
Abstract
Background:
Iodine intake is associated with thyroid autoimmunity. In this study, we evaluated the changes in thyroid autoimmunity after 20 years of universal salt iodization (USI) in China.
Methods:
A total of 78,470 subjects (18 years or older) from 31 provincial regions of mainland China participated in the study. Serum thyroid peroxidase antibody (TPOAb), thyroglobulin antibody (TgAb), TSH receptor antibody, thyrotropin (TSH), and urinary iodine concentration (UIC) were measured.
Results:
Positive TPOAb and TgAb were detected in 10.19% [CI 9.80–10.59] and 9.70% [CI 9.28–10.13] of the subjects, respectively. The prevalence of positive isolated TPOAb (i-TPOAb), positive isolated TgAb (i-TgAb), and double positive TPOAb and TgAb (d-Ab) was 4.52%, 4.16%, and 5.94%, respectively. The prevalence of thyroid antibody positivity was the highest in the iodine-deficient (UIC <100 μg/L) groups. The prevalence of i-TPOAb was inversely associated with more than adequate iodine intake (MAI) and excessive iodine intake (EI); the odds ratio (OR) was 0.89 [CI 0.81–0.98] for MAI and 0.90 [CI 0.81–0.99] for EI. We observed that i-TgAb, like i-TPOAb, was a high-risk factor for subnormal TSH levels (OR = 3.64 [CI 2.62–5.05]) and elevated TSH levels (OR = 1.62 [CI 1.49–1.77]). The prevalence of thyroid antibody positivity varied among five ethnic groups.
Conclusions:
After two decades of USI, the prevalence of thyroid antibody positivity has remained low. MAI and EI had an inverse relationship with TPOAb positivity, which reveals that UIC between 100 and 299 μg/L is optimal and safe for thyroid autoimmunity. These conclusions need to be confirmed in a follow-up study because this study was a cross-sectional study.
Introduction
Iodine is an important trace element that is involved in the synthesis of thyroid hormones and affects thyroid function and thyroid autoimmunity (1 –4). The presence of thyroid antibodies is an important marker of thyroid autoimmunity, which is closely related to severity of lymphocyte infiltration in the thyroid glands (4). However, the relationship between iodine intake and thyroid autoimmunity has not been determined. The effect of excess iodine and iodine supplementation on thyroid autoimmunity has become a research focus within the scientific community because the global salt iodization strategy has been in place for more than 20 years (2).
The universal salt iodization (USI) program, which was implemented in 1996 in China, has the following characteristics. First, USI was implemented in 1995 based on the sufficient iodine status with a median urinary iodine concentration (UIC) of 165 μg/L (5). Second, the national standard for salt iodine concentration was high, and household salt iodine concentration was generally higher than 30 mg/kg. Third, mandatory USI was strictly enforced, covering all geographical areas, and consumption of iodized salt was >98% in those areas. Fourth, in 2002 and 2011, the national standard for salt iodine concentration was reduced, resulting in a median UIC (MUI) of 199.7 μg/L in 2017 (6). Therefore, China was exposed to 6 years of excessive iodine intake (EI), 10 years of more than adequate iodine intake (MAI), and 4 years of adequate iodine intake (AI) from 1996 to 2016 (Supplementary Fig. S1).
To understand the changes in thyroid disorders after more than 20 years of USI in China, we conducted an epidemiological survey in 31 provinces of mainland China. The overall results have been previously reported (6). This study analyzed the effects of iodine intake on thyroid autoimmunity.
Materials and Methods
Subjects and study design
This study had a four-stage stratified design with cluster sampling from urban and rural areas in parallel (Supplementary Fig. S2) (6). The inclusion criteria were nonpregnant adults, aged 18 years or older, who had lived in the selected communities for no less than 5 years, and had not received any iodine-containing drugs or contrast agents in the previous three months. A total of 78,470 subjects participated in the study, which was approved by the Medical Ethics Committee of China Medical University. All subjects were provided with informed consent forms.
Anthropometric indices and laboratory measurements
Demographic information (age, sex, nationality, and location) and data on personal and family history of thyroid diseases and current smoking status were collected using a standard questionnaire. Body weight and height were measured while the study subjects were wearing light clothing and no shoes. Fasting blood and urine samples were collected. Serum samples obtained from centrifuged blood samples were stored at −20°C before analyses. All specimens were transported in a cold chain system to a central laboratory in Shenyang, China.
We measured serum thyrotropin (TSH), thyroid peroxidase antibody (TPOAb), and thyroglobulin antibody (TgAb) in all subjects. TSH receptor antibody (TRAb), free thyroxine (fT4), and free triiodothyronine (fT3) were measured in subjects with TSH <0.27 mIU/L by electrochemiluminescence using a Cobas 601 analyzer (Roche Diagnostics, Switzerland).
The sensitivity of the TSH assay was 0.014 μIU/mL. The intra-assay coefficients of variation (CVs) for TSH, fT4, fT3, TPOAb, TgAb, and TRAb ranged between 1.1% and 6.3%, and the interassay CVs ranged between 1.9% and 9.5%. According to the test kit manufacturers, the reference ranges for TSH, fT4, fT3, TPOAb, TgAb, and TRAb were 0.27–4.2 mIU/L, 12.0–22.0 pmol/L, 3.1–6.8 pmol/L, <34.0 IU/mL, <115.0 IU/mL, and <1.75 mIU/L, respectively. Isolated positive TPOAb (i-TPOAb) was defined as having TPOAb ≥34.0 IU/mL and TgAb <115.0 IU/mL. Isolated positive TgAb (i-TgAb) was defined as having TgAb ≥115.0 IU/mL and TPOAb <34.0 IU/mL. Double positive TPOAb and TgAb (d-Ab) were characterized by TPOAb ≥34.0 IU/mL and TgAb ≥115.0 IU/mL.
UIC was assessed by inductively coupled plasma mass spectrometry (Agilent 7700x; Agilent Technologies). Certified reference material (GBW09108, GBW9109, and GBW9110) from the Center for Disease Control (CDC) in China was used to control measurement quality, and the target values were 70 · 8 ± 9.0, 143 ± 10, and 224 ± 14 μg/L. The interassay CVs were 2.3%, 2.5%, and 2.4% and intra-assay CVs were 2.7%, 1.4%, and 2.3%, respectively. The iodine nutrition evaluation criteria recommended by the World Health Organization (WHO) were the following: UIC <100 μg/L for iodine deficiency (ID); UIC 100–199 μg/L for AI; UIC 200–299 μg/L for MAI; and UIC ≥300 μg/L for EI.
Statistical analysis
We used SPSS 21.0 for data handling and statistical analysis. The Kolmogorov–Smirnov method was used to test the normality of continuous variables. Variables that were not normally distributed were expressed as median with interquartile range and analyzed using the Mann–Whitney U test or Kruskal–Wallis test for comparison of two or more groups. Categorical variables presented as counts and percentages were analyzed by the chi-square test. Logistic regression models were used to identify the independent factors of positive thyroid antibodies and evaluate the association between positive thyroid antibodies and thyroid dysfunction. The results were expressed as adjusted odds ratio (OR) and 95% confidence interval (CI). Statistical significance was set at p < 0.05. Corrected p-values were used for pairwise comparisons of multiple groups.
Results
Prevalence of positive thyroid antibodies
Positive TPOAb and TgAb were detected in 10.19% [CI 9.80–10.59] and 9.70% [CI 9.28–10.13] of the subjects, respectively (6). The prevalence of positive thyroid antibodies was highest in the ID group: 5.60% for i-TPOAb, 4.98% for i-TgAb, and 7.30% for d-Ab (Table 1). The prevalence rates were significantly higher in women than in men. Specifically, women had 1.71 times higher i-TPOAb levels, 3.43 times higher i-TgAb levels, and 2.95 times higher d-Ab levels than men, especially in the 40- to 60-year-old group.
Prevalence of Positive Thyroid Antibodies Stratified by Sex
Chi-square test results compared with results obtained from women, p < 0.05.
Chi-square test results compared with results obtained from Han, p < 0.05/4 = 0.0125.
Chi-square test results compared with UIC 100–199, p < 0.05/3 = 0.0167.
BMI, body–mass index; d-Ab, double positive TPOAb and TgAb; i-TgAb, isolated thyroglobulin antibody; i-TPOAb, isolated thyroid peroxidase antibody; TSH, thyrotropin; UIC, urinary iodine concentration.
Thyroid antibodies and iodine intake
As shown in Table 2, ID was significantly associated with positive subtype antibodies (OR = 1.11 [CI 1.01–1.22] for i-TPOAb; OR = 1.15 [CI 1.06–1.25] for d-Ab), while the prevalence of positive i-TPOAb and d-Ab significantly decreased with increasing iodine intake (p < 0.01). MAI and EI were inversely associated with i-TPOAb positivity (OR = 0.89 [CI 0.81–0.98] for MAI; OR = 0.90 [CI 0.81–0.99] for EI). However, TgAb showed a U-shaped curve, and both ID and EI were associated with a higher prevalence of positive TgAb (OR = 1.10 [CI 1.00–1.22] for ID; OR = 1.10 [CI 1.00–1.22] for EI). The prevalence of positive TRAb was 53.22% for overt hyperthyroidism (n = 2219), 21.97% for subclinical hyperthyroidism (n = 152), and 0.1% for normal controls (n = 657). The prevalence of TRAb was significantly higher in ID subjects than in iodine-sufficient subjects (22.22% vs. 13.59%, χ2 = 26.838, p < 0.0001; Table 3).
Logistic Regression of Positive Thyroid Antibodies and Associated Factors
p < 0.05 for the independent association between positive thyroid antibodies and each factor after adjusting for the remaining factors, family history of thyroid diseases, and body–mass index.
CI, confidence interval; OR, odds ratio.
Prevalence of Thyrotropin Receptor Antibody Positivity in Iodine Deficiency and Iodine Sufficiency
Total sample size was 3028, with 2219 of overt hyperthyroidism, 152 of subclinical hyperthyroidism, and 657 of normal thyroid function.
Prevalence of TRAb: 53.22% in overt hyperthyroidism; 21.97% in subclinical hyperthyroidism, and 0.1% in normal controls.
22.22% versus 13.59%; χ2 = 26.838, p < 0.0001.
TRAb, TSH receptor antibody.
Thyroid antibodies and thyroid function
Compared with the negative antibody group, all subjects in the positive antibody group had significantly higher TSH levels (Table 4). There was a significant association between thyroid antibodies and abnormal serum TSH levels. In the TSH <0.27 mIU/L group, OR for i-TPOAb was 3.05 [CI 2.24–4.14], OR for i-TgAb was 3.64 [CI 2.62–5.05], and OR for d-Ab was 6.27 [CI 4.70–8.35]. In the TSH >4.2 mIU/L group, OR for i-TPOAb was 2.04 [CI 1.88–2.21], OR for i-TgAb was 1.62 [CI 1.49–1.77], and OR for d-Ab was 3.72 [CI 3.49–3.97] (Table 4). Both positive i-TPOAb and i-TgAb were associated with abnormal TSH levels, and d-Ab had a superimposing effect. The prevalence of subnormal TSH levels was significantly associated with higher antibody titers at TPOAb or TgAb >15 U/mL (p < 0.01), and the prevalence of elevated TSH levels significantly increased with antibody titers at TPOAb >15 U/mL or TgAb >34 U/mL (p < 0.01; Fig. 1). Additionally, the prevalence of hyperthyroidism and hypothyroidism was significantly higher in subjects with positive thyroid antibodies than in subjects with negative thyroid antibodies (Supplementary Table S1).
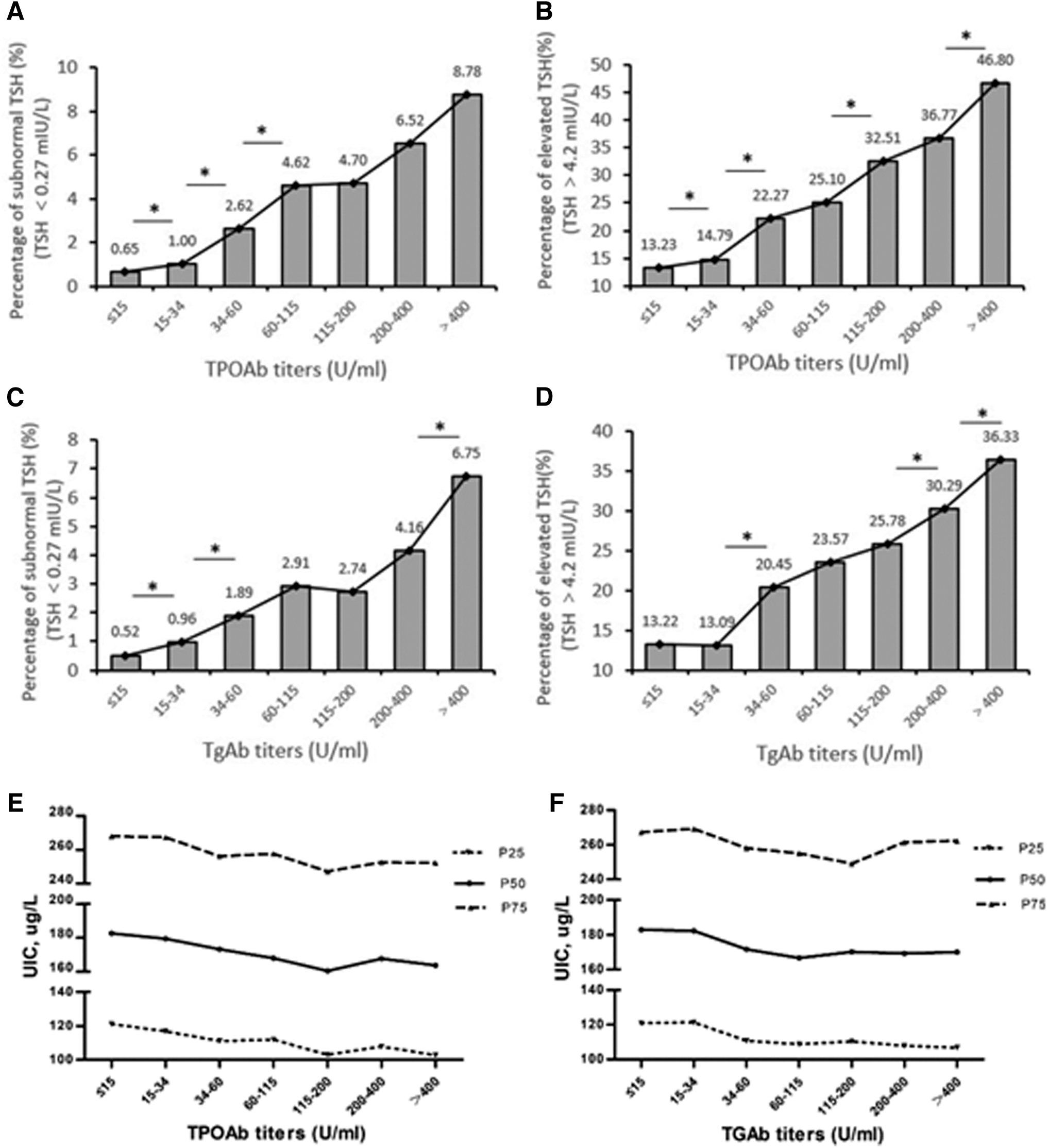
Percentage of abnormal serum TSH and UIC levels stratified by TPOAb and TgAb titers. TPOAb titer levels and percentage of subnormal TSH (
Prevalence of Abnormal Thyrotropin Levels According to Antibody Status
p < 0.05 adjusted for sex, age, UIC, BMI, and TRAb.
p < 0.05 adjusted for sex, age, UIC, and BMI.
Similar letters represent no differences between two groups based on the chi-square test.
Thyroid antibodies and race/ethnicity
Table 1 shows the five races/ethnicities that were represented in this study: Han, Tibetan, Hui, Zhuang, and Uygur. Compared with the Han participants, Tibetans had a lower risk of d-Ab in both sexes (men: OR = 0.50 [CI 0.29–0.86]; women: OR = 0.43 [CI 0.33–0.56]) and Hui participants had a lower risk of i-TPOAb (OR = 0.69 [CI 0.48–0.99]) and d-Ab (OR = 0.68 [CI 0.51–0.91]) in women, but a higher risk for positive i-TgAb in men (OR = 1.64 [CI 1.07–2.50]). Zhuang participants had a higher risk of i-TPOAb in both sexes (men: OR = 1.51 [CI 1.13–2.03]; women: OR = 1.63 [CI 1.31–2.03]), but a lower risk of i-TgAb in men (OR = 0.74 [CI 0.56–0.99]), compared with Han participants. The OR value of i-TgAb in Uygur women was 1.51 [CI 1.23–1.86].
Discussion
Iodine is involved in thyroid hormone synthesis and thyroid gland function. Therefore, iodine intake is closely related to thyroid disease (4). According to the WHO, Iodine Global Network (IGN), and United Nations Children's Fund (UNICEF), iodine deficiency disorders (IDD) have been effectively controlled by USI, and 130 countries have achieved the goal of eliminating IDD (3). However, the relationship between excess iodine and thyroid disease has not been established. In particular, the safety of long-term USI implementation has not been evaluated.
The relationship between excessive iodine and thyroid autoimmunity has not been studied. One view is that excess iodine initiates and aggravates thyroid autoimmunity. Pedersen et al. compared the positive rates of thyroid antibodies before and after five years of iodine supplementation. Median urinary iodine (MUI) increased from 61 to 101 μg/L, the prevalence of positive TPOAb increased from 14.3% to 23.8%, and the prevalence of positive TgAb increased from 13.7% to 17.9% (7). The Pescopagano survey reported that after 15 years of iodine supplementation, MUI increased from 55 to 98 μg/L and positive thyroid antibody increased from 12.6% to 19.5% (8). Similar results have been reported in Slovenia, Poland, Greece, and other countries (9 –11). Studies on NOD.H-2h4 autoimmune mice confirmed that spontaneous thyroiditis and thyroid autoantibodies (mainly TgAb) develop in mice fed high-iodine diets (12). The observed immunogenicity is induced by stereochemical changes to the Tg structure; highly iodinated Tg may have a different confirmation and may be more immunogenic than poorly iodinated Tg (13).
However, some studies suggest that increased iodine intake was not associated with thyroid autoimmunity (2,7,14,15). Epidemiological data from a mildly iodine-deficient population in Tasmania revealed no association between iodine supplementation and thyroid autoimmunity between 1995 and 2013 (15). According to the literature, the prevalence of thyroid antibody positivity ranges between 12% and 26% (16). Even though China has been exposed to 6 years of EI, 10 years of MAI, and 4 years of AI, the prevalence of thyroid autoantibodies has remained low and stable. As an example, TPOAb rates were 9.81% in 1999, 10.64% in 2006, and 11.05% in 2010 versus 10.19% in the present study (Supplementary Fig. S3) (6,17 –19). Furthermore, an inverse relationship between iodine intake and thyroid antibodies was found in this study. The prevalence of TPOAb and d-Ab decreased significantly with increased iodine intake, and MAI and EI became protective factors for antibodies. The findings suggest that MUI at 100–299 μg/L is safe from a thyroid autoimmunity perspective. There are two explanations for this phenomenon. First, China started to implement USI based on the adequate iodine status. Second, during USI, the national standard for salt iodine concentration was reduced twice.
Another major finding of this study was that the prevalence of i-TPOAb, i-TgAb, and d-Ab positivity was highest in the iodine-deficient group (Table 2). The prevalence of positive TRAb was significantly higher in the ID group than in the iodine sufficiency group (Table 3). These results indicate that ID is a risk factor for thyroid autoimmunity.
Thyroid antibodies are closely related to thyroid function; however, the effects of thyroid antibody subtypes are controversial. Huber et al. reported an increase in the incidence of hyperthyroidism in TPOAb-positive patients during follow-up visits; however, there was no statistically significant association between positive TgAb and thyroid function deterioration in patients (20). Hollowell et al. proposed that unlike positive TgAb, positive TPOAb was associated with hyperthyroidism and hypothyroidism. In addition, positive TgAb without TPOAb was not associated with thyroid disease (21). Vanderpump et al. followed up 2779 British community residents, and the risk of hypothyroidism increased with high antibody concentrations in TPOAb-positive women, but not in TgAb-positive subjects (22). Pendersen et al. reported that single positive TgAb was not associated with increased TSH (23). However, in our study, positivity of both TgAb and TPOAb was significantly associated with elevated TSH levels (OR = 2.04 for TPOAb and OR = 1.62 for TgAb), and the two antibodies had an additive effect on thyroid function (OR = 3.72; Table 4).
There are few studies that have explored the relationship between thyroid antibody and the lower limit of the TSH reference range. According to the National Health and Nutrition Examination Survey (NHANES III) in the United States and the health study of Nord Trondelag (HUNT) in Norway, the relationship between the serum TSH level and thyroid antibody positive rate may be “U” shaped. At extremely low and high TSH levels, an increase of the thyroid antibody positive rate was observed, but this is more common at the extremely high TSH level (24,25). This is also reflected in the Nijmegen Biomedical Study in the Netherlands (26). A study from Japan also found that the positive rates of thyroid antibodies in adult patients with subclinical hyperthyroidism and hyperthyroidism were higher than that in euthyroid people (27). However, the reason for the high positive rates of thyroid antibodies in the population with low serum TSH levels has not been effectively explained in these studies.
Four ethnic minorities (Tibetan, Hui, Zhuang, and Uygur) were investigated in the survey. The results varied widely among the five groups. For example, Tibetan and Hui people had low positive rates of thyroid antibodies, while Zhuang people had high positive rates. Within the same ethnic group, the prevalence of the two antibodies varied. For example, Zhuang people had a higher prevalence of positive TPOAb, but a lower prevalence of TgAb, than Han people. The results were consistent with reports from black and white Americans (21). Geography, genetics, and lifestyle might explain the difference. There is also a difference in susceptible gene variation in the comparison of similar studies among Japanese, Chinese, Korean, and European populations (28). A Danish twin study estimated that the genetic influence was 61% on serum TPOAb concentration and 39% in males and 75% in females on serum TgAb concentration (29).
Our study has some limitations. First, the study had a cross-sectional design, hence we cannot determine the causal relationship between iodine intake and thyroid autoimmunity. Second, an epidemiological survey of such massive scale is methodologically challenged by the control of geographical, environmental, and genetic factors, which may influence disease outcomes. Finally, no information was obtained on food composition through the questionnaires.
In conclusion, after two decades of USI, the prevalence of thyroid antibody positivity in China has remained low, indicating that USI is safe for thyroid autoimmunity. With the increase in iodine intake, the prevalence of positive TPOAb decreased significantly. ID is a risk factor for thyroid autoimmunity, while iodine intake between 100 and 299 μg/L is optimal and safe for thyroid autoimmunity. TgAb, like TPOAb, was significantly associated with abnormal TSH levels. The prevalence of thyroid antibodies varied among the five ethnic groups, which may be related to genetic, geographical, and environmental factors.
Authors' Contributions
W.P.T., Z.Y.S., D.T., W.Q.Y., X.G.S., and Y.Z.L. conceived and designed the study. W.P.T. and Z.Y.S. supervised the study. Z.Y.S., W.P.T., D.T., W.Q.Y., and Y.Z.L. performed the statistical analysis. All authors contributed to the analysis and interpretation of data. D.T. and W.Q.Y. drafted the manuscript. All authors approved the final version of the manuscript before submission.
Footnotes
Acknowledgments
The authors thank the participants of this study. For continuous support, assistance, and cooperation, the authors are grateful to Jiang He and Chung-Shiuan Chen (Tulane University); Wei Gong, Chenling Fan, Hong Wang, Hongmei Zhang, Shuangning Ding, Xiaochen Xie, and Tingting Liu (The First Hospital of China Medical University); Caiping Li and Jian Huangfu (The Affiliated Hospital of Inner Mongolia University); Nan Jin (Chinese PLA General Hospital); Wuquan Deng and Fang Deng (Third Military Medical University); Haicheng Zhou (The First Affiliated Hospital of Dalian Medical University); Qingling Lu (Cardiovascular and Cerebrovascular Disease Hospital of Ningxia Medical University); Yunfeng Shen (The Second Affiliated Hospital of Nanchang University); Guodong Liu (The First Affiliated Hospital of Harbin Medical University); Junxiu Hou and Zhiqiang Zhang (The Affiliated Hospital of Inner Mongolia Medical University); Hong Zhang (The Second Xiangya Hospital); Xiaodong Mao, Qifeng Wang, and Kun Wang (Nanjing University of Chinese Medicine); Yanping Wang (Fujian Medical University Union Hospital); Xiaojun Ma (The First Affiliated Hospital of Zhengzhou University); Liheng Meng (First Affiliated Hospital of Guangxi Medical University); Weihua Linle and Tuanyu Fang (Hainan General Hospital); Xingjun Liu and Yanru Zhao (The First Affiliated Hospital of Xi'an Jiaotong University); Lulu Chen, Jiaoyue Zhang, and Hanyu Wang (Huazhong University of Science and Technology); Jingfang Liu and Songbo Fu (The First Hospital of Lanzhou University); Qingguo Lv (West China Hospital); Chenglin Sun (The First Hospital of Jilin University); Qiuming Yao and Ronghua Song (Shanghai University of Medicine & Health Sciences-Affiliated Zhoupu Hospital); Tingting Chen (The First Hospital of An Hui Medical University); Ben Niu (The First People's Hospital of Yunnan Province); Mingtong Xu and Feng Li (Sun Yat-sen Memorial Hospital); Lizhen Lan (The First Hospital of Shanxi Medical University); Jun Yue and Jia Song (People's Hospital of Tibet Autonomous Region); Yanan Li and Wei Luo (Qinghai Provincial People's Hospital); Xiaoming Lou and Zhe Mo (Zhejiang Provincial Center for Disease Control and Prevention); Nianchun Peng and Lixin Shi (Affiliated Hospital of Guiyang Medical University); Mian Wang, Qiuxiao Zhu, and Lingling Yuan (Second hospital of Hebei Medical University); Haiqing Zhang (Shandong Provincial Hospital affiliated to Shandong University); Yong Fan (The First Affiliated Hospital of Xinjiang Medical University); and Hongyan Wei (Tianjin Medical University General Hospital).
Author Disclosure Statement
The authors hereby confirm that no part of this article has been published or is under consideration for publication elsewhere. The authors have no potential conflicts of interest to declare.
Funding Information
This study was supported by the Research Fund for Public Welfare from the National Health and Family Planning Commission of China (Grant No. 201402005).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1