
Abstract
Background:
Serum Ca19.9 positivity is a prognostic factor for mortality in patients with advanced medullary thyroid cancer (aMTC), independently from calcitonin doubling time (DT). However, it is unknown whether aMTC patients who become positive for Ca19.9 also have progressive disease (PD) according to response evaluation criteria in solid tumors (RECIST) and whether Ca19.9 DT has a role in the management of aMTC patients. The aims of this study were to evaluate whether in aMTC, when serum Ca19.9 becomes positive, PD develops, and to determine the role of Ca19.9 DT in predicting mortality and PD.
Patients and Methods:
Serum Ca19.9 was periodically measured in 107 aMTC patients, and the DTs were calculated. Restaging of the disease was radiologically performed in 104 of 107 patients and PD was evaluated according to RECIST.
Results:
At the end of follow-up, 25 of 107 patients were Ca19.9 positive and PD was identified in 30 of 104 patients. No significant association was found between Ca19.9 positivity and PD, while there was a significant association between Ca19.9 positivity and mortality (p < 0.0001). Ca19.9 DTs <6 months and <1 year were not associated with PD but were associated with mortality (p < 0.0001 and p < 0.0001, respectively). In particular, 3 patients who had a Ca19.9 DT <6 months with no evidence of PD according to RECIST died of their disease after 6, 5, and 3 months, respectively.
Conclusions:
Serum Ca19.9 positivity and DTs <6 months and <1 year are prognostic factors for mortality but not for PD. Serum Ca19.9 positivity and DTs <6 months and <1 year should be considered in the decision-making process of whether to initiate systemic therapy even if there is no evidence of PD according to RECIST.
Introduction
Medullary thyroid cancer (MTC) is a neuroendocrine tumor that secretes several markers. The clinically important markers are calcitonin (Ct), chromogranin A, and carcinoembryonic antigen (CEA) that are secreted into blood or can be identified by immunohistochemistry in tumor tissue (1,2).
In MTC patients, while the increase of serum Ct and CEA levels suggests the progression of disease (PD), serum chromogranin A is less specific and is not useful in clinical practice (3).
Recently, it was demonstrated that, in addition to the mentioned markers, MTC also secretes carbohydrate antigen 19.9 (Ca19.9). In 2015, Milman et al. (4) found that Ca19.9 was positive in 63% of MTC tissue samples by immunohistochemistry, and that the Ca19.9 positive tumors were significantly larger than the Ca19.9 negative group. Positive Ca19.9 immunohistochemistry was also significantly associated with stage IV disease. In a recent study (5), we demonstrated that Ca19.9 was present in 40% of tissue samples in advanced MTC (aMTC) samples and in 16% of the sera in the same group of patients. The hypothesis that Ca19.9 might be relevant, not only in gastroenteropancreatic neoplasia, but also in MTC patients, derived from the observation of two peculiar cases of MTC, occurred in a young male with multiple endocrine neoplasia (MEN) 2A and in a woman with MEN 2B who had very high levels of serum Ca19.9 and both rapidly died from the disease despite a relatively low tumor burden (6,7).
On the basis of these studies, Ca19.9 has been proposed as a prognostic factor for mortality in aMTC independent of serum Ct levels (5). Another study by Alencar et al. (8) was recently published, confirming the prognostic role of Ca19.9 in aMTC patients. Although the role of Ca19.9 positivity was demonstrated in aMTC patients, no information about the role of this marker in predicting the biological behavior of MTC in terms of PD has been provided so far.
The aims of this study were to evaluate change in serum Ca19.9 values during the follow-up of aMTC to calculate its doubling time (DT) and establish whether change in Ca19.9 levels and/or its DT have a role in predicting PD.
Patients and Methods
We retrospectively studied 107 consecutive patients [46 females (43%)], referred to the Endocrine Unit of the Department of Clinical and Experimental Medicine of Pisa University Hospital for the evaluation of advanced structural persistent/recurrent MTC, from 2011 to 2017. In particular, only patients with the presence of local disease and/or metastatic lymph node and/or distant metastases and with more than one measurement of Ca19.9 were included in the study. The mean age at diagnosis of MTC in the study group was 45.9 ± 15.1 years (standard deviation [SD]) (median age: 45.5 years; range 13–79 years).
Ca19.9 was routinely measured during each clinical evaluation, every 6–12 months, from 2011, when we observed a peculiar case of aMTC and high levels of Ca19.9 (6), to 2017. In 23 of 107 patients, the first measurement of this marker was performed retrospectively on a stored blood sample collected between 2006 and 2010. For this reason, the mean follow-up period of Ca19.9 trend was 4.4 years ±2.3 (median: 5 years; range: 0.5–11 years). However, when considering the time of diagnosis, the mean follow-up of the study group was 11.79 years ±7.2 (median age: 45.5 years; range 13–79 years).
The mean number of Ca19.9 measurements for each patient was 5.2 ± 2.09 (median: 5; range: 2–10). Assessment for PD was performed in 104 of 107 patients (3 patients had only 1 computed tomography [CT] scan, thus a comparison to establish PD was not possible).
Ninety-one out of 107 patients underwent total thyroidectomy, central compartment lymphadenectomy, and lateral cervical lymph node dissection (23 right lateral cervical lymphadenectomy, 24 left lateral cervical lymphadenectomy, and 44 bilateral lateral cervical lymphadenectomy). Five patients underwent total thyroidectomy and central lymph node dissection while 11 of 107 patients underwent total thyroidectomy only.
According to the mentioned “inclusion criteria,” at the time of the selection of the patients, 28 of 107 patients (26.2%) had lymph node metastases, 67 of 107 (62.6%) had both lymph node and distant metastases, and 12 of 107 (11.2%) patients had only distant metastases.
All 107 patients were tested for germline RET mutation and 17 of them (15.8%) were positive for a germline mutation.
The study was approved by our institutional reviewing board and all patients gave written consent to participate in the study. No Clinical Trial Registration number is available for this study.
Biochemical and radiological procedures
The biochemical evaluation of the study group included the measurements of serum Ca19.9 (ELECSYS CA19.9; Roche Diagnostics, Indianapolis, IN; normal range <37 U/mL). The same laboratory and the same assay were used for the Ca19.9 measurement during the study period.
Ca19.9 DTs were calculated according to the American Thyroid Association (ATA) guidelines (9), and the ATA website calculator was used (
For the Ca19.9 DTs, we used <6 months and <1 year consistent with previous studies in the literature looking at the prognostic role of Ct and CEA DTs (10 –12).
Neck ultrasonography was performed during each examination along with biochemical and clinical evaluation. In addition, to restaging patients, CT scan was performed every 4–6 months. In patients with only local or cervical lymph node metastases, CT scan was performed when a consistently rising Ct and/or CEA levels were found (9). CT scans were performed with intravenous infusion of iodinated contrast medium with arterial and venous phases. Bone scintigraphy was performed when there was a clinical suspicion of bone lesions and additional evaluation of bone lesions was obtained using magnetic resonance imaging. Magnetic resonance imaging was also used whenever necessary to detect or follow liver lesions. To evaluate for PD, the response evaluation criteria in solid tumors (RECIST) version 1.1 was used (13).
Statistical analyses
Data are presented as mean ± SD, median (interquartile range), or as frequency (percentage), when appropriate. The chi-squared test was used to assess association between categorical variables. Survival curves for mortality were calculated using the Kaplan–Meier method and the statistical significance between groups was assessed using the log-rank test. A p-value <0.05 was considered statistically significant. Statistical analyses were performed in SPSS (version 21.0; IBM Corp., Armonk, NY).
Results
Ca19.9 positivity and DT at the end of follow-up
At the beginning of our follow-up period, 99 of 107 aMTC patients (92.5%) were Ca19.9 negative, while 8 of 107 (7.5%) patients were Ca19.9 positive. At the end of the follow-up period, 82 of 107 patients (76.6%) were still negative, 17 of 107 (15.9%) patients who were initially negative became positive, and all the 8 cases (7.5%) who were Ca19.9 positive initially remained positive. At the end of the observation, a total of 25 of 107 patients were Ca19.9 positive (23.4%). The trend in Ca19.9 positivity is summarized in Figure 1.
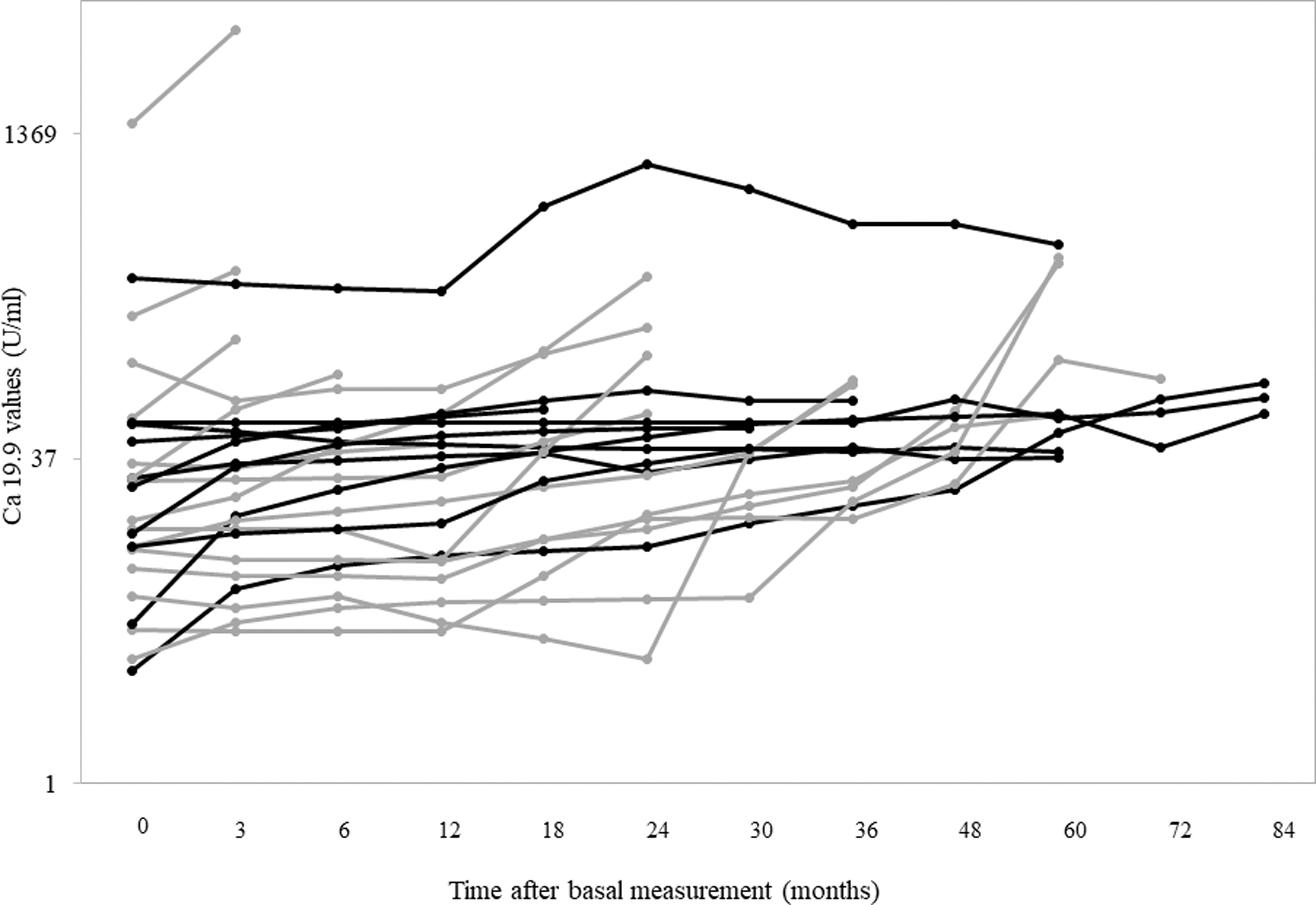
Ca19.9 trend in patients with Ca19.9 positivity at the end of follow-up (gray lines: dead patients; black lines: alive patients).
At the end of follow-up, Ca19.9 DT was <6 months in 6 of 107 patients (5.6%) and <1 year in 9 of 107 patients (8.4%).
Association between Ca19.9 DTs and distant metastases
At the end of our study period, 21 of 107 patients (19.6%) had bone metastases, 44 of 107 (41.1%) patients had liver metastases, and 50 of 107 (46.7%) patients had lung metastases. During the time of follow-up, 12 of 107 patients (11.2%) developed bone metastases. Among them, 2 of 12 (16.7%) patients were already Ca19.9 positive at the beginning of the study, 3 of 12 (25%) patients became Ca19.9 positive, and 7 of 12 (58.3%) patients remained Ca19.9 negative. Thirty-one of 107 patients (29%) developed liver metastases during follow-up. Among them, 3 of 31 (9.7%) patients were initially Ca19.9 positive, 9 of 31 (29%) patients became Ca19.9 positive, and 19 of 31 (61.3%) patients remained negative. Twenty-nine of 107 patients (27.1%) developed lung metastases. Among them, 2 of 29 (6.9%) patients were initially Ca19.9 positive, 11 of 29 (37.9%) patients became Ca19.9 positive, and 16 of 29 (55.2%) patients remained negative.
No significant association was found between the development of distant metastases during follow-up and Ca19.9 positivity (p = 0.27). However, a significant association was found between Ca19.9 DTs both <6 months and <1 year and the presence of bone metastases at the end of follow-up (p < 0.0001 and p = 0.0002, respectively) but not with liver and lung metastases (p = 0.21 and p = 0.66 for liver metastases; p = 0.84 and p = 0.19, for lung metastases, respectively).
Association between Ca19.9 positivity and either mortality or PD according to RECIST
During the study period, 31 patients died of their disease. In particular, 15 of 25 (60%) Ca19.9 positive patients died while only 16 of 82 patients (19%) who were Ca19.9 negative died (p < 0.0001). As shown in Figure 2, the rate of mortality was significantly higher in Ca19.9 positive patients with respect to that of patients with normal values of Ca19.9 (p < 0.001). At the end of follow-up, PD was present in 30 of 104 (28.8%) patients and 74 of 104 (71.2%) aMTC patients had stable disease. There was no statistically significant difference in PD in the Ca19.9 positive and negative subgroups of patients (p = 0.11).

Survival curves in Ca19.9 positive and Ca19.9 negative patients. The difference was statistically significant (p < 0.001).
Association between Ca19.9 DTs <6 months and <1 year and mortality and PD according to RECIST
Both Ca19.9 DT <6 months (exact odds ratio [OR] = 23.5) and Ca19.9 DT <1 year (exact OR = 40.6) were associated with mortality (p < 0.0001 for both DTs). In particular, when Ca19.9 DTs <6 or >6 months were considered, 6 of 6 patients (100%) and 25 of 101 patients (25%), respectively, died of their disease. When Ca19.9 DTs <1 or >1 year were considered, 9 of 9 patients (100%) and 22 of 98 patients (22%), respectively, died of their disease. Figure 3 shows survival curves in the study cohort according to Ca19.9 DTs (<6 and >6 months in panel A and <1 and >1 year in panel B).
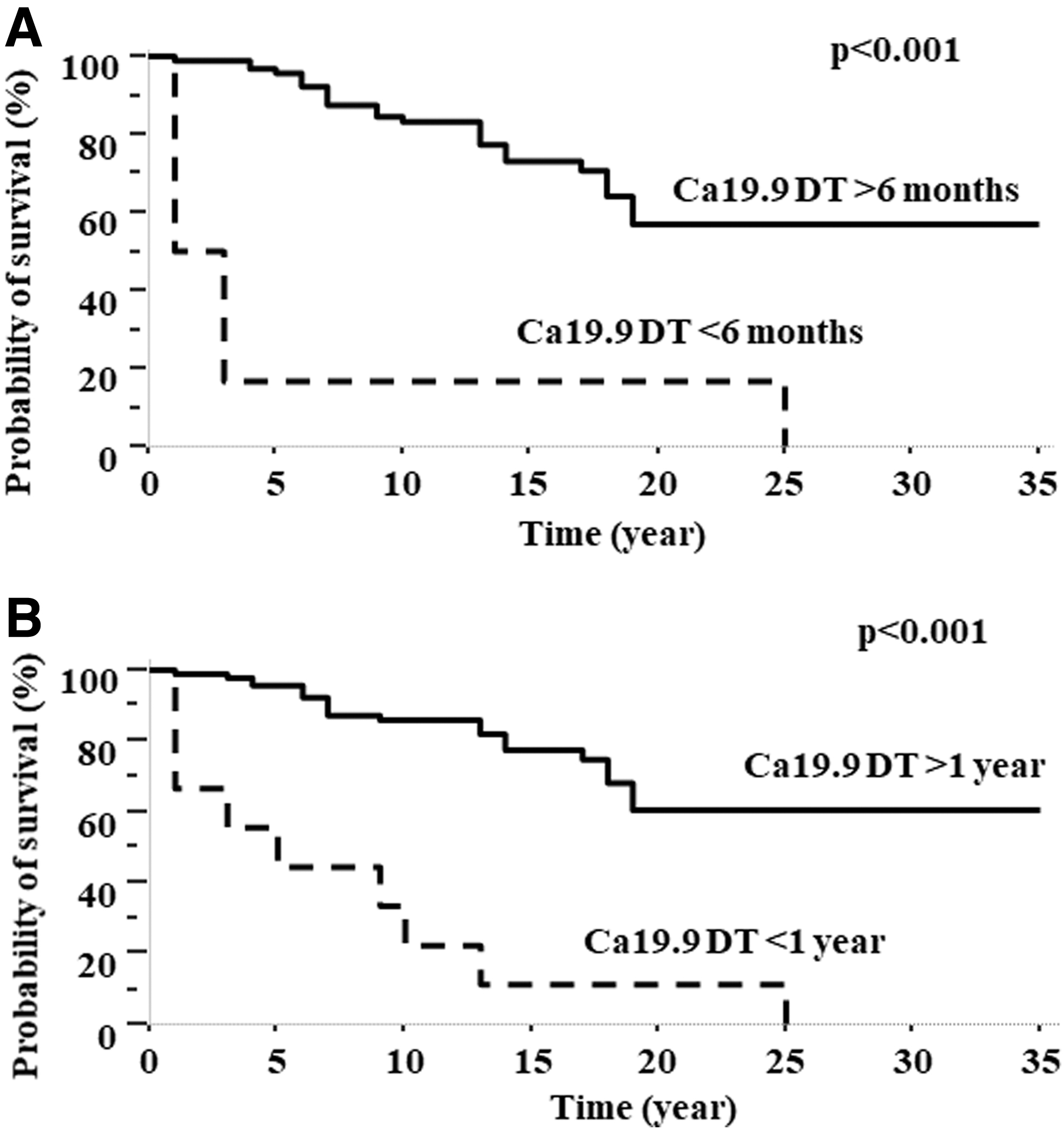
Survival curves in patients according to Ca19.9 DT <6 months (
Although both Ca19.9 < 6 months and <1 year were associated with mortality, neither Ca19.9 DT <6 months nor DT <1 year was associated with PD (p = 0.57 and p = 0.4, respectively). PD was identified in 2 of 5 patients (40%) with Ca19.9 DT <6 months and in 28 of 99 patients (28.3%) with Ca19.9 DT >6 months. PD was identified in 3 of 7 patients (43%) and in 27 of 97 patients (27.8%) for Ca19.9 DTs <1 or >1 year DTs, respectively. However, 3 patients who had a Ca19.9 DT <6 months with no evidence of PD died of their disease after 6, 5, and 3 months, from the time of increasing levels of Ca19.9.
Discussion
In a previous study, we demonstrated that serum Ca19.9 positivity is able to identify a subgroup of aMTC patients with high Ct and CEA levels, with a Ct DT shorter than 6 months and with a higher probability to die in a shorter period of time when compared with Ca19.9 negative cases (5).
Although this study demonstrated the ability of serum Ca19.9 to predict mortality in patients with aMTC with aMTC, no information regarding the association of Ca19.9 serum values, and, in particular, of its DT, with the evidence of PD according to RECIST was studied. Moreover, in the previous study it was impossible to study the precise moment when patients became Ca19.9 positive because the study was conducted analyzing only one blood sample and only one value of Ca19.9. In this study, we selected a group of aMTC patients with the same clinical features as those participating in the previous study with structural disease identified with radiological imaging and two or more Ca19.9 serum samples. Using these two inclusion criteria, the identification of structural PD and the measurement of Ca19.9 DTs were possible and comparable.
We confirmed that serum Ca19.9 positivity, at the end of follow-up, was present in ∼23% of aMTC patients. This prevalence was higher than that previously found in another series of our patients (5). Also in this longitudinal study, this marker was confirmed to be associated with mortality and with the development of bone metastases. However, Ca19.9 positivity was found in only eight patients at the beginning of the follow-up period and its percentage increased during follow-up. This means that, in predicting mortality, the use of Ca19.9 positivity, established in one single measurement may have some limitations that can be overcome by using multiple measurements during follow-up and its DT.
The prognostic role of Ct and CEA, and in particular of their DTs, is very well established (10 –12). It is known that the positivity of these two markers is related to a greater tumor burden and high levels of serum Ct and/or CEA are suggestive of metastatic disease. Moreover, the shorter DTs are predictive of patients' outcome and, if we exclude the very rare undifferentiated MTC characterized by low levels of Ct (14), their determination may be helpful in selecting a therapeutic strategy. According to our results, this is not the case for Ca19.9 since its positivity is not correlated with the tumor burden, as assessed by conventional imaging (6,7), and its DT is not always predictive of PD according to RECIST.
The absence of this correlation led us to posit that some limits in the use of RECIST are present to define PD in some aMTC patients. In fact, to establish the tumor response, the RECIST criteria, not well recognized in clinical practice but usually used in clinical trials, consider only the major diameters of the well-identified target lesion(s). Moreover, the RECIST criteria to define PD are very strict, since they require an increase of >20% of the sum of the greatest diameters of target lesion(s). In 2017, Sabra et al. (15) published a study on PD of papillary thyroid cancer, demonstrating the better clinical utility of the assessment of tumoral volume instead of the sum of the largest diameters used for RECIST. Since the metastatic nodules have an ellipsoid shape, these authors calculated the tumor volume by using all the three dimensions of the nodule, and the DT of this volume was more helpful to identify the time to start systemic therapy. It would be interesting to assess PD with the volume formula method proposed by Sabra et al. (15), and to evaluate whether lesion volume PD correlates with Ca19.9 positivity and/or its DT. In this study, we could not perform this analysis since the necessary data to assess tumor volume were not available.
The observation that the 3 patients with Ca19.9 DT <6 months and no evidence of PD all died of their disease in a very short time (6, 5, and 3 months, respectively) is greatly suggestive of the strong predictive role of Ca19.9 DT for death without evidence of PD. The hypothesis to explain the difference between the strong association of Ca19.9 DTs with mortality but not with PD is that, in these cases, the PD is not macroscopic and thus not detected by imaging and RECIST. We speculate this may be due to a diffusion of micrometastases, not detected on CT scan, that is responsible for the cancer-related death, as demonstrated by the autopsy of the patient with MEN 2A and high serum Ca19.9 level, who rapidly died of their disease (6). In particular, this patient only had a small cervical lymph node metastasis, a small liver lesion, and a few bone lesions, in addition to bilateral pheochromocytoma, and, at the time of death, radiological imaging excluded PD. However, autopsy revealed a massive microscopic progression of the disease, since neoplastic microemboli were present in all organs and caused multiorgan failure and the death of patient. In the same way, in our study, the subgroup of patients with aMTC and Ca19.9 positivity who died without evidence of PD according to RECIST could have had the same phenomenon. This is rather difficult to conclusively demonstrate since we would need a large series of autopsy findings of similar types of aMTC patients. However, with the use of new diagnostic tools, such as positron emission tomography-CT with fluoro-dopa (16,17) or, maybe in the future with 111In-CP04 (18), the metabolic active areas could be identified even if microscopic and not detected with conventional radiological imaging techniques.
In conclusion, we demonstrate the utility of serum Ca19.9 to identify a subgroup of aMTC patients with a greater probability of dying of their disease. Ca19.9 DT <6 months can identify those patients who will rapidly die of their disease despite the absence of an evidence of PD according to RECIST. Our findings suggest these patients should probably be immediately treated with systemic agents such as cabozantinib (19) or vandetanib (20) or other systemic therapies if available (21,22), without awaiting for the evidence of PD according to RECIST.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study has been supported by Associazione Italiana Ricerca sul Cancro (IG 2018, cod 21790); PRA_2018_27 “Studio del profilo di progressione tumorale nei carcinomi midollari tiroidei e paratiroidei.”