
Abstract
Background:
There is an escalating worldwide population of thyroid cancer (TC) survivors. In addition to conventional metrics of quality of care, quality-of-life (QoL) assessment in TC patients is imperative. TC survivors face unique impediments to health-related quality of life (HRQoL), including thyroid-specific symptoms and exposure to disease-related stressors—including fear of recurrence and financial toxicity—over a prolonged survival period. Survey instruments currently used to assess HRQoL in TC survivors may be insufficient to accurately capture the burden of disease in this population. We aimed to identify the HRQoL instruments in the literature, which have been applied in the TC survivor population, and to present the psychometric properties of the scales and indexes that have been used. We hypothesized that few instruments have shown evidence of validity in this population.
Summary:
Of the 927 articles identified by search criteria, only 28 studies using 15 HRQoL instruments met inclusion criteria. Of the 15 HRQoL instruments identified, 9 were psychometric health status instruments and 6 were preference-based indexes, but none had been validated in the TC survivor population. While the majority of reviewed studies demonstrated impaired psychological and emotional well-being in TC survivors, these findings were not uniformly demonstrated across studies, and the longevity of the impact of TC on HRQoL was variably reported.
Conclusions:
Discrepancies in the literature regarding the impact of TC survivorship on HRQoL emphasize the challenges of accurately assessing patient perspectives, reinforcing the importance of using well-constructed instruments to measure patient-reported outcomes in the target population. Care providers involved in the treatment of TC survivors should be aware of longitudinal effects on HRQoL, especially pertaining to chronic psychological debilitation. Further development and rigorous validation of TC-specific instruments will allow for better data gathering and understanding of the barriers to achieving high long-term HRQoL in TC survivors throughout their long postsurvival course.
Introduction
With the increasing incidence of thyroid cancer (TC), young age at diagnosis, and comparatively low disease-specific mortality, there is an escalating worldwide population of TC survivors (1,2). Assessing survival alone as the key outcome for TC patients is inadequate. In addition to conventional metrics of quality of care, quality-of-life (QoL) assessment in TC patients is imperative. Health-related quality of life (HRQoL) comprised the physical, psychological, social, and spiritual impacts of a disease, as described by Ferrell et al. in their defining qualitative studies of HRQoL in cancer survivors (3 –7).
Assessment of HRQoL relies on information obtained directly from the patient and/or a proxy, termed a Patient-Reported Outcome Measure (PROM). PROMs enable communication of the needs and goals of patients beyond survival, including patient prioritization of QoL versus length of life (8 –10). Measurement of HRQoL can both assess the effectiveness of an intervention and, in some reports, ultimately be correlated with improved survival (11 –13). HRQoL is multidimensional, encompassing symptoms, functioning, and general perceptions of well-being that are challenging to measure objectively (14). Moreover, HRQoL is subjective, personal, and may fluctuate over time and with progression of disease.
Two main methods are used in HRQoL measurement: psychometric health status measurement and utility/preference-based measurement (15). Psychometric measures (such as the short-form 36-item [SF-36]) are derived from patient-reported data regarding the presence, frequency, and intensity of symptoms, combined to generate functional summary scales for domains such as physical and psychological well-being (16).
Numerous psychometric surveys exist and can broadly be categorized as generic, disease-specific, and/or problem-specific. Utility- or preference-based instruments (such as the EuroQol Instrument, or EQ-5D-5L), designed as indexes, are derived from macroeconomics, psychological and decision theory, and are developed for economic analyses by design (17). These values or preferences for states of health, also called “utilities,” are usually generic in scope, meaning they generate health values comparable across different diseases. However, there has been recent interest in disease-specific utility indexes, due to the shortcomings in coverage in generic instruments.
While the accuracy of HRQoL measurement is imperative, the challenges of accurately measuring HRQoL in TC survivors are manifold: TC patients are distinct from survivors of most other cancers in that many patients are relatively younger, otherwise healthy, and most will live with their cancer diagnosis for many years. TC survivors face unique impediments to QoL, including thyroid-specific symptoms and exposure to disease-related stressors—including fear of recurrence and financial toxicity—over a prolonged survival period (18,19). For these reasons, survey instruments currently used to assess HRQoL in TC survivors may be insufficient to accurately capture the burden of disease in this population. Therefore, we aim to identify the HRQoL instruments in the literature, which have been applied in the TC survivor population, and to present the psychometric properties of the scales and indexes that have been used. We hypothesized that few instruments have shown evidence of validity in this population.
Literature Review
A systematic review of the literature was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) method for all peer-reviewed literature published between 1990 and 2018 in both PubMed and Embase. The aim of the search was to identify all studies over the time period, which either used existing instruments or developed HRQoL instruments in TC survivors older than 17 years. Search terms included: thyroid cancer, thyroid carcinoma, thyroid cancer survivors, quality of life, health-related quality of life, thyroid surgery, thyroidectomy, radioactive iodine, post-thyroid surgery, post-radioactive iodine.
Studies were included if they evaluated TC QoL within the adult population (defined as age >17 years) using validated HRQoL instruments. In addition, only instruments that were validated in the language used, and had a description of their development and reported specific psychometric properties, were included. A priori exclusion criteria included previously developed instruments used in a language other than English, and those that did not use all components of a previously validated instrument. Studies that evaluated only specific aspects of TC treatment (i.e., thyroid hormone withdrawal, radioactive iodine treatment, robotic thyroidectomy) or specific aspects of QoL (salivary function, body image) were also excluded. In addition, we excluded all review articles, abstracts, perspectives, and nonpeer-reviewed articles.
Review of all studies was conducted independently by two authors (E.M.R., B.C.J.) and compared for consistency of application of inclusion and exclusion criteria. There was no major disagreement between reviewers regarding application of inclusion and exclusion criteria, and no arbitration was required.
Instruments included in the analysis were categorized as generic HRQoL instruments, cancer-specific instruments, or TC-specific instruments. Instrument characteristics were cataloged in detail, including number of items, domains, domain description, incorporation of Ferrell's QoL domains (physical, psychological, social, spiritual), scaling, scoring, and description of administration instructions (3 –7).
Information on psychometric properties of each instrument was extracted from each study reporting the instrument's use, as well as from studies referenced by the included study. Reliability was reported as poor, moderate, or strong based on Cronbach's alpha (α) measuring internal consistency. We also looked for any evidence of use of Item Response Theory (IRT) calibration of items. Validity was reported as degree of correlation with established QoL metrics. Convergent, divergent, and discriminant validity was noted if reported in original validation studies. Responsiveness was reported as specific changes in health status over which it was observed. Additional collected information included sample size, patient population, reported objectives, study conclusions, instruments used as well as implementation appropriateness, and Ferrell's QoL domains collectively assessed by instruments used in the study.
Results
Studies and instruments
An initial query identified 927 articles based on the search criteria. Of these, 791 articles were excluded by title as they did not concern TC survivorship. Of the remaining 136 articles, 91 were excluded based on the inclusion and exclusion criteria (Fig. 1). Forty-five articles remained for review of their QoL instruments. Five instruments were excluded as they were not validated in the language used in the study, and 12 were excluded due to lack of documented validation. The remaining 28 studies (18,20 –45) utilized 15 QoL instruments for analysis (Table 1). The primary findings of the 28 studies are summarized in Table 2.
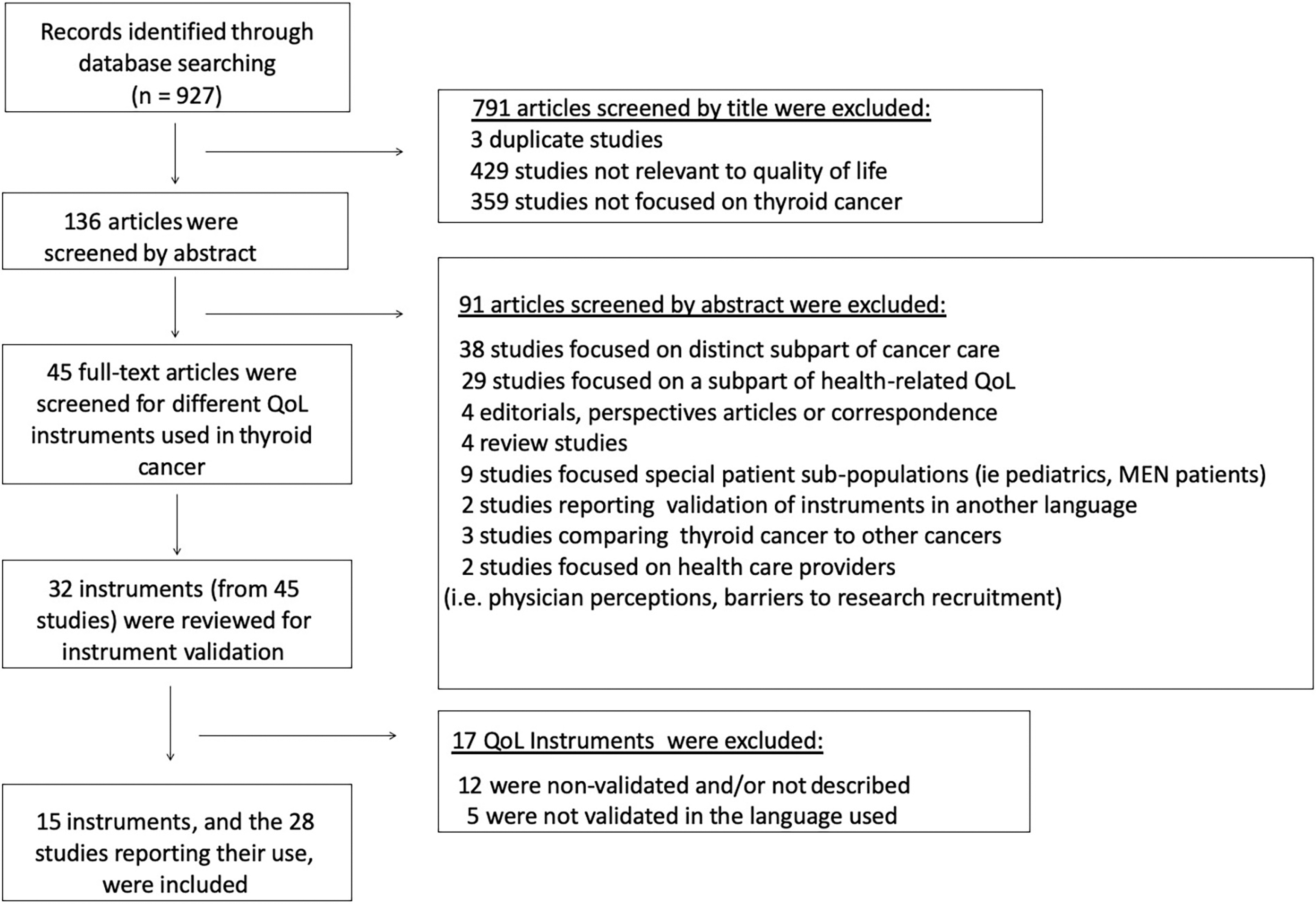
Schematic presentation of methodology used and selection criteria.
Description of Quality-of-Life Instruments Used in Thyroid Cancer Survivors
Blank boxes indicate domain not assessed.
HRQoL, health-related quality of life; N/A, not applicable; QoL, quality of life; TC, thyroid cancer.
Quality-of-Life Studies in Thyroid Cancer Survivors
See Table 1 for disease-specific instrument acronyms.
Qualitative data gathered from study participants were mapped onto elements of SF-6D and EQ-5D by investigators.
40 question version of HUI to be administered by an interviewer.
Survey scores gathered from pre-existing national database.
Functional domains and global scales only, symptom domains excluded.
Scaling and time frame modified to match coadministered EORTC QLQ-C30.
Additional thyroid-specific questions added.
BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; BFI, Brief Fatigue Inventory; DTC, differentiated thyroid cancer; FoR, fear of recurrence; HADS, Hospital Anxiety and Depression Scale; MFI-20, 20-item Multidimensional Fatigue Inventory; NATCSS, North American Thyroid Cancer Survivorship Study; PTC, papillary thyroid cancer; RAI, radioactive iodine ablation; SDQ, Somatoform Disorders Questionnaire; T4, thyroxine; TSH, thyrotropin.
Of these 15 HRQoL instruments identified, 9 were psychometric health status instruments and 6 were preference-based indexes. Importantly, while each of these instruments has been utilized in other cancer types and numerous other disease states, none of them has been validated in TC survivors. The majority of studies (18/28) reported the use of a single HRQoL instrument. Eight studies used two or more instruments, and two studies used three instruments. Half (14) of the studies used cancer-specific instruments, including 9 studies that used TC-specific instruments. Of the four TC-specific instruments identified, only two—COH-QoL and THYCA-QoL—had undergone phase IV testing. Notably, 5 of the 28 reviewed studies made alterations in instrument scaling or administration at the discretion of the investigators, using the instrument in an alternate manner other than that in which it was intended to be used.
QoL in TC survivors
Of the 28 included studies, 17 demonstrated impaired HRQoL in TC survivors compared with age- and sex-matched controls (40), the general population (21,30,34,36,43), or survivors of other types of cancer (34,36,38). Only three studies reported no decrease in HRQoL in TC survivors (41,42,44). Again, none of the instruments used had undergone thorough psychometric testing in TC survivors.
The most frequently reported symptoms related to reduced HRQoL in TC survivors were anxiety (26,27,33,37,44), depression (35,37,44), and fatigue (26,28,33,35 –37,44). Insomnia and sleep disturbances (32,35,36), memory issues, difficulty concentrating, and neuromuscular complaints (21,26,32) were also reported in several studies. Importantly, fear of recurrence was a significant contributor to reduced QoL reported in four studies (18,24,27,32), with one study reporting comparable effects of anticipated and actual disease recurrence on QoL in TC survivors over a decade after diagnosis (18).
Preference-based indexes and their properties
Six preference-based measures were used to assess HRQoL in TC survivors: HUI2, HUI3, EQ-5D-5L, EQ-5D-3L, 15D, and SF-6D. The number of items assessed ranged from 5 to 16. While EQ-5D-5L, EQ-5D-3L, and SF-6D evaluated the physical, psychological, and social domains of HRQoL, HUI2 and HUI3 evaluated only the physical and psychological domains, which is often the case in utility indexes.
QoL evaluation using preference-based indexes
While one study found HRQoL in TC survivors to be comparable with that of the general population at long-term follow-up using 15D (42), all other studies using preference-based instruments found significant impairment in HRQoL in TC patients. Two studies used SF-6D to demonstrate impaired HRQoL in young female adult survivors and patients with advanced differentiated thyroid cancer (DTC), respectively (22,26). While EQ-5D-3L was used in multiple studies to demonstrate decreased HRQoL and increased anxiety and depression in patients with TC compared with other types of cancer (34,38), the ability of SF-6D to more comprehensively capture the HRQoL effects of DTC than other preference-based indexes has been demonstrated (22,28).
Psychometric instruments and their properties
Psychometric instruments used in the assessment of HRQoL in TC survivors demonstrated a variety of scoring metrics and assessed a range of symptoms and behaviors. The number of domains ranged from 4 to 10. The number of items assessed ranged from 12 to 58. All instruments were designed to be self-administered in a one-time sitting. Only two instruments evaluated all four of Ferrell's QoL domains (physical, psychological, social, and spiritual) (33,46). Five psychometric instruments evaluated three of the domains—SF-12, SF-36, PROMIS-29, EORTC QLQ-C30, and UW-QoL; each excluded the spiritual domain. Finally, two instruments evaluated two domains (physical and psychological) (45,47). Four instruments were designed to evaluate TC-specific HRQoL (33,45 –47).
Cancer-specific psychometric instruments and their properties
The psychometric properties of the six reported cancer-specific instruments—including TC-specific instruments—varied in the strength of their validation metrics (Table 3). All instruments reported internal consistency of Cronbach's a > 0.7 in the majority of scales, with the exception of ThyCAT for which reliability was not reported (33,45 –50). Validity measures were reported in five of six instruments. THYCA-QoL reported convergent validity for five out of seven scales, but poor correlation (r < 0.4) with EORTC QLQ-30. Responsiveness across treatment course was reported only for UW-QoL, which measured responsiveness in both tumor stage and treatment course (50). All instruments were also evaluated for IRT calibration of individual items. No study had included documentation of IRT calibration, although the PROMIS-29 items were calibrated with IRT methods when this generic instrument was created (51).
Psychometric Properties of Cancer-Specific Quality-of-Life Instruments Used in Thyroid Cancer Survivors
α = Cronbach's alpha (internal consistency, a > 0.7); r = correlation coefficient.
Validated in patients undergoing chemotherapy.
Validated in patients with nonresectable lung cancer.
Validated in head and neck cancer.
Validated in thyroid patients undergoing T4 withdrawal.
FACT-G, Functional Assessment of Cancer Therapy-General; KAF, Karnofsky Performance Scale; NATCSS QoL, North American Thyroid Cancer Survivorship Study Quality of Life; SIP, Sickness Impact Proflie.
QoL evaluation using psychometric instruments
Several studies using psychometric instruments examined the impact of age and life stage on HRQoL in TC survivors, demonstrating decreased HRQoL in various subpopulations, including patients older than 50 years (39) and young female patients (23,26) using both preference-based indexes and THYCA-QoL. Multiple studies using THYCA-QoL demonstrated reduced physical impairment, but worse psychological symptoms and overall HRQoL, in younger TC survivors when compared with older survivors (26,35).
Summary
As the incidence of TC increases and the population of survivors expands, understanding of the impact of TC diagnosis and treatment on QoL has become increasingly important. There are currently over 50,000 patients diagnosed with TC in the U.S. annually (52). As this cancer is largely a nonlethal disease, there is a rapidly rising population of TC survivors for whom optimizing QoL is of paramount importance.
This demand for optimizing QoL has taken on two dimensions. First, and more established, this patient demographic has generated a shift toward increasingly conservative treatment with reduced radioiodine use and thyroid hormone for thyrotropin suppression and less aggressive surgical intervention. With changes in clinical practice thus being shaped by attention to patient priorities, it is imperative that this patient population undergoes a detailed analysis of QoL as it relates to both treatment and monitoring.
The second dimension—which is relatively new and still emerging—is the emphasis not only on assessing short-term physical side effects of treatment but on longitudinal data regarding the emotional, psychological, and social impacts of carrying a cancer diagnosis throughout a normal life expectancy as well. The majority of instruments used to evaluate HRQoL in TC survivors focus on the physical, psychological, social, and spiritual QoL domains as outlined by Ferrell et al. in the evaluation of QoL in breast cancer survivors (5). In their validation of a breast cancer QoL model, Ferrell et al. conducted a qualitative interview and survey-based study of 21 breast cancer survivors, and derived themes of HRQoL impairment within these four domains (6,7). While results demonstrated significant physical and psychological burden in breast cancer survivors, several aspects of spiritual well-being were shown to be positively impacted by survivorship.
Of note, only two instruments reviewed in the present study address Ferrell's spiritual domain of HRQoL. Spiritual well-being, defined as the ability to maintain and derive meaning from the cancer experience (4), is a core component of the overall assessment of HRQoL for some and has been shown to have a direct correlation with health outcomes (53). As changes in one domain can impact and influence the evaluation of all four domains, exclusion of this domain in the evaluation of TC QoL might result in an incomplete understanding of QoL survivorship using a psychometric approach. Utility indexes, in contradistinction, which are by nature designed for structural independence (i.e., no double counting), may show an impact by spiritual items on other domains (e.g., anxiety). Furthermore, because spirituality may be difficult to define, it may be difficult to measure it alone and in terms of its effects.
Many of the studies reviewed here demonstrated impaired psychological and emotional well-being in TC survivors, with anxiety, depression, and fatigue commonly cited as contributors to decreased HRQoL in these patients. Several studies suggested that younger patients are especially likely to be negatively affected by these symptoms, and that fear of recurrence can be significantly detrimental to QoL up to decades after diagnosis. However, these findings were not uniformly demonstrated across studies. The impact of TC on HRQoL varied widely; while a small number of studies demonstrated no long-lasting HRQoL detriments in TC survivors compared with the general population (41,42,44), others reported comparable or worse HRQoL to other cancer types with significantly worse prognoses (34,36,38)—a finding previously demonstrated by others (54).
Notably, several studies suffered from varying degrees of selection bias. Utilization of patient samples from survivorship groups is likely to overestimate HRQoL impact of TC, as patients may be more likely to join survivorship groups if they experience QoL issues, making the results less generalizable to the entire population (22,34). Other studies may have suffered from selection bias by surveying exclusively long-term survivors, who may have been more likely to respond if they were experiencing persistent symptoms after definitive treatment (24,29).
Nonetheless, the marked discrepancies demonstrated in the findings of these studies emphasize the challenges of accurately assessing patient perspectives, reinforcing the importance of using well-constructed instruments to measure patient-reported outcomes in the target population, including not only the physical and psychosocial impact of diagnosis and treatment but also the financial toxicity associated with the disease. To date, the financial component of QoL has been largely underappreciated. Ramsey et al. evaluated the bankruptcy rate associated with various cancer types, showing a bankruptcy rate of 9.3 per 1000 person-years (55). While the etiology of this finding is not fully understood, recognition that financial toxicity likely impacts QoL in TC survivors should prompt researchers in this field to incorporate this domain into future instruments (56).
The use of instruments in disease-specific QoL assessment requires a thorough understanding of how the instrument was developed and the intended use for it. Most importantly, such tools must be reliable and responsive to the domains of life quality being assessed, thus relevant to the disease being evaluated. TC patients have disease-specific QoL changes that may differ from other cancer types. Thus, the population being evaluated must be similar to the population in which the tool was developed and should be used in the same language in which the tool was developed.
The decision to use generic instruments versus disease-specific instruments has specific advantages and disadvantages. Generic instruments are most often supported by strong validation across numerous populations, but if not validated specifically in the target population being evaluated, they may fail to detect disease-specific QoL changes that have significant effects on that population. This review identified no instruments that have undergone thorough validation of psychometric properties in the TC population, although many of the instruments used to assess HRQoL in this population have been well-validated in other populations.
Because TC survivors face unique HRQoL concerns, these generic instruments are neither comprehensive in their assessment of symptoms nor completely relevant in the HRQoL content they address, and may be poorly responsive to treatment effects. For example, many TC survivors are relatively young at the time of diagnosis; the prolonged survival period they face, although prompting their cancer diagnosis to be labeled as “the good cancer,” in fact increases their susceptibility to long-term financial vulnerability and anxiety (16,19,20,22,43). The usual list of symptoms measured in standard PROMs is inadequate in TC, as it fails to identify and measure the key health and nonhealth contributors to clinical anxiety, including prolonged fear of recurrence and financial toxicity. Recent research has demonstrated the magnitude and prevalence of psychological financial hardship in TC survivors, emphasizing the need for tools and further studies to better understand its impact (57).
In the current literature, assessment of HRQoL in TC survivors has relied heavily on general HRQoL instruments that have not been validated in the TC population. Although instruments designed to assess QoL in cancer survivors exist, only two—EORTC QLQ-C30 and the UW QoL—have been applied to studies of HRQoL in TC survivors. Few instruments are available that specifically assess QoL in TC; all are included in this review. The City of Hope—Thyroid Version instrument developed by Dow et al. is the oldest instrument, developed in 1997 to evaluate QoL in patients undergoing thyroxine withdrawal before scanning procedures (46). The THYCA-QoL developed by Husson et al. was the first rigorously validated instrument, designed for use in combination with the EORTC QLQ-C30 for holistic assessment of HRQoL in TC survivors (45). Singer et al. developed the EORTC QLQ-THY from the EORTC QLQ-C30 general cancer instrument, and it is currently undergoing phase IV testing (47). Most recently, Aschebrook-Kilfoy et al. developed the ThyCAT, a computerized adaptive test, using questionnaire response data from a longitudinal cohort study of QoL in 1078 TC survivors in the North American Thyroid Cancer Survivorship Study (33).
Of these four thyroid-specific instruments, phase IV testing has been completed in only three instruments. Rigorous evaluation of psychometric properties has shown acceptable validity and reliability in three instruments; responsiveness has not been demonstrated in any of the four instruments. Responsiveness, defined as the measurement of longitudinal validity or the ability to capture change in health status over time (58,59), is a critical component of QoL assessment.
The identification of subtle changes in HRQoL is an important component of survivorship evaluation and may be influenced by treatment and monitoring approaches. A static evaluation of HRQoL misses the natural and variable progression of patient survivorship over time, and studies that have evaluated HRQoL and instrument responsiveness longitudinally, as performed by Lubitz et al., are rare (28). The ability to detect these changes in the HRQoL of TC survivors is especially important, as the long-term persistence of mood symptoms and fear of recurrence has been demonstrated in several studies, but may not be accurately captured by nonthyroid-specific HRQoL instruments (28).
In general, psychometric, nonpreference-based instruments have traditionally been constructed with the methods of Classical Test Theory (CTT). In CTT, reliability and validity at the level of the scale as a whole are of importance with summated scoring usually used in a unidimensional instrument. However, CTT has been found to have substantial limitations, since it does not emphasize the proper structure of the items. Individual items can be fraught with problems in their construction, which cause measurement issues.
IRT, on the contrary, plots the behavior of items as a logistic function where, by the slope and breadth of the function, one can see how well an item discriminates different levels of a construct as well as showing where the item best functions to detect patients with lower versus higher degrees of a construct (i.e., pain, fatigue, anxiety). IRT then shows how well an item functions in a population and where the patient's level of morbidity or “location” is with respect to that item. Furthermore, CTT does not look at the structure of the response set of an item. For example, in an item about pain, a response set (e.g., none, somewhat, moderate, severe, extreme) may confuse patients in our efforts to differentiate their level of pain.
IRT analysis can show that the item characteristic curves generated for each level of pain are not a monotonic function with increasing severity, so that the item level curves are distorted. For example, data may show that a patient is more likely to endorse a (higher) “moderate” level of pain rather than (lower) a “somewhat” level. IRT can also evaluate situations where an item is not performing equally in different groups when it should, say in different sex or ages, because of the language used (differential item functioning). Finally, IRT can establish relative “invariant measurement” for an item for use in any TC population once it shows good performance in a reasonably sizeable TC population.
This study has several limitations. Inclusion and exclusion of studies, as well as assessment of validation metrics, were dependent on methodology reported by the authors. Only those studies explicitly documenting or providing references for tool validation or specific assessment of psychometric properties were included and reported as such in this review. Notably, the studies included for review were heterogeneous in nature: while many assessed HRQoL of TC survivors in comparison with the general population, others simply reported stages of instrument development and validation or assessed correlation of validated instrument domains with patient focus groups. With so few studies meeting the inclusion criteria, the authors allowed for this heterogeneity to more comprehensively review the HRQoL instruments available for use in the TC patient population, with the understanding that these instruments were being applied in a variety of ways across studies. There was no major disagreement between independent reviewers regarding the application of inclusion and exclusion criteria to individual studies.
Taken together, the results of this study indicate a need for development and a thorough validation of a standardized HRQoL assessment tool for TC survivors, using a complete and rigorous developmental process as described above using IRT and CTT methods as appropriate. Critical in such an instrument would be the capability to function as a preference-based index, either by a valuation process to use all of the chosen items or a proper subset of more conceptually nonredundant psychometric items.
Given the substantial financial ramifications of TC care for both patients and the health care system, a view toward cost-effectiveness is reasonable. A usual concern with disease-specific instruments is that the quality-adjusted life years (QALYs) generated will not be conceptually similar to the QALYs generated by generic indexes—thus not comparable across diseases.
Prior work by the National Health Measurement Study showed that in factor analysis, all generic indexes have three basic factors/domains: Pain, Physical, and Psychosocial (60). The psychosocial domain often emphasizes psychological aspects over social, since many feel the index-based domains should only be aspects “within the skin,” noted by the HUI2/3. Such an approach usually eliminates social aspects. If a proposed index has coverage of these three areas, then the QALYs that result are likely valid and are arguably more valid than a generic tool. An optimal tool would adequately cover TC QoL, given the differences in treatment, prognosis, and HRQoL impact of DTC compared with other cancer types, but therefore scaled so that the QALYs are meaningful.
Evaluation of the effects of definitive treatment on HRQoL should reflect current shifts in clinical practice toward conservative treatment approaches. Assessment of necessary QoL domains and sensitivity to the longitudinal impact of psychological stressors (including fear of recurrence) are essential to accurately understand the burden of TC survivorship.
Conclusions
This review identifies the HRQoL instruments in the literature, which have been used in TC survivors, and summarizes their psychometric properties. We also systematically review the current literature and evaluate published studies using HRQoL instruments in TC survivors. Care providers involved in the treatment of TC survivors should be aware of longitudinal effects on HRQoL, especially pertaining to the various components that contribute to chronic psychological debilitation, to most effectively monitor symptoms and guide care. Further development and rigorous validation of TC-specific instruments will allow for better data gathering and understanding of the barriers to achieving high long-term HRQoL in TC survivors throughout their long post-treatment survival course.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by NIH/NCI-R37CA231957 (CCL).