0.85]), whereas patients aged >60 years significantly preferred the conventional incision over either the TOETVA (β coefficient −0.63 [CI −1.22 to −0.05]) or TOaST approaches (β coefficient −0.88 [CI −1.63 to −0.16]) (Table 4).
Estimated Coefficients and Marginal Willingness to Pay by Age Groups
Trade-off analyses in each age group are summarized in Table 5. Participants aged ≤60 years were willing to pay $2332 more in out-of-pocket cost, as well as travel an additional 693 miles, to undergo the TOETVA approach when compared with the conventional neck incision. In addition, they were willing to accept a 2.2% risk of mental nerve injury as well as an additional 0.6% risk above the baseline for RLN injury. In contrast, participants aged >60 years were willing to pay $3401 and travel 1011 miles, as well as tolerate a 3.2% additional risk of RLN injury, for a conventional neck incision when compared with the scarless TOETVA approach.
Trade-Off Analysis of Other Attributes That (A) Patients Aged ≤60 Years Would Be Willing to Accept to Avoid a Neck Incision/Scar and (B) Patients Aged >60 Years Would Be Willing to Accept to Have a Conventional Thyroidectomy and Neck Incision
Discussion
In this DCE study, we aimed to evaluate the influence of cosmetic concerns and their relationship to other factors in patient decision-making when choosing among various technical approaches to thyroid lobectomy for a noncancerous thyroid condition. We found that overall, the risk of surgical complications (specifically, RLN and mental nerve injuries), out-of-pocket cost, and traveling distance were the most significant attributes affecting patients' decisions. Cosmetic concerns, as assessed by patient preferences for the presence/absence and location of incisions, also influenced patient decision-making but in different ways according to patient age. Younger patients significantly preferred the approach associated with no skin incision; however, older patients not only did not mind the presence of a conventional neck incision, but they demonstrated a significant preference for a conventional incision over either of the “scarless” approaches. To the best of our knowledge, this is the first report to use the robust DCE method to quantify the relationship between age and cosmetic concerns as they relate to decisions around thyroidectomy approach.
Previous investigations have examined the association of neck scars and patient satisfaction after thyroidectomy (11,12). A number of studies spanning different countries, patient populations, and thyroidectomy techniques have suggested that the majority of patients were satisfied with their neck scars, with one study concluding that thyroidectomy should not be performed with a small incision purely for esthetic reasons (13 –16). There is also a body of literature that suggests that cosmetic concerns are important to some patients earlier on in the postoperative course, but abate progressively over several years (17,18). However, one prospective study of patient perspectives by Chaung et al. found that across a broad range of demographic subgroups, patients preferred smaller and thinner incisions for thyroidectomy (19). In a survey study of 812 randomly selected individuals in Wisconsin without known thyroid disease, Coorough et al. found that participants were more likely to prefer an approach avoiding a neck scar (with a transaxillary approach) even at the expense of a higher complication rate and monetary cost (20). Arora et al. surveyed 120 patients who had undergone thyroid or parathyroid surgery in England and found that scar-related problems were among the most common postoperative complaints, with the negative impact worse in those of Asian or African ancestry; in addition, the vast majority of respondents expressed a clear retrospective preference for a surgical approach that would eliminate a neck incision (21).
Although helpful, these survey studies are characterized by one or more of the following limitations: (i) recall bias from questionnaires asking patients to remember aspects of their treatment from different time points in the past; (ii) lack of information provided to subjects regarding the option of alternative thyroidectomy approaches, or (iii) survey of nonrepresentative patient populations. Accordingly, our study sought to overcome these limitations in that it was a prospective study in patients with a thyroid condition warranting lobectomy but who had not yet been biased by having undergone surgical treatment. We also designed our study to exclude patients with a preoperative thyroid cancer diagnoses to avoid the introduction of additional confounding variables and attributes that would make our analysis more unwieldy.
One of the strengths of the DCE method is that it is able to quantify patient preferences and thus calculate trade-offs between attributes that patients are willing to accept. In our study, we found that younger patients were willing to pay over $2000 out of pocket and travel nearly 700 miles to avoid a neck incision and tolerate a mild increase in complication rate. This directionality in younger patients is generally consistent with the findings of Coorough et al., but the DCE model provides a more precise and robust estimate of these trade-off thresholds. In older adults, we were surprised to discover how strongly the preferences were reversed, in that this cohort was willing to accept greater cost, travel distance, and complications to avoid the scarless approaches. We believe that these results should help inform both patients and surgeons when deciding on technical approaches to thyroidectomy.
One finding of interest to our current clinical practice was that although we found the standard TOETVA approach to be preferred in younger patients, our study did not see a similar finding for the modified TOaST approach, which results in virtually the same cosmetic result as TOETVA. What's more, the TOaST approach was found in this DCE to be even less desirable than the TOETVA approach in the older patients compared with the conventional approach. This discrepancy conflicts with our own patients' esthetic assessment of this approach, which has anecdotally been quite positive, specifically because the submental incision remains hidden from view in most social situations. Nevertheless, we believe this particular result highlights the idea that patients can have strong reactions to the visual representation of a visible scar on the neck or under the chin. This concept is supported by a recent study using eye-tracking software, which found that the presence of a visible neck scar leads to significant gaze distraction of viewers away from the face (22).
Our study has several additional limitations. First, DCE is not designed to include every possible attribute that may be important to the decision in question, so it is possible that we did not include other important attributes. Second, the study's exclusion of patients without a preoperative diagnosis of thyroid cancer may not have completely eliminated the confounding influence of attributes related to oncological management, particularly by our inclusion of patients with indeterminate nodules. We minimized these two risks by following a careful and iterative process of ranking and selecting our attributes from a diversified set of methods including the literature review, expert opinion, and patient focus groups. Third, the participants completed the surveys after initial surgeon evaluation, which could potentially bias survey responses depending on the content and tone of surgeon discussion. However, we believe that the advantages of survey patients right after a comprehensive surgical evaluation were critical to capture subjects at their most educated and informed; indeed, the alternative—that is, conducting the DCE before surgeon consultation—would introduce different and less desirable drawbacks since patients would not yet have a reasonable understanding of critical information such as whether they actually need an operation, the extent of operation required, and general expectations of surgery, to intelligently complete the DCE survey.
Fourth, by design the attributes used standardized levels of risk and cost for each of the thyroidectomy approaches, which do not take into account individual variations of risk and cost based on thyroid pathology, patient comorbidities, surgeon experience, and geographic differences in cost of living. Fifth, bias favoring the nonconventional approaches could have possibly been introduced in some patients through selective discussion of the transoral procedure by the only transoral surgeon in the group (I.S.). To control for this, we performed a separate sensitivity analysis excluding patients evaluated by this surgeon, with no substantive differences in our findings. Finally, the study participants were enrolled from the patient population seen at a single tertiary/quaternary referral center in the San Francisco Bay Area, composed of a relatively higher proportion of people with private insurance, greater education level, and of Asian ethnicity; this unique patient makeup may not be generalizable to other populations in the United States. Thus, it would be important for future investigations to determine whether our findings are replicable in other settings and cultures.
In conclusion, the increasing availability of alternative-access approaches to thyroidectomy that aim to eliminate a visible neck scar must be accompanied by a greater understanding of the complex interplay of factors that contribute to patients' decisions on whether to pursue them. This DCE provides new information on the priority of avoiding neck scars in some patients by quantifying its importance relative to other factors that patients consider when undergoing thyroid lobectomy. Further investigations into the effect of age on patient preferences regarding the presence of a neck scar after thyroidectomy will help surgeons further define the appropriate patients for these techniques as well as inform patients' decision-making.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No specific funding was obtained for this study.
Supplementary Material
Supplementary Table S1